


INTRODUCTION
Familial history (FHx) has long been considered a major risk factor for coronary heart disease (CHD). FHx was emphasized as a major nonmodifiable risk factor from the National Cholesterol Education Program Adult Treatment Panel (NCEP-ATP) III guidelines [1]. Other major risk factors for CHD, such as old age, renal insufficiency, hypertension, and diabetes mellitus (DM), were reported as predictors of mortality in patients with CHD in previous studies [2-5]. However, the prognostic implication of FHx in patients with CHD has not been studied sufficiently. There were three studies insisted on negative prognostic implication of FHx, which studies had the limitation of small population [6-8]. Another study insisted that FHx was related to better prognosis in patients with first-onset acute myocardial infarction (AMI) [9]. Those studies were from about 10 years ago when revascularization using drug eluting stents was not common. Furthermore, those studies did not consider sufficiently clinical variables, such as therapeutic strategies, which have developed continuously in recent years.
This aim of this study was to reveal the prognostic implication of FHx in the setting of secondary prevention and to evaluate the impact of FHx on disease presentation in patients with first-onset AMI in the current clinical environment. As part of the Korea AMI Registry (KAMIR) study, we focused on the prognostic implication of FHx in a Korean population.
METHODS
Study population
KAMIR is a prospective, multicenter, online national survey designed to reflect the clinical features, and prognosis of AMI in the Korean population with support from the Korean Circulation Society. KAMIR was launched in 2005 with a nationwide effort to collect data from patients with AMI admitted to 49 major cardiac centers capable of primary percutaneous coronary intervention (PCI) in Korea.
Data of 11,612 patients (8,132 males [70%], age 62.7 ± 12.6 years) who were enrolled in KAMIR between November 2005 and June 2008 were used in this study. Patients suffering from ST-segment elevation myocardial infarction (STEMI) and non-ST segment elevation myocardial infarction (NSTEMI) were enrolled. Diagnosis with STEMI was decided by new or presumed new ST-segment elevation of ≥ 2 mm in more than two precordial leads or ≥ 1 mm in more than two limb leads or new left bundle-branch block on the index or subsequent 12-lead electrocardiogram with positive cardiac biochemical marker of necrosis (creatine kinase-MB, troponin I, or T). Patients who were diagnosed with CHD before study enrollment were excluded. Patients younger than 30 years were also excluded because of the possibility of hereditary disorders, congenital anomalies, or vasculitis such as Kawasaki disease. FHx was defined as a first degree male relative with CHD under 55 years or a first degree female relative with CHD under 65 years. Patients with and without FHx are referred to as FHx+ and FHx-, respectively.
Past medical history, including medication use, was reviewed from medical records or depended on patient-reported information if no medical record was accessible. Nonresponses or "unknown" answers were considered as "no."
Initial therapeutic strategy, including PCI, thrombolysis, or conservative management and medication, was decided by the cardiologist, according to the American College of Cardiology and the American Heart Association guidelines for the management of patients with acute coronary syndrome.
Study endpoints
The primary endpoint was cardiac death and the composite major adverse cardiac event (MACE), including cardiac death, nonfatal myocardial infarction (MI), and revascularization (repeated PCI or coronary artery bypass graft after index admission) within 1 year from index admission. All deaths were considered as cardiac deaths unless a noncardiac cause of death was confirmed.
Patients were informed to visit the outpatient clinic of the cardiology department after 1 month from discharge and then every 6 months after the PCI procedure, or whenever angina-like symptoms occurred.
Statistical analysis
Data are expressed as total numbers and proportion (%) or means ± SD. Nonparametric Mann-Whitney U tests were used to compare the median follow-up periods for FHx+ and FHx- patients. Differences in variables between two groups were analyzed using the chi-squared test or Fisher exact test for categorical variables or by the two-tailed unpaired t test for continuous variables to compare baseline clinical and angiographic characteristics. The Cox proportional hazard regression model was used to analyze the prognostic implication of FHx for mortality or composite MACEs. In model 1, the analysis used covariates including age, gender, BMI, and conventional risk factors, including hypertension, DM, dyslipidemia, and current smoking. Model 2 included left ventricular ejection fraction (LVEF) in addition to the covariates in model 1 to reflect severity of infarction and/or baseline cardiac function at index admission. Model 3 included estimated glomerular filtration rate (eGFR), calculated from serum creatinine levels using the prediction equation from the Modification of Diet in Renal Disease Study Group [10] in addition to the covariates in model 2 because renal dysfunction was also assessed as an independent prognostic factor in previous studies [11,12]. All statistical procedures were performed using the PASW software version 18.0 (IBM Co., Armonk, NY, USA).
RESULTS
Baseline characteristics and laboratory findings
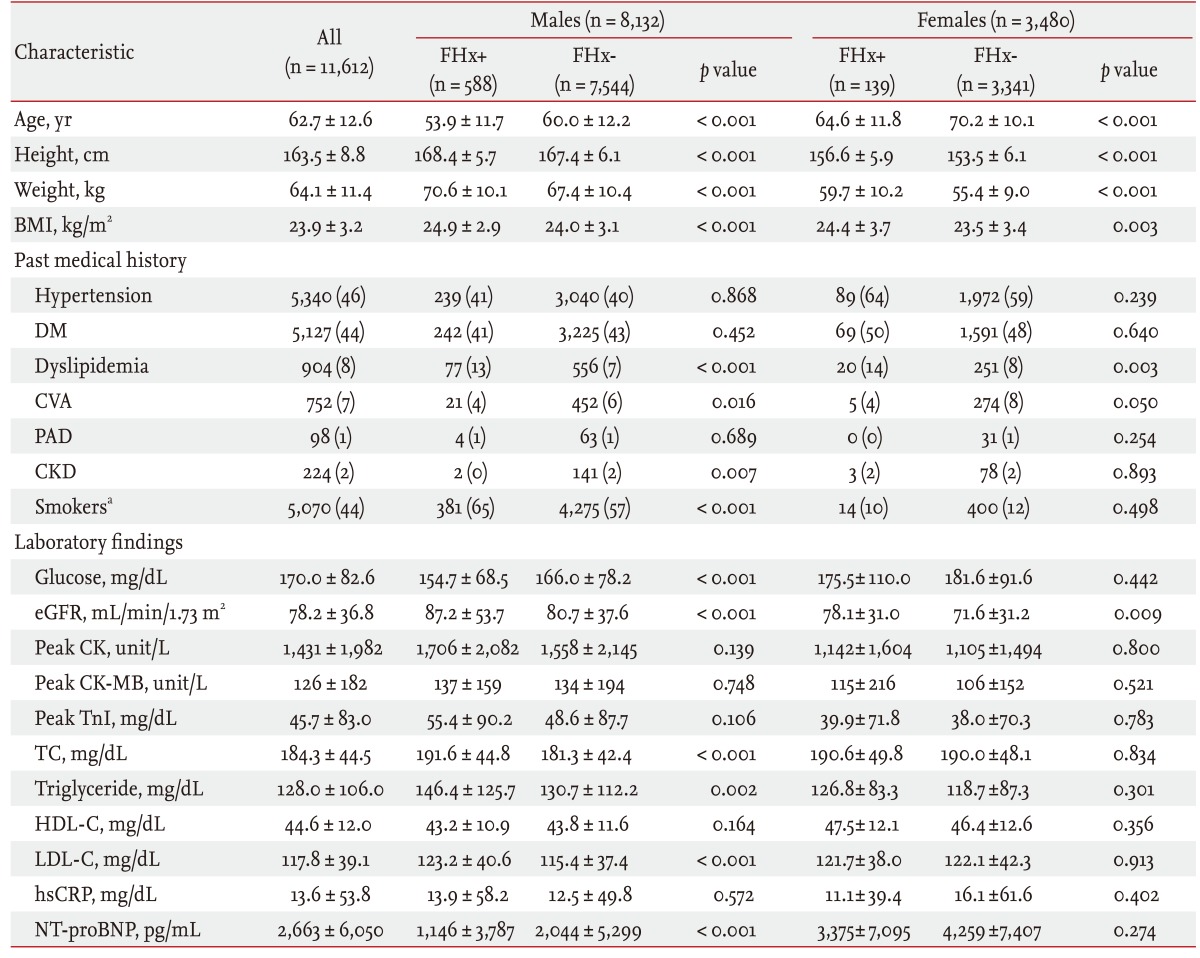
The median duration of follow-up was 341 days (interquartile range [IQR], 36 to 388). The median duration of follow-up was 359 days (IQR, 151 to 389) for FHx+ patients and 339 days (IQR, 34 to 388) in FHx- patients (p= 0.001). FHx+ patients included more males (8,132 [81%] vs. 3,480 [69%]; p<0.001) and were younger (53.9 ± 11.7 years vs. 60.0 ± 12.2 years in males, 64.6 ± 11.8 years vs. 70.2 ± 10.1 years in females; both p<0.001). Dyslipidemia was more common among FHx+ patients before the index admission (13% vs. 7% in males, p<0.001; 14% vs. 8% in females, p = 0.003). Male patients with FHx included more current smokers (65% vs. 57%; p<0.001). In female patients, there was no significant difference in laboratory findings except eGFR. However, FHx+ was related to poor lipid profiles including higher total cholesterol (191.6 ± 44.8 mg/dL vs. 181.3 ± 42.4 mg/dL; p<0.001), triglycerides (146.4 ± 125.7 mg/dL vs. 130.7 ± 112.2 mg/dL; p = 0.002), and low density lipoprotein cholesterol (LDL-C) level (123.2 ± 40.6 mg/dL vs. 115.4 ± 37.4 mg/dL; p<0.001) in male patients (Table 1).
Impact of FHx on AMI presentation
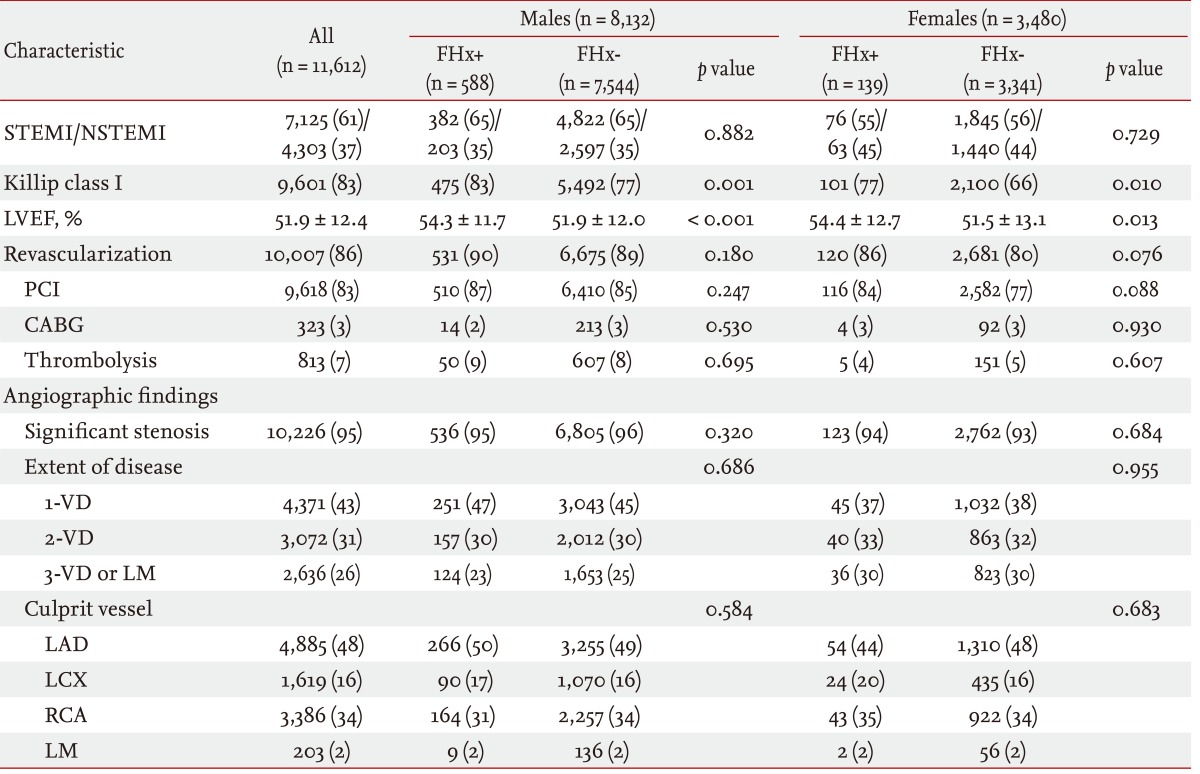
There was no statistically significant difference in the proportion of STEMI and NSTEMI between FHx+ and FHx- patients. More FHx+ patients presented with Killip classification I (82% vs. 74%; p<0.001) and higher LVEF (54.3% ± 11.9% vs. 51.8% ± 12.4%; p<0.001). FHx+ patients were treated more aggressively with revascularization compared with FHx- patients (90% vs. 86%; p = 0.007). There was no significant difference between FHx+ and FHx- patients in the presence of significant stenosis, the number of diseased vessel, or culprit vessel lesions confirmed by coronary angiography (Table 2).
Impact of FHx on clinical outcomes
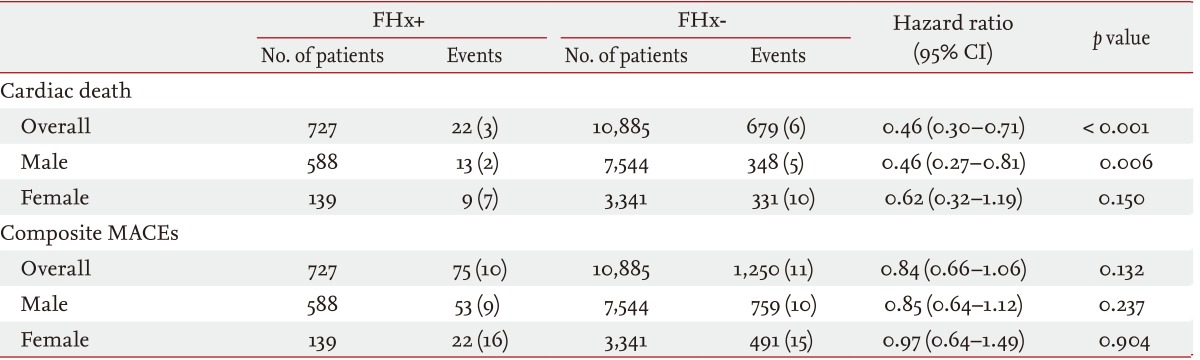
FHx+ patients had a lower incidence of cardiac death (3.0% vs. 6.2%, p<0.001) but there was no significant difference in the incidence of composite MACEs (10.3% vs. 11.5%, p = 0.132). Because significant differences were found in baseline characteristics and event rates of cardiac deaths (4.4% vs. 9.8%, p<0.001) and composite MACEs (15% vs. 10%, p<0.001) between male and female patients (Table 3), prognostic analyses were performed separately for males and females.
In multivariate analysis, the adjusted hazard ratio (HR) of FHx was 1.56 (95% confidence interval [CI], 0.95 to 2.55; p = 0.080) for cardiac death and 1.41 (95% CI, 1.09 to 1.82; p = 0.009) for composite MACEs in all patients (model 3). The prognostic implication of FHx were significant in female patients. A HR of FHx was 2.02 (95% CI, 0.98 to 4.17; p = 0.056) for cardiac death and 2.07 (95% CI, 1.32 to 3.24; p = 0.002) for composite MACEs in female patients. However, in male patients, no significant difference was found between FHx+ and FHx- patients. A HR of FHx+ was 1.29 (95% CI, 0.65 to 2.53; p = 0.467) for cardiac deaths and 1.22 (95% CI, 0.89 to 1.65; p = 0.215) for composite MACEs in male patients (Table 4).
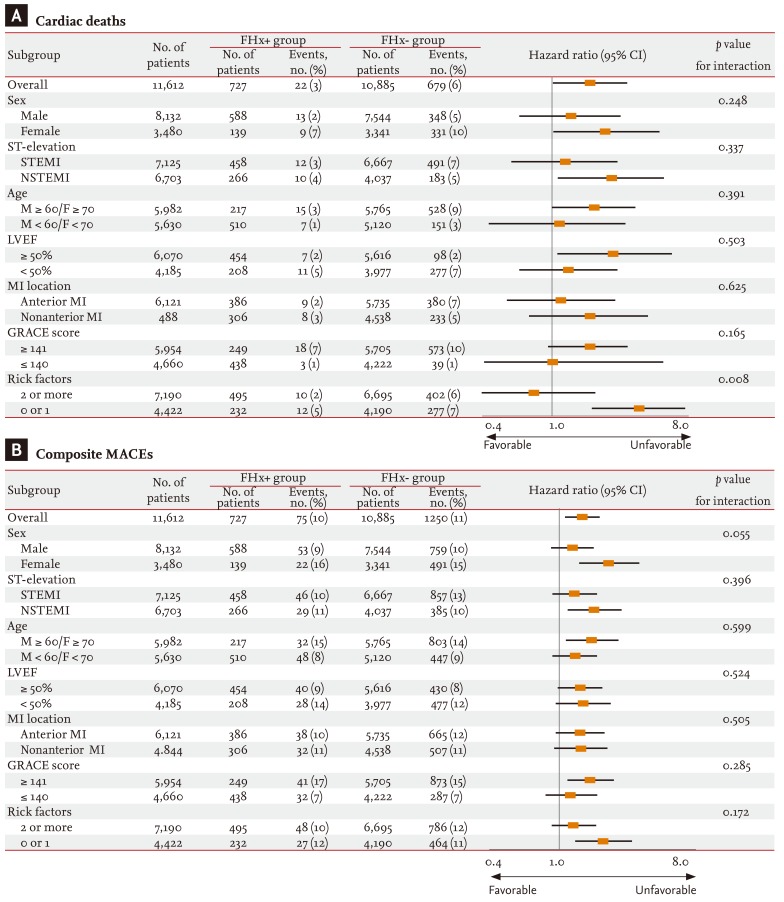
Further analyses were performed with dichotomous subgrouping according to ST-elevation, age, LVEF, MI location, GRACE score, and number of risk factors (including hypertension, DM, dyslipidemia [previous diagnosis, LDL-C ≥ 160 mg/dL, high density lipoprotein cholesterol, HDL-C<40 mg/dL, and triglycerides ≥ 200 mg/dL]) (Fig. 1). The prognostic implication of FHx was statistically significant only in older patients (≥ 60 years in males, ≥ 70 years in females) and patients with higher LVEF (≥ 50%), NSTEMI, or fewer risk factors. However, no significant interaction was found between each paired group except between male and female patients for composite MACEs (p = 0.057) and high (≥ 2 risk factors) and lower risk groups for cardiac deaths (p value for interaction = 0.008) (Fig. 1). In patients with fewer risk fa ctors, a HR of FHx was 2.65 (95% CI, 1.394 to 5.024; p = 0.003) for cardiac deaths and 1.51 (95% CI, 1.019 to 2.245; p = 0.040) for composite MACEs.
DISCUSSION
In this study, we intended to assess the significance of FHx as an independent predictor in the setting of secondary prevention. The FHx+ group was younger and included more male patients. Patients with FHx included more current smokers and had poor lipid profiles, especially the males. FHx was related inde pendently to poor clinical outcomes by survival analysis using a multivariate regression model.
Familial clustering of CHD has been demonstrated and FHx is considered a risk factor for CHD. In 1966, Slack and Evans [13] studied the relatives of patients with CHD and showed higher mortality from CHD. Since the 1980s, a few prospective studies have indicated that FHx is an independent risk factor, even after adjusting for other risk factors [14-17] and the NCEP-ATP III guidelines [1] included FHx as a major risk factor for CHD. The Framingham Study also revealed that FHx was associated with a risk of cardiovascular outcome; however, the Framingham risk score (FRS), a prediction model of CHD, did not include FHx in the equation [18]. Recent studies insisted that FRS may underestimate the risk of CHD in low-risk individuals with FHx [19,20]. In the Multi-Ethnic Study of Atherosclerosis (MESA) study, there was association between the presence of coronary artery calcium score and FHx independently from FRS or other traditional risk factors and it was revealed most significantly in Asian ethnicity [21]. These studies evaluated FHx as a risk factor for CHD events or clinical outcomes among the general population who did not suffer from CHD.
FHx, as an aspect of secondary prevention, had very limited evidence in support of the independent implication for clinical outcomes. Four studies have evaluated the prognostic implication of FHx as an independent risk factor in the patients with CHD. Tadros et al. [6] found that FH was an independent predictor of 30-day MACEs (odds ratio [OR], 3.56; 95% CI, 1.25 to 6.57; p = 0.01; n = 383). In other studies of post-PCI patients, FHx was related to adverse events during hospitalization (OR, 2.75; 95% CI, 0.93 to 8.11; n = 197) and after discharge (OR, 1.41; 95% CI, 0.98 to 2.04) [7], and to overall death and cardiovascular events after a 1-year follow-up (OR, 4.6; 95% CI, 1.7 to 12.8; p<0.005; n = 135) [8]. However, these studies were performed in small populations. In an Israeli study with 2,960 first-onset AMI patients [9], FHx was independently related to lower 1-year mortality (HR, 0.58; 95% CI, 0.42 to 0.80; p<0.001) contrary to common expectations. The investigators in the study suggested that the association between FHx and favorable outcomes might be mostly due to the younger age of the patients with FHx compared with those without FHx. Furthermore, the study could be influenced by selection bias because only patients who were admitted to intensive care units were included. The age difference between the patients with and without FHx was greater (53 years vs. 64 years) than in our study (56 years vs. 63 years). Additionally, the analysis was only of mortality, not composite MACEs, as the clinical outcome.
We found that FHx was independently related to poor prognosis. FHx was related to poor clinical outcomes after adjustment, but not significantly so, and to cardiac death in all patients. Because cardiac death was infrequent (701, 6.0%) especially in the FHx+ group (22, 3.0%), the statistical significance may be underpowered compared with that of composite MACEs (1,325, 11.4% in all patients; 75, 10.3% in the FHx+ group).
Our study showed that FHx was a significant prognostic indicator, which was further augmented in female patients. To reveal the difference in the impact of FHx between male and female patients, we compared the significance of the impact of FHx between both patients in subgroups with or without each risk factor (hypertension, diabetes, dyslipidemia, smoking, and any risk factor). However, there was no statistically significant difference in the subgroup analyses. The disparities of impact of FHx from each subgroups may be caused by less influence of FHx on outcomes than other major risk factors. And FHx itself may be related to other risk factors as well. Which risk factors and how much each risk factor affects the outcomes may also differ between male and female patients. Further subgroup analyses of each variable risk factors separately would be needed to assess the interaction between FHx and other risk factors. Despite these possibilities, FHx was independently associated with a poor outcome, and this may have significance for secondary prevention strategies in patients with first-onset AMI.
The relationship between female gender and FHx has been reported. An epidemiological study of the impact of FHx on the incidence of CHD revealed that maternal history may be more important in terms of increasing the risk [22]. The reason for gender differences in CHD remains unclear, but several mechanisms have been proposed, such as hormonal effects on lipid metabolism, insulin resistance, and thrombogenic factors. Poor lipid profiles, including elevated levels of LDL-C and triglycerides or low levels of HDL-C, are known to be related to CHD and other vascular diseases. Previous studies revealed that poor lipid profiles may have greater predictive potential for CHD incidence and mortality, especially in female patients [23-26]. However, another study indicated that FHx (OR, 5.11 vs. 3.14; p<0.05) and hypercholesterolemia (OR, 3.77 vs. 2.19; p<0.05) were associated with a higher risk of CHD in male patients [27]. In our study, a significant difference in lipid profiles between the FHx+ and FHx- group was only seen in male patients. However, true differences in lipid profiles caused by FHx may have been hidden in the female patients because the FHx- group included older patients, and total cholesterol and triglyceride levels tend to diminish with increasing age [28].
In our study, the prognostic implication of FHx was also further augmented in patients with fewer risk factors, especially for cardiac deaths. Some previous studies that emphasized a correlation between FHx and CHD suggested that FHx may be more important in low-risk patients [29-31]. A recent study of the MESA cohort [21] found that FHx was related to higher plaque burden, considered a risk for CHD, and the correlation was independent of other risk factors or FRS. Otherwise, there was no significant difference in the prognostic implication of FHx between the higher and lower GRACE score groups. The importance of FHx in evaluating the risk of CHD might have been underestimated, especially in patients at lower risk, as classified by traditional risk stratification systems, such as the number of conventional risk factors and FRS. Further studies will reveal the prognostic implication of FHx in various risk stratification systems.
Study limitations
First, although we used a large population, this was a retrospectively analysis of a multicenter prospective registry, and it was not randomized or controlled. The difference in age and gender was considerable, those factors could be significantly related to prognosis. Though we attempted to minimize the effects of confounders by adjustment, interference might not have been totally excluded, and some other potential confounders, such as socioeconomic factors, may have been present.
The 6.3% rate of FHx was lower compared with other studies in Western populations and other Asian ethnicities. Indeed, 15.6% of Japanese patients undergoing coronary intervention had FHx [32]. It is possible that the low incidence of FHx compared to CHD events is a result of the rapid increase in the incidence of CHD in Korea. However, the validity of FHx of CHD in our study was likely not high because confirmation of FHx depended mainly on patient self-reporting. Thus, the lower reported rate of FHx might have been related to ignorance of the implication of FHx on CHD of patients and/or physicians.
It is not certain whether patients enrolled in KAMIR are representative of all MI patients in Korea because KAMIR includes only patients admitted to major cardiac centers capable of primary PCI. However, the exclusion of PCI-incapable medical centers might not have affected the results of our study because in Korea it is possible to be admitted or transferred to a PCI capable medical center within 2 hours if primary PCI is required.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





