


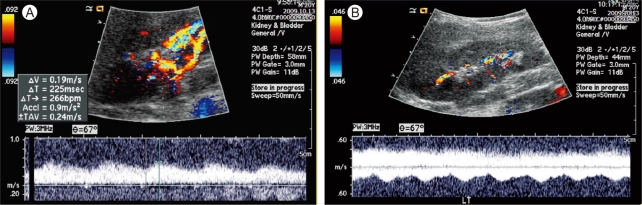
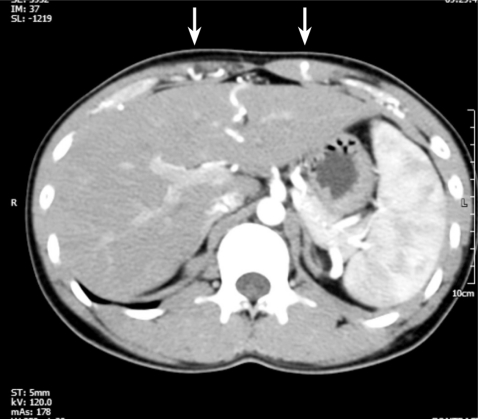
A 21-year-old male with secondary hypertension was referred to our facility by a general physician. The patient had no family history or risk factors for hypertension. During the physical examination the patient's blood pressure (BP) measured 190/110 in both arms and no cardiac murmur or bruit was detected. Renal Doppler sonography was performed to identify the potential cause of secondary hypertension, specifically renal artery stenosis. Tardus-parvus pulse waves were noted in both renal intra-arteries (Fig. 1A and 1B); however, a subsequent abdominal computed tomography (CT) did not show any evidence of renal artery stenosis and both adrenal glands looked normal. There was a noted tortuous and engorged superior-epigastric artery along the abdominal wall (Fig. 2).
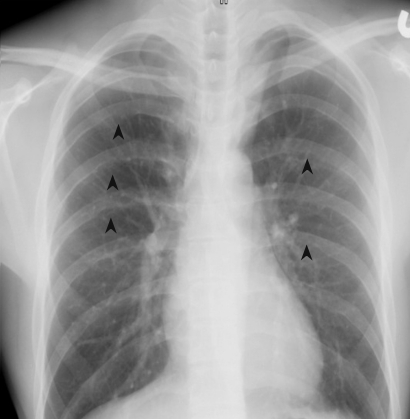
A chest CT was performed to evaluate supra-diaphragmatic vessel abnormalities. The CT revealed a stenotic lesion in the isthmus of the aorta (Fig. 3). After making a diagnosis, multiple rib notchings were found on a chest X-ray (Fig. 4). The patient was transferred to another university hospital for surgical treatment.
Coarctation of the aorta (COA) is a congenital malformation, which can cause systemic hypertension and subsequent complications. Because hypertension caused by COA tends to be resistant to medical therapy, early detection and surgical correction are important. Although discrepancies between arm and leg BP and the presence of bruits due to narrowing lesions can aid in the diagnosis of COA, sometimes these signs are not obvious or can be overlooked.
Renal Doppler sonography is a useful and frequently used tool to evaluate secondary hypertension. When bilateral tardus-parvus wave patterns are detected, bilateral renal artery stenosis, aortic stenosis, and COA should be considered. To differentiate between COA and bilateral renal artery stenosis, the pulse wave of the aorta should be checked, which is superior to the renal artery. If the aortic pulse wave also shows tardus-parvus patterns, it can either be COA or AS [1]. Additionally, engorged collateral circulations, such as in the internal thoracic artery, intercostal artery, or superior epigastric artery, can help in the diagnosis of COA [2].

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





