


INTRODUCTION
Age-linked epidemiology of disease generally differs in prevalence, incidence and severity at presentation. The causes and outcome of coronary artery disease differ by age1). Younger patients <40 with an acute myocardial infarction have different clinical characteristics and a different prognosis than older patients2). Patients older than 70 have been shown to be at risk for overt coronary artery disease and for exercise- induced silent ischemia based on age alone even when asymptomatic3). Many risk factors have been identified for the development of ischemic heart disease (IHD) in elderly patients. In addition, the prevalence of IHD has been closely associated with sociodemographic, biological, psychological, and behavioral risk factors4). To date there is only limited information available on the clinical characteristics of ischemic heart disease in different age groups in the Korean population.
The KCAR (Korean Coronary Artery disease Registry) Study is a registry study initiated in 1999 to investigate the clinical characteristics of IHD in Korea. The purpose of the present study was to assess the differences in epidemiology, clinical characteristics and treatment modalities for IHD in Koreans based on age.
MATERIALS AND METHODS
Subjects
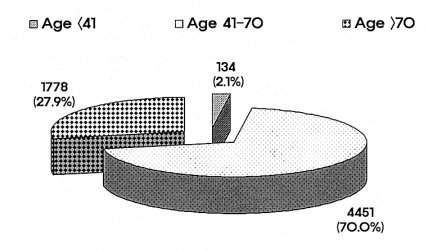
This study was a prospective, multicenter registry-based study performed from March 1999 to December 2005. The KCAR (Korean Coronary Artery disease Registry) Study was initiated in 1999 to determine and record the clinical characteristics of ischemic heart disease in the Korean population. Nationwide, seven university hospitals in Korea (Yeungnam University Hospital, Daegu: Chungnam University Hospital, Daejeon: Kyunghee University Hospital, Seoul: Chungbuk University Hospital, Cheongju: Chonnam University Hospital, Gwangju: Hanrim University Hospital, Seoul: Donga University Hospital, Busan) participated in this study. Research coordinators registered all patients, evaluated at the cardiac catheterization laboratory for the purpose of assessment or treatment of ischemic heart disease. This registry included all consecutive patients who had coronary angiography with one of the following: 1) evidence of myocardial ischemia on exercise electrocardiography (ECG) and myocardial perfusion scanning ; 2) induced coronary spasm with the ergonovine or acetylcholine provocation test 3) clinical evidence of myocardial infarction based on clinical symptoms, cardiac enzymes and ECG. The different patient diagnoses included syndrome X, variant angina, stable angina, unstable angina, ST-elevated MI (STEMI), and non-ST elevated MI (NSTEMI). All diagnoses were determined by expert consensus after review of the available clinical data. Patients with atypical chest pain and normal angiographic findings, without evidence of myocardial ischemia, were excluded from this study. On the day after admission, a detailed medical history was obtained from subjects and doctors and study coordinators performed a physical examination. The physical examination included height and weight recorded according to standard methods; the body mass index was calculated by weight (kg)/height (m)2. The total serum cholesterol and triglyceride levels were measured by enzymatic calorimetric testing after overnight fasting on the day after admission. The low-density lipoprotein cholesterol was calculated using the Friedewald formula. A coordinator at each hospital entered data collected from each institution into a standardized computerized database provided by the KCAR committee. The data coordinators attended meetings four times a year; at the meetings, the study protocol was reviewed and discussed. From March 1999 to December 2005, 6,549 patients were registered into the database. All patients were divided into three groups according to age: young patients, Ōēż40 (n=134), middle-aged patients, 41-70 (n=4451) and older patients, Ōēź71 (n=1778). We compared the baseline clinical characteristics and angiographic findings among these groups.
Definitions
Based on the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC) VII guidelines, hypertension was defined as known hypertension or a blood pressure (BP) Ōēź140/90 mmHg5). The diagnosis of diabetes mellitus was based on fasting plasma glucose levels Ōēź126 mg per dL (7.0 mmol per L) or two-hour postprandial plasma glucose (2hrPPG) readings Ōēź200 mg per dL (11.1 mmol per L)6). The metabolic syndrome was defined according to a modification of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III)7). Since the cutoff values for the definition of obesity in Asian populations have been revised, the criteria for the metabolic syndrome was modified8). The metabolic syndrome was diagnosed if three or more of the following were present: (a) Obesity defined by a body mass index >25 kg/m2 (b) hypertriglyceridemia if the TG Ōēź150 mg/dL (c) low HDL-C : HDL-C<40 mg/dL in men or <50 mg/dL in women (d) hypertension as known hypertension or a BP Ōēź130/85 mmHg and (e) dysglycemia was defined as known diabetes (DM) or a fasting plasma glucose Ōēź110 mg/dL. Cardiac syndrome X was present in patients with typical exertional chest pain, a positive response to stress testing and normal coronary angiograms.
RESULTS
Clinical characteristics
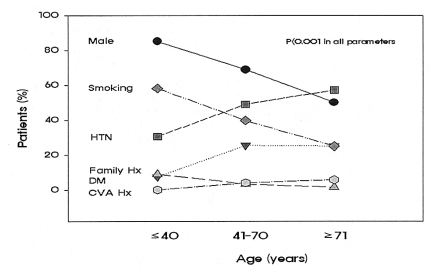
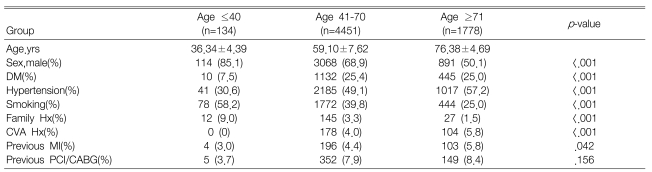
Of the 6,349 patients enrolled: 70% of the patients were in the 41-70 age group 2.1% in the Ōēż40 age group, and 27.9% in the Ōēź71 age group (Figure 1). The Ōēż40 age group had a higher number of males than the 41-70 and Ōēź71 age groups (85.1%, 68.9% and 50.1%, respectively, p<0.01). Furthermore, the 40 age group had a higher frequency of smoking and family history of ischemic heart disease than did the other groups (p<0.01, respectively). However, the over 41 age groups had a higher frequency of age-related risk factors such as diabetes mellitus, hypertension and stroke than did the Ōēż40 age group (p<0.01, respectively) (Table 1) (Figure 2).
Lipid profiles and metabolic syndrome
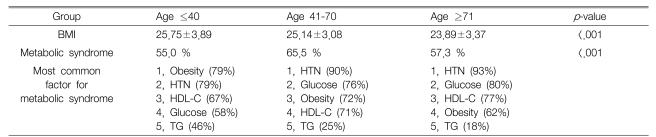
Hypercholesterolemia defined as a serum total cholesterol 200 mg/dL or more was more common in the Ōēż40 age group than in the 41-70 and Ōēź71 age groups (49.4%, 37.3% and 31.5%, respectively, p<0.01). The levels of total cholesterol, triglycerides and LDL-C were significantly higher in younger patients than in the older patients. However, the HDL-C was not significantly different among the three groups (Table 2). To determine the frequency and contributing factors for the metabolic syndrome, all risk factors were identified and compared in the different groups; the metabolic syndrome for the total study population was identified in 55% of the Ōēż40, 66% of the 41-70 and 57% of the Ōēź71. The highest prevalence of the metabolic syndrome was in the middle age group (p<0.001) (Table 3). The frequency of contributing factors for the metabolic syndrome, according to age group was analyzed. In the Ōēż40 age group, obesity (79%) and hypertension (79%) were the most common contributing factors identified for the metabolic syndrome; hypertension and high fasting glucose were the most common contributing factors in the older age groups (Table 3).
Coronary angiographic findings, clinical presentation and treatment modalities
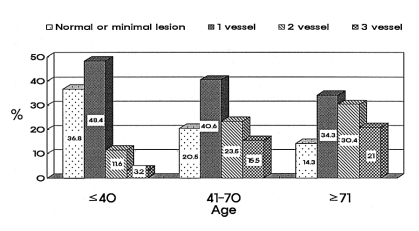
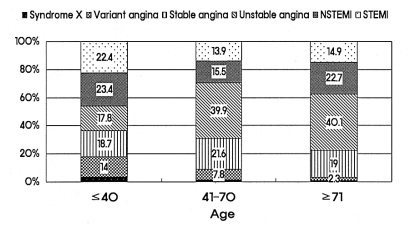
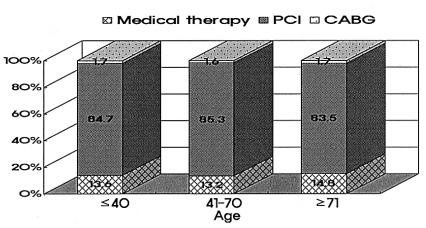
Coronary angiography showed normal or minimal stenosis in 37% and one vessel disease in 48% in the Ōēż40 age group. The prevalence of multivessel disease was dramatically increased with advancing age; 51% of the patients had more than two vessel disease in the Ōēź71 age group (Figure 3). Young patients frequently presented with a myocardial infarction (MI), non-ST elevated MI (23%) and ST elevated MI (22%). However, older patients were most frequently admitted with unstable or stable angina (Figure 4). The treatment modalities were not different among the different age groups. About 13~14% of patients were treated by medication only. Percutaneous coronary intervention (PCI) was performed in more than 80% of the patients in each group. Coronary artery bypass graft surgery (CABG) was performed in 1.7% of all patients (Figure 5).
DISCUSSION
In this multicenter registry based study of 6,549 patients hospitalized for ischemic heart disease, we found age-related variations in epidemiologic characteristics and clinical presentation. This is the first large scale study evaluating the epidemiologic features of ischemic heart disease in the Korean population.
The age group of 65 and over is currently the fastest growing age group in Korea; ischemic heart disease is an age-related disease and its prevalence is increasing with the aging population. Race and socioeconomic status are also associated with the prevalence and clinical outcome of ischemic heart disease9). The risk factors associated with atherosclerotic disease are different in elderly patients when compared to younger patients10). However, currently we do not have sufficient data to assess the specific risk factors contributing to the development of ischemic heart disease in the Korean population. In this study, we analyzed epidemiologic and clinical data from patients with ischemic heart disease who were treated at seven Korean university hospitals.
We analyzed epidemiologic variables in three different age groups. For the younger patients we found a higher frequency of males than in the older patients; the gender differences equalized after 70, similar to the data from Western countries11, 12). The menopausal age of Korean women is on average 4913). This suggests that the antiatherogenic effects associated with female gender are no longer present by about 20 years after menopause. The smoking rate was 58% in the younger age group, and it dropped to 25% in the old patient group. Therefore, smoking is still a major risk factor for coronary artery disease in young Korean males. However, the older group showed a higher prevalence of age related diseases such as hypertension and diabetes.
As for the lipid profiles, the younger patients had dyslipidemia more commonly than the older patients did. This may have been related to the higher incidence of obesity in the younger patients. This also suggests the possibility of a genetic predisposition related to the metabolic abnormalities observed in younger patients.
Recently, the clinical significance of the metabolic syndrome for the development of cardiovascular disease has been emphasized; the prevalence of metabolic components such as high blood sugar, obesity and hypertension are increasing in Korea. The incidence of the metabolic syndrome depends on the definition used14, 15). In this study, the definition introduced by the National Cholesterol Education Program (NCEP) Expert Panel was used16). The definition of obesity was modified according to the Asian criteria developed for the body mass index (BMI) Ōēź25 kg/m2 8). It is well known that the prevalence of the metabolic syndrome, in the general population, varies based on race, gender and geographic region. The prevalence of the metabolic syndrome, in Korea, using the ATP III-BMI25 definition was reported to be 13%, based on Korean health data17), which included 20.1% men and 23.9% women from the Korean nutritional health survey18). In this study, the prevalence of the different components of the metabolic syndrome differed by age group. For the less than 40 group, obesity was the most common contributing factor. However, for the older groups age-related factors such as hypertension and diabetes were the most frequent factors.
The angiographic severity of coronary artery disease appears to differ in younger patients compared to the older patients; the younger patients showed a preponderance of normal findings, minimal lesions or single-vessel disease. For the Ōēź71 age group there was a significantly higher prevalence of three-vessel disease, up to 21%.
Recently, with improvements in coronary intervention and surgical skills, treatment is available at any age. However, our data showed that older patients were less likely to undergo percutaneous coronary intervention or bypass surgery during their hospital admission1, 19); although the medical treatment options were similar for the different age groups. In routine clinical practice in Korea, about 84% of patients with ischemic heart disease and significant coronary artery stenosis have percutaneous coronary intervention.
The limitations of this study included the following: not all clinical parameters were routinely noted and the treating physician recorded most of the diagnostic criteria; since we intended to determine general patient patterns in Korea, site selection was not random.
In conclusion, the KCAR study provides important information on age-related trends in the epidemiologic characteristics of ischemic heart disease in Korea. Coronary artery disease in younger adults showed different demographic characteristics and different clinical presentation compared to older patients.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





