


INTRODUCTION
Capecitabine (Xeloda) is an oral fluoropyrimidine carbamate, which is converted to its only active metabolite, FU, by thymidine phosphorylase. Higher levels of this enzyme are found in several tumors, as well as the liver, compared with normal healthy tissue1-3). The localization of this enzyme to liver and tumor tissues allows for targeted intratumoral release of FU, with subsequently less systemic toxicity than with i.v. FU, as documented in clinical trials3-5).
The most common dose-limiting adverse effects associated with capecitabine monotherapy are hyperbilirubinemia, diarrhea and hand foot mouth disease (HFS). Myelosuppression, fatigue and weakness, abdominal pain and nausea have also been reported as potential side effects6).
HFS is a cutaneous adverse effect, also referred to as palmar-plantar erythrodysesthesia. It has been clinically described as a condition affecting the palms of the hands and the soles of the feet. Patients with HFS experience various degrees of dysesthesia, painful erythema and edema, which may be followed by dry or moist desquamation of the involved skin. In more severe cases, the symptoms interfere with the normal activities of daily living. A grading system for HFS has been developed, incorporating both clinical and functional domains7).
Drugs have been associated with HFS, including 5-FU, capecitabine, cytarabine, doxorubicin, epirubicin, fluorodeoxyuridine (FUDR), hydroxyurea, mercaptopurine, cyclophosphamide, docelaxel and vinorelbine8).
Herein is report a case of HFS, with scleroderma-like changes induced by capecitabine.
CASE REPORT
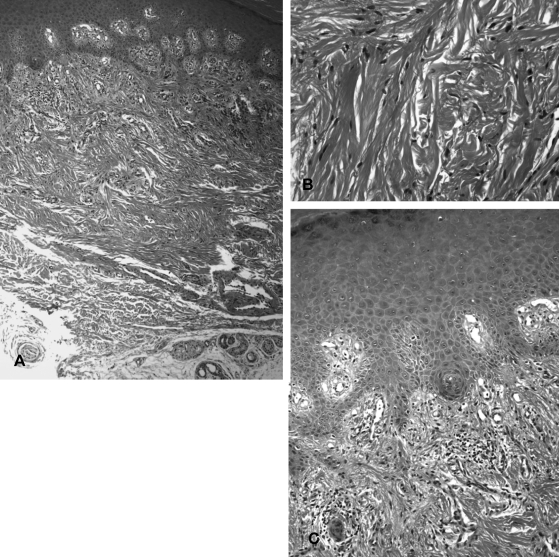
A 70-year old male, after undergoing a palliative gastrojejunostomy in December 2003, was diagnosed with a stage IV signet ring cell carcinoma of the stomach. He received palliative chemotherapy, with 5-FU and taxotere for 6 courses, 5-FU, irinotecan and leukovorin for 3 courses, and 5-FU and heptaplatin for 3 courses. In December 2004, computed tomography (CT) scans revealed a stable disease with peritoneal seeding. The patient then received oral capecitabine (Xeloda) chemotherapy, at a daily dosage of 2500 mg/m2, in divided doses. Each cycle of therapy consisted of 2 weeks of capecitabine administration, followed by a 1-week resting period. After the fourth course, the clinician noted desquamation and brownish to black hyperpigmentation on the palms, fingers and soles. The patient also complained of mild pain in his palms and soles, but denied any paresthesia. Because the patient's only concurrent medications were azintamide, almagate and metoclopramide HCl, the HFS was attributed to capecitabine. He was instructed to apply lotion to his hands and feet in the absence of dosage reduction or cessation of the drug. After the 16th course, the clinician noted a scleroderma-like change with hyperpigmentation of the fingers and palms (Figure 1). The patient experienced mild pain and discomfort when using his hands, which interfered with hand grasping. A punch biopsy of the skin from the finger was performed (Figure 2). Histologically, there were foci of mild perivascular infiltration of chronic inflammatory cells, with some scattered pigmentladen macrophages in the superficial dermis. Dermal sclerosis, with thickening of collagen bundles, was noted throughout the reticular dermis. In the basal layer of the epidermis, mild spongiosis with exocytosis of a few small lymphocytes was noted. The search for antinuclear, anticentromere, anti-Scl 70 antibodies and rheumatoid factor was negative. The next round of chemotherapy was stopped in January 2006. The scleroderma-like changes gradually improved within the subsequent 3 to 4 months of capecitabine cessation.
DISCUSSION
5-FU has been known to cause HFS since the association was first described by Lokich and Moore in 19849). Compared with bolus infusion, continuous infusion of 5-FU is associated with a higher incidence of this side effect10). In addition, continued prolonged exposure to 5-FU, provided by oral administration of capecitabine, leads to rates of HFS as high as 68%7).
The manifestations of HFS are classified into 3 grades according to their severity11). Grade 1 consists of erythema of the lateral aspects of the fingers that progress to the thenar and hypothenar eminences, with swelling, numbness, dysesthesia/paresthesia and tingling, especially over the pads of the distal phalanges. The same manifestations occur on the soles, but less frequently on the dorsal aspects of the hands and feet. Grade 2 is a progression of grade-2 manifestations, where pain and discomfort affect the daily activities of the patient. Grade 3 is the superimposition of blistering, moist desquamation and ulceration, coupled with severe pain.
Of the adverse reactions of capecitabine HFS is listed first in the drug's product information provided by the manufacturer11), with cessation of the medication recommended for grades 2 and 3 HFS until the event is resolves or decreases in intensity.
Recognition and identification of the signs and symptoms of grade 1 HFS in patient receiving capecitabine are important to avoid progression to grade 2 or to the more debilitating grade 3.
Most importantly; however, the manifestations of HFS in patients are different from those described in the literature. First, our developed a progressive hyperpigmentation of his palms, fingers and soles rather than erythema. Second, there was a concomitant gradual thickening of the skin of the palms, fingers and soles, which lead to stiffness of the hands and feet.
In another case report12), Parthas, et al observed that the administration of capecitabine lead to hyperpigmentation of the palms and soles, followed by a distinct keratoderma-like thickening in 3 black patients. They suggested that the definitions for grades 1, 2 and 3 HFS for black patients should be revised. We also feel that the definition of grade 1 HFS should be revised to include hyperpigmentation of the palms, fingers and soles, either with or without erythema, and that progression to grade 2 HFS should consist of keratoderma-like thickening, as in the report of Parthas, et al.
The pathophysiology of HFS is largely unknown, with only a few cases having been investigated via biopsies. Pathological changes described thus far include, vacuolar degeneration of basal keratinocytes, dermal perivascular lymphocytic infiltration, apoptotic keratinocytes and dermal edema13, 14). In this case, dermal sclerosis, with thickening of collagen bundles, was noted throughout the reticular dermis.
In a case report of HFS in black patients12), the result of a punch biopsy showed vacuolar degeneration of the basal layer of the epidermis, with cellular enlargement, spongiosis, mild exocytosis of small lymphocytes and marked hyperkeratosis. The dermis showed a mild superficial perivascular lymphocytic infiltrate.
We report a case of HFS, with scleroderma-like change, which was apparently induced by capecitabine. More research will be required to look at the true incidence of HFS from a variety of causes. Continued research may lead to the discovery of more effective strategies for the prevention and treatment of this complication of chemotherapy, and allow a better understanding of the biology and pathophysiology of fluoropyrimidine.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





