


INTRODUCTION
Broncholith is an uncommon medical problem. When considering broncholiths from a therapeutic standpoint, the role of bronchoscopy has been somewhat controversial. We report here on two cases of successful removal of broncholith that were done without any clinically significant complications by using flexible bronchoscopy.
CASE REPORT
Case 1
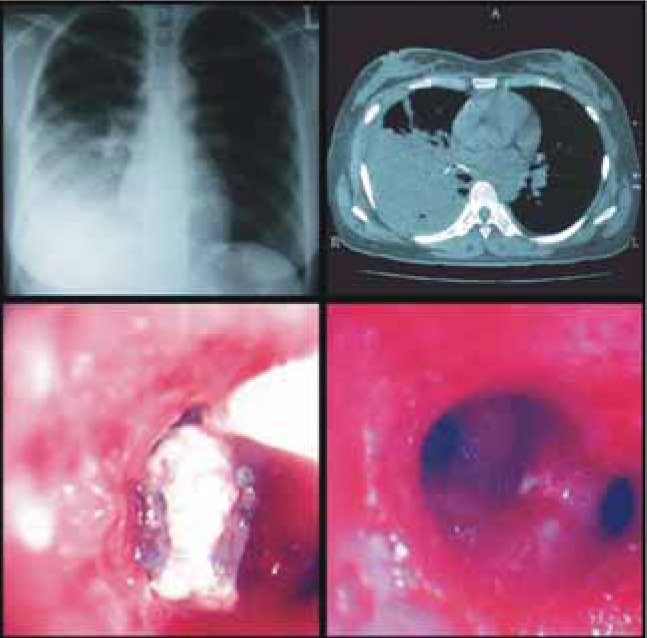
A 65-year-old male patient was admitted to the hospital for the evaluation of atelectasis, and he had a history of recurrent hemoptysis and pneumonia for a few years. The broncholith was impacted at RB9, and there was inflammation of the surrounding mucosa on bronchoscopy. We removed the broncholith using a tripod forcep and the inflammation subsided afterwards (Figure 1).
Case 2
A 37-year-old female patient was referred from a general hospital due to a calcified lymph node from an unknown cause that was discovered on computerized tomography during the treatment for her pneumonia and parapneumonic effusion. Bronchoscopy revealed the impacted broncholith and exudate at the right lower opening. Fungus was cultured from the bronchoaleveolar lavage fluid. We removed the broncholith using a balloon catheter and tripod forcep after antifungal treatment (Figure 2).
DISCUSSION
Broncholiths are calcified peribronchial lymph nodes that encroach upon the adjacent airways and they cause clinical and roentgenographic abnormalities1). Mycobacterial and fungal granulomatous lymphadenitis are the most frequently cited infections that are responsible for tissue calcification, although silicosis is a less commonly associated noninfectious cause. The most common infectious complication resulting from broncholithiasis appears to be bacterial pneumonia that is generally due to airway obstruction by a broncholith and also to the associated airway inflammation and edema. Lung abscesses along with bronchoesophageal and bronchomediastinal fistulas are potentially more serious complications arising from symptomatic broncholithiasis, and these complications are responsible for cases of prolonged or recurrent infection2). In our case, both patients had recurrent and prolonged pneumonia.
Bronchoscopy is considered the most important diagnostic test for broncholithiasis. However, its role in the treatment of broncholithiasis is controverial. Olson and his coworkers3) reported that 100% of their patients with loose (free in the airway) broncholiths underwent flexible and rigid bronchoscopic extraction attempts without severe complications. Massive life-threatening hemoptysis secondary to fistula or rupture of aorta or pulmonary arteries is a possible complication, but generally, massive hemoptysis caused by broncholithiasis is a rare complication3-5).
As compared with the morbidity and mortality associated with surgical intervention, bronchoscopic management appears favorable for patients with loose or partly eroded broncholiths6). Loose, movable broncholiths are especially suitable for removal by bronchoscopic extraction in the clinical setting having capabilities for rigid and flexible bronchoscopy and immediate thoracic surgical support, and after the relation of the broncholith to adjacent vascular structures has been studied by computerized tomography3).

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





