


INTRODUCTION
The main pathogenetic features of Beh├¦et's disease are vascular inflammation and thrombophilia. Clinical presentation is variable and may include: skin manifestations like recurrent oral or genital ulcers as well as, CNS, articular, and ocular signs as described by the international study group of Beh├¦et's disease as the key diagnostic features1). Diverse vasculopathies and thrombophilia of any size and in any vessel, encompass vascular accidents of arterial, venous vasculitis, and thrombosis in Behcet's disease. These findings however, rarely become complicated by vascular stenosis or aneurismal dilatation. Here, we describe a case of Beh├¦et's disease that was complicated by cardiac tamponade with hemorrhagic pericarditis, TTP, DVT, coronary artery stenosis and a coronary artery pseudo aneurysm, the latter of which occurred during disease evolution.
CASE REPORT
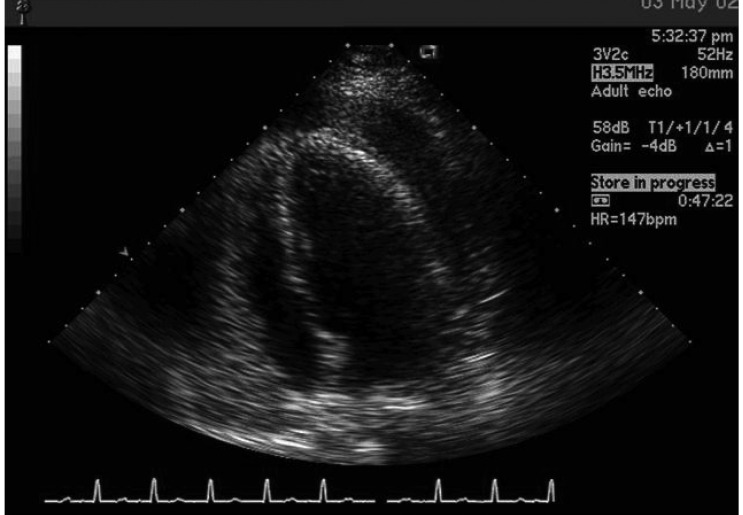
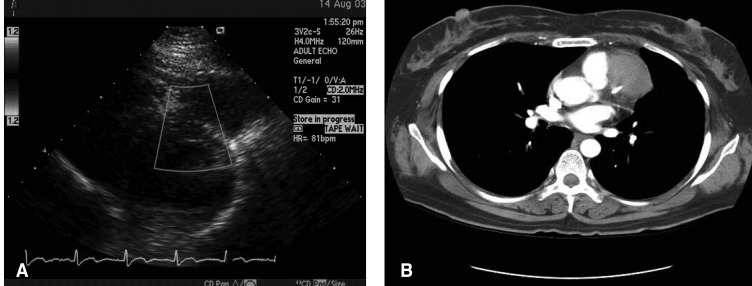
A 37-year-old woman was transferred to our emergency room with the history of syncope. Three days previously, she experienced chest discomfort, dyspnea, palpitations and a low grade fever, but had no relevant past medical history or co-morbidity. At presentation her blood pressure was 80/50 mmHg, pulse rate 76/min, respiratory rate 36/min and body temperature 37.5Ōäā. The physical examination was remarkable for: dyspnea, orthopnea, absence of normal heart sounds, and jugular vein dilatation; Additional tests revealed: low voltage ECG, sinus tachycardia and a large cardiac shadow on X-ray. Laboratory findings showed a pH of 7.37, PaCO2 18.8 mmHg, PaO2 88.5 mmHg, HCO3- 10.8 mmol/L on ABGA, hemoglobin 9.2 g/dL, white blood cell of 12900/┬ĄL, and platelet 476000/┬ĄL on CBC. ANA, rheumatoid factor, and VDRL were all negative and non- reactive. The patient had a suspected cardiac tamponade therefore a transthoracic echocardiography (TTE) was performed immediately and revealed moderate pericardial effusion and a hypokinetic LV at the anterior, anterolateral and apex portions of the heart (Figure 1). Pericardiectomy with a window formation was performed to remove the effusion and hematoma. The drained fluid had a white blood cell 225 (PML 100%), red blood cell 90,000/┬ĄL LDH 1064U/L, and glucose 190 mg/dL; there were no organism on gram stain and culture. A class I cytology, indicating acute and chronic inflammation was revealed. On postoperative day 3, fever, dyspnea, oliguria and mental status changes developed and the patient deteriorated rapidly. A follow-up evaluation showed the serum hemoglobin to be 6.9 g/dL, white blood cell 14900/┬ĄL, platelets 18000/┬ĄL and AST, ALT and CPK of 272, 151, and 247 U/L, respectively. Blood urea nitrogen was 40.6 mg/dL, creatinine 4.9 mg/dL, LDH 2279 U/L, PT 11.6 seconds and aPTT of 32 seconds.
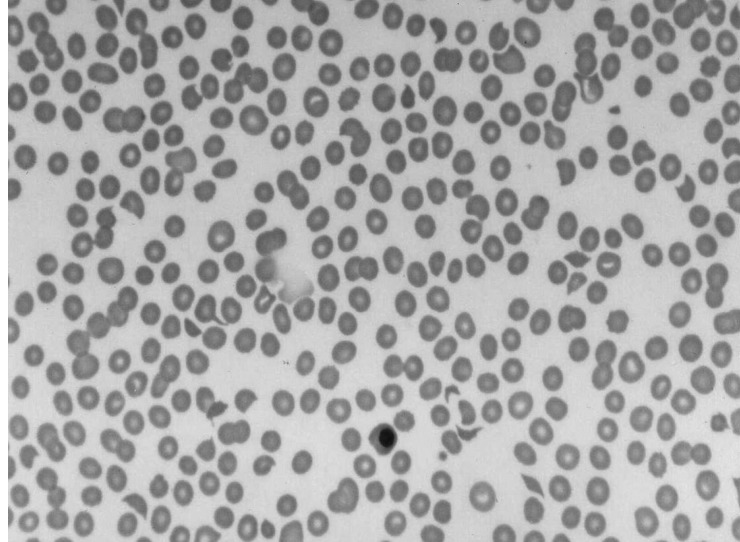
A chest X-ray revealed a ground glass appearance in both lungs. The brain MRI was reported as normal. A peripheral blood smear was remarkable for schistocytosis, anisocytosis, normoblasts and a thrombocytopenia, suggestive of microangiopathic hemolytic anemia (Figure 2). All of these findings were compatible with the diagnosis of thrombotic thrombocytopenic purpura (TTP). Treatment with methylprednisolone pulse therapy was started (1 g/day for 3 days). Investigation for the etiology of TTP revealed that the patient had suffered from severe recurrent oral and genital ulcers. The ulcers were reported to be as frequent as 3 to 4 per month and were exacerbated by menstruation after the age of 20. The patient also reported taking medications intermittently for painful skin indurations and eruptions as well as arthralgia. Considering the clinical symptoms in total the diagnosis, of Behcet's disease complicated by TTP and hemorrhagic pericarditis, was made. Treatment with methylprednisolone pulse therapy resulted in a dramatic response with improvements of the CBC, LFT, azotemia, and improved mental status. The patient went on to fully recover and returned to normal activities of daily living within a few days. Follow-up evaluation with TTE after complete recovery showed a normal right and left ventricular heart function and a minimal pericardial effusion. After discharge, the patient continued taking medication including colchicine 1.2 mg/day and prednisolone 5 mg/day. The patient continued to be followed.
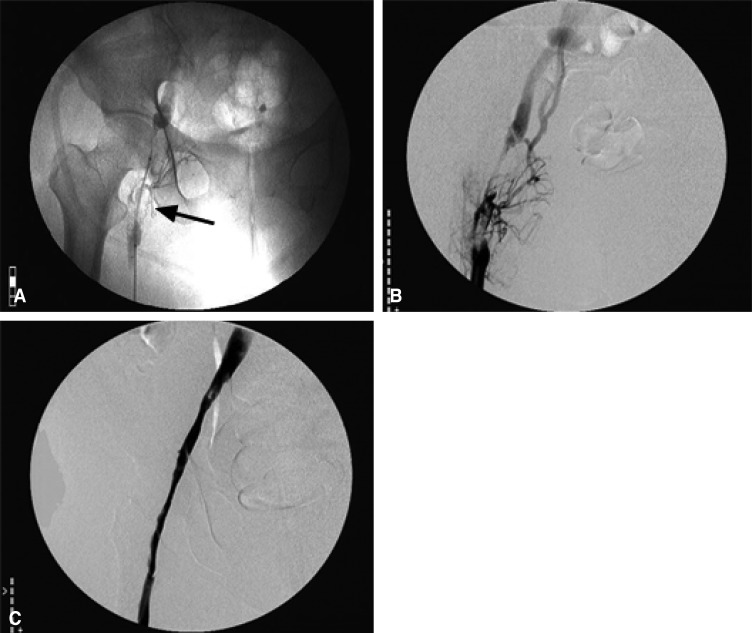
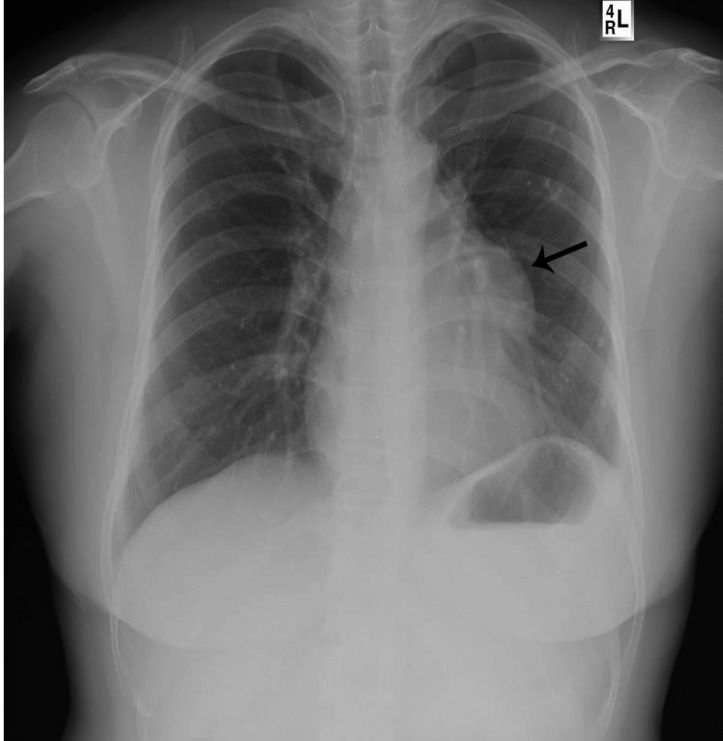
Six months after discharge, the patient required readmission to the hospital. She presented with a sudden onset left leg swelling and pain that was diagnosed as a left proximal femoral vein thrombosis by duplex scan. There were no associated signs or symptoms such as dyspnea or fever. A venogram demonstrated that a filling defect obstructed the left proximal femoral vein. the patient was treated with catheter directed thrombolysis using urokinase, thrombectomy and venoplasty and then started on combination anticoagulation therapy (Figure 3). Six months after maintenance therapy with coumadin, colchicines, and sulfasalazine was started, a homogenous soft tissue mass was found, incidentally, on routine laboratory and radiologic follow up. The soft tissue density was attached to the left perihilar area by the pulmonary conus (Figure 4). The laboratory tests showed a hemoglobin of 11.1 g/dL, platelet 324000/┬ĄL, WBC 6000/┬ĄL, ESR 39 mm/H, CRP 1.59 mg/dL, albumin 4.5 g/dL, LDH 503 U/L, BUN 11.8 mg/dL, creatinine 1.0 mg/dL, PT 29.7 second, INR 2.95.
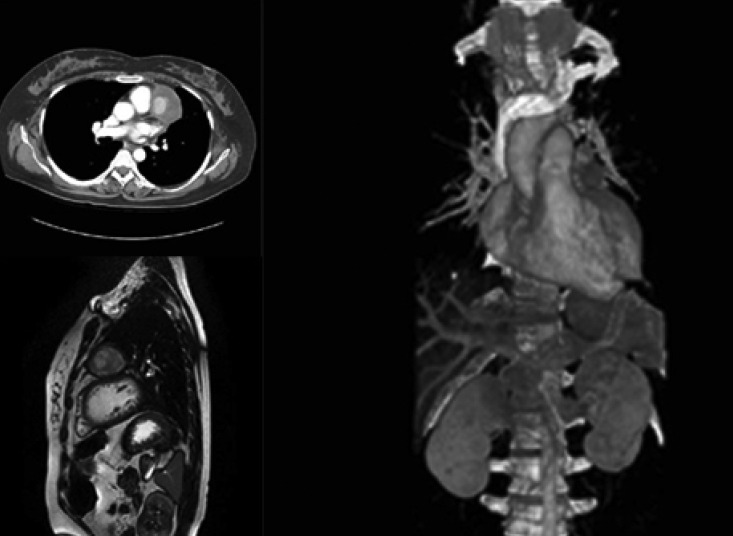
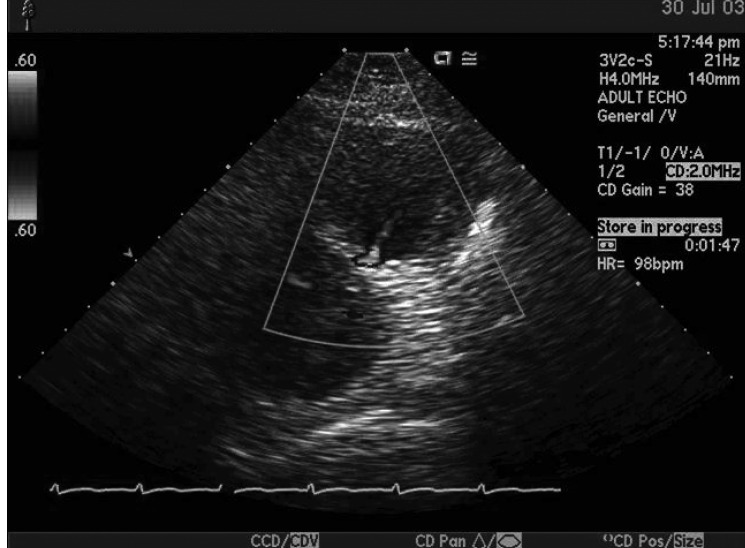
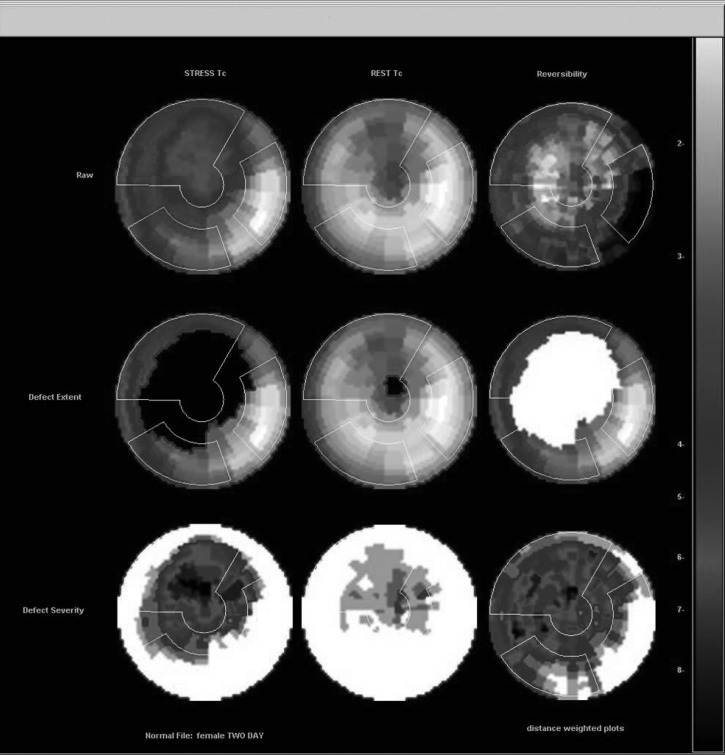
Chest CT angiography and cardiac MRI revealed a 5x5cm sized round aneurysmal sac between the left atrium and left ventricle adjacent to the proximal pulmonary artery, but no definite stalk from the origin could be found (Figure 5). A doppler echocardiography demonstrated holosystolic ejection flow from the surface of the left ventricle (Figure 6). Despite the fact that the origin of aneurysmal stalk could not be identified, the pressure gradient calculated by the color doppler flow from the aneurysmal stalk to lumen was about 9 mmHg. The dilated vascular sac appeared to be a pseudo aneurysm with a coronary artery origin. A Tc99m sestamibi scan was performed to investigate the possibility of myocardial ischemia. The scan revealed a reversible perfusion defect on the antero-septal wall (Figure 7). Subsequent coronary angiography allowed us to confirm the diagnosis of a pseudo aneurysm from the mid-left anterior descending artery (LAD), which interrupted distal flow by creating indentations and diffuse stenotic lesions along the whole length of the right coronary artery (RCA). In addition, a well developed collateral circulation was observed from the LAD and the left circumflex artery (LCX). An emergency operation was planned for aneurysmal resection and coronary artery bypass grafting (CABG). However, because of the size and thus the risk of rupture, we opted instead for balloon angioplasty with a U-pass and graft stent. Implantation proceeded using a Graftmaster 3.0├Ś19 mm at the mid LAD the origin of pseudo aneurysm (Figure 8). Because of the compromised distal flow of the RCA, the LAD would be of no advantage to the outcome of the CABG. If packed completely, it was expected that the aneurysmal sac would not grow any more and would regress by resorption and fibrosis. The administration of high dose glucocorticoid therapy (prednisolone 1 mg/kg/day) with azathioprine (150 mg/day) in addition to the mechanical intervention were both highly effective management as demonstrated by a follow-up TTE and coronary angiography which showed no further diversion of flow from the LAD and regression of the aneurysmal size to 3.9├Ś3.8 cm from 5├Ś5 cm Initially. and a preserved heart function (LVEF 60%) (Figure 9). Six months after discharge, the patient was asymptomatic and only a vestige of the aneurysm was evident by routine chest X-ray (Figure 10).
DISCUSSION
Beh├¦et's disease has a heterogenous presentation with variable symptoms including: mucocutaneous, ophthalmic, neurological, cardiovascular, pulmonary, gastrointestinal, urogenital and musculoskeletal involvement. The prevalence of vascular involvement in Beh├¦et's disease has been reported to range from 7.7 to 60.6%. Kabbaj et al reported 85% venous involvement, 10% arterial and 5% combined arterial and venous involvement2-4). Deep vein thrombosis, has been found to occur earlier in the course of disease than arterial disease, which develops after a median of 7 years. Deep vein thrombosis occurs primarily in the lower extremities, but involvement is possible at any site5).
Although the pathogenesis of thrombotic events in Beh├¦et's disease has not been elucidated, microscopic examinations of veins and arteries involved have demonstrated vasculitis. It has been postulated that a genetic predisposition to certain agents might result in damage and/or functional impairment of the vascular wall and endothelium of vessels. This observed damage may be due to impaired prostacyclin production, significantly higher levels of plasma endothelin-1,2, von Willebrad factor, or anti-endothelial cell antibodies. The role of thrombophilia in Beh├¦et's disease with protein C or S, or antithrombin deficiency, in the presence of antiphospholipid antibodies or factor V Leiden have been investigated but results have been conflicting6, 7).
Cardiac involvement in Beh├¦et's disease is rare, but pericarditis, myocardial infarction, coronary arteritis, valvular regurgitation (especially aortic valve regurgitation), and an impaired conduction abnormalities have been reported8). In our case, hemorrhagic pericarditis was identified as a presenting abnormality with no other identifiable sign or symptom.
Jabr et al. reported on the possibility of a link between Beh├¦et's disease and TTP and came to the conclusion that TTP had developed due to some other cause, e.g., the drugs administered or infection. Others reported hemolytic uremic syndrome (HUS) in patients with Beh├¦et's disease treated with cyclosporin9-11). In our case, the patient had a history of prior surgery under general anesthesia, along with exposure to several medications (mainly antibiotics) before the onset of TTP. However, there were no definite signs of infection either physiologically or in culture. Nevertheless, she recovered completely and dramatically on high doses of glucocorticoid and conservative maintenance of antibiotics.
The prevalence of arterial occlusion in Beh├¦et's disease has been reported to range from 0.5 to 1.5% and can involve the coronary, subclavian, carotid, renal, pulmonary, or any peripheral artery and cause myocardial infarction, pulseless disease, stroke, hypertension, respiratory failure, or intermittent claudication6). Aneurysm formation may coexist with arterial thrombosis. Common sites are the aorta and pulmonary, femoral, popliteal, subclavian and common carotid arteries, but any artery can be affected6, 12). It is significant that aneurysmal rupture is the leading cause of death in Behcet's disease patients6), and thus it should be deliberate to counter thrombophilia with anticoagulant therapy despite the presence of the thrombotic event.
The presence of an arterial pseudo aneurysm generally requires surgical repair with aneurysmectomy. Degeneration at the anastomotic site and thrombosis are not rare complications in the postoperative period12). Ozeren et al. reported a pseudo aneurysm originating from the proximal left anterior descending artery and a true aneurysm of the right coronary artery with fistulization to the right atrium. They surgically corrected the pseudo aneurysm under cardiopulmonary bypass support by closing the neck of the false aneurysm using an endo-aneurysmal approach with a Gore-Tex patch13). In our case, we adopted the approach of a stent graft implantation rather than surgical removal.
Several studies have been undertaken to examine graft stent implantation in Beh├¦et's disease. However, there is no prior report of the involvement of the coronary artery. The main advantages of endovascular treatment are lower mortality rates, e.g., 0.6% to 3.5%, even in high risk groups, and higher success rates (97%). Other advantages are shorter hospital stay and a shorter convalescence period before returning to normal life. In addition, the avoidance of general anesthesia and surgical dissection, this is especially important in Beh├¦et's disease because of its propensity for healing impairment12, 14, 15).
Here, we report on a Behcet's disease patient with rare complications related to the cardiovascular system during disease evolution., These problems included: hemorrhagic pericarditis, TTP, DVT, coronary artery stenosis, and a coronary artery pseudo aneurysm. The coronary pseudo aneurysm was treated with a combined approach of immunosuppression and endovascular non-surgical intervention.
Cardiovascular complications of Bechet's disease must be treated with aggressive immunosuppression using a combination of corticosteroid and a cytotoxic agents. Anticoagulants and antiplatelet agents are judiciously required to address the risk of hemorrhage during the vasculitic process and that of aneurysmal rupture in cases of thrombotic complications6, 16). In patients with graft stent implantation, subsequent vascular thromboses are possible. For these cases some recommend anticoagulant therapy although this increases the risk of pseudo aneurysm formation13). As evidenced by the present case, anticoagulants like coumadin may cause aneurysm formation and growth in Beh├¦et's disease. Therefore, for patients with Beh├¦et's disease the early detection of cardiovascular complications is of cardinal importance as they are the leading cause of mortality. We recommend that physicians pay close attention to even minor complaints and that physical changes be scrutinized and that regular screening protocols are established for the early detection of cardiovascular complications in Beh├¦et's disease.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





