


INTRODUCTION
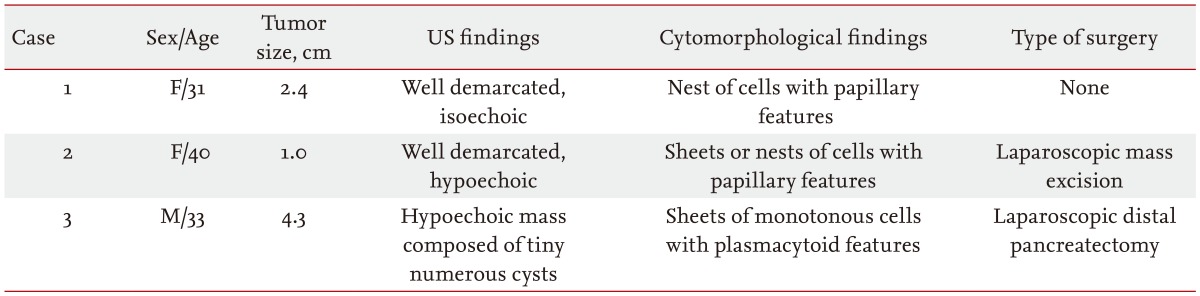
Solid pseudopapillary tumors (SPTs) of the pancreas are rare [1]. Preoperative diagnosis of SPT is difficult because they do not generally exhibit a typical appearance in radiologic tests. In the clinical setting, cytomorphological features and immunostaining of cell blocks help to discriminate SPTs from other pancreatic neoplasms [2,3]. Little is known about the differential diagnosis of pancreatic SPTs from other pancreatic tumors by endoscopic ultrasound (EUS)-guided fine needle aspiration (FNA), and Trucut biopsy (TCB) can be challenging. A definitive preoperative diagnosis of SPTs would allow for tailoring of the surgical resection with the goal of preserving as much of the pancreas as possible [4]. Herein, we report three cases of SPTs that highlight the importance of preoperative diagnosis for minimal invasive surgery, as well as the immunoprof ile that contributes to differentiating pancreatic lesions (Table 1).
CASE REPORTS
Case 1
A 31-year-old female was diagnosed with a pancreatic mass, which was found on an abdominal computed tomography (CT) scan performed during an examination for chronic liver disease. The physical examination was unremarkable. On admission, laboratory results were all within the normal reference ranges: white blood cell (WBC) count, 5.68 ├Ś 103/┬ĄL; hemoglobin, 11.8 g/dL; platelets, 188 ├Ś 103/┬ĄL; total bilirubin, 0.4 mg/dL; aspartate aminotransferase (AST)/alanine aminotransferase (ALT), 37/19 U/L; amylase/lipase, 84.0/84.6 U/L; carbohydrate antigen (CA) 19-9, 7.59 U/mL.
An abdominal CT scan showed an ovoid, slightly hypoattenuating, 2.4-cm mass with accompanying distal pancreatic duct dilatation in the body of the pancreas. Magnetic resonance imaging (MRI) demonstrated a well-circumscribed, round mass with mild upstream duct dilatation. Hypervascularity then delayed enhancement was noted during the arterial phase, which was interpreted as suspicious for SPT. During the EUS exam, an approximately 3-cm, well demarcated, homogenously isoechoic mass was observed in the neck of the pancreas. The tumor compressed the pancreatic vein and pancreatic duct but there was no evidence of invasion into the surrounding tissues.
EUS-FNA was performed three times using a 25-gauge needle without complications. Materials were smeared on glass slides, and then fixed immediately in 95% alcohol for hematoxylin and eosin (H&E) and Papanicolaou stains. Additional aspirate materials were used for preparation of the cell block, which was fixed in formalin.
Case 2
A 40-year-old female was diagnosed with a mass in the pancreatic body that was detected incidentally by abdominal ultrasonography during a general examination. All laboratory values were within normal levels: WBC, 5.32 ├Ś 103/┬ĄL; hemoglobin, 13.7 g/dL; platelets, 228 ├Ś 103/┬ĄL; AST/ALT, 16/9 U/L; amylase/lipase, 78.3/38.4 U/L; and CA 19-9, 28.6 U/mL. Abdominal CT showed no definite pancreatic lesion. MRI revealed a 1-cm sized, delayed enhancing lesion in the body of the pancreas. The tumor was a morphologically well-defined, hypoechoic mass by EUS imaging.
EUS-FNA was performed five times using a 25-gauge needle via a transgastric approach without complications. Specimens were prepared for cytologic smears and cell blocks using the same method as described above. The initial impression based on the imaging studies was pancreatic SPT or pancreatic neuroendocrine tumor.
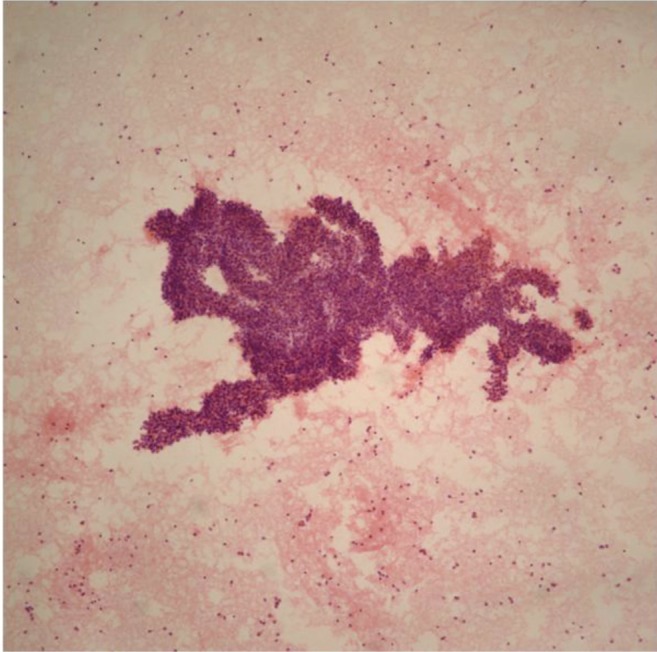
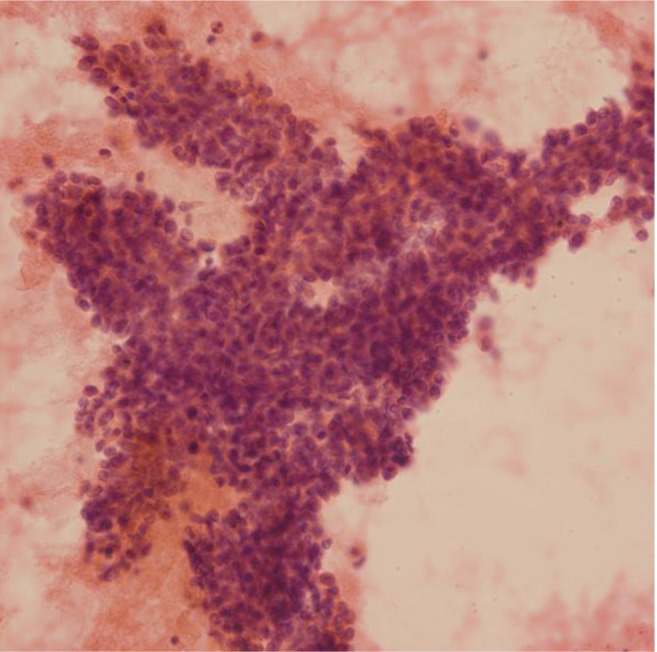
Cytologic smears and cell blocks showed hypercellular sheets or nests of atypical ductal epithelial cells with papillary features and a vascular core and some discohesive cell nests. Based on the characteristic histology, no immunostaining was performed. We interpreted the mass as a SPT.
Case 3
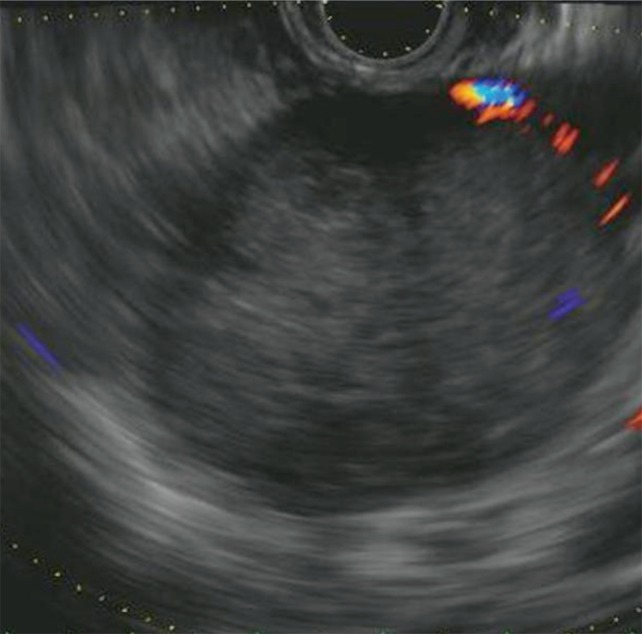
A 33-year-old male visited our hospital for evaluation of an adrenal mass, which was suspected in abdominal ultrasonography during a general examination. An abdominal CT scan revealed a mass in the tail of the pancreas, not the adrenal gland. The physical examination was unremarkable. Laboratory studies revealed slightly increased AST and ALT: WBC, 6.49 ├Ś 103/┬ĄL; hemoglobin, 14.3 g/dL; platelets, 269 ├Ś 103/┬ĄL; AST/ALT, 66/101 U/L; amylase/lipase, 78.9/45 U/L; CA 19-9, 28.7 U/mL. The CT scan showed a 4-cm heterogeneous low-attenuation mass with a smooth margin in the tail of the pancreas. The lesion demonstrated iso-enhancement relative to the surrounding pancreas in the adrenal enhancement phase. MRI demonstrated a 4.2-cm, well-demarcated cystic mass involving the tail of the pancreas. In the MR arterial phase, the lesion showed a relatively low enhancement pattern. EUS showed that the 5-cm cystic mass consisted of numerous tiny cysts (Fig. 4).
EUS-FNA and TCB were performed. We used a 25-gauge needle for FNA and a 19-gauge needle for TCB and approached the pancreas using a transgastric pathway. Both cell aspirates and tissue sections were obtained.
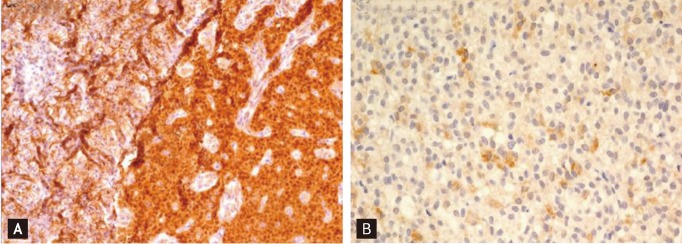
Smear and cell block sections showed hypercellularity and sheets and clusters of monotonous small cells with round nuclei. The tissue sections did not display typical pseudopapillary features. We performed immunohistochemical staining to identify other cystic lesions in the pancreas. Immunostaining was positive for ╬▓-catenin and CD10, whereas staining was negative for neuroendocrine markers, such as synaptophysin and chromogranin. These immunohistochemical features implied that the mass would be a SPT. A laparoscopic spleen-preserving distal pancreatectomy was performed. The resected specimen showed a round solid mass, measuring 5 cm, with some cystic change due to necrosis. Microscopically, the tumor was composed of round tumor cells with numerous pseudopapillae and multifocal necrosis. The immunoprofile was consistent with the biopsy specimen. The final histopathologic diagnosis was SPT of the pancreas.
DISCUSSION
The SPT is a relatively uncommon pancreatic tumor with low malignant potential. SPTs are found predominantly in young females. The radiologic findings are nonspecific; most cases require biopsy or cytologic examination for diagnosis [1]. Radiologically, SPTs are usually large, well-demarcated heterogenous lesions. SPTs have a range of appearances from solid to cystic, but typically, they present with a combination of these features. EUS provides more detailed images of the inner structure of cystic lesions and the overall accuracy of EUS is superior to that of CT scans and MRI for detecting pancreatic lesions; although, these findings are also not specific [3,5].
Small SPTs (< 3 cm) have been reported to have several radiologic features: pure solid consistency, low signal intensity on unenhanced T1-weighted images, high signal intensity on T2-weighted images, and early heterogeneous and slowly progressive enhancement [6]. Among the three cases described in this report, the first two cases revealed SPTs of < 3 cm and showed delayed enhancement, whereas the third case showed delayed enhancement, although it was a large mass. We suspected microcystic serous cystadenoma before pathological confirmation because of the gender of the third patient, and the imaging feature of delayed enhancement and tiny cystic aggregations on MRI and EUS. These findings suggested that a relatively large SPT did not undergo degenerative change and it had characteristics of small and early SPT. The positive immunohistochemical staining for ╬▓-catenin from the specimen obtained by EUS-FNA was critical to the diagnosis. It is well known that SPTs show frequent somatic ╬▓-catenin mutations, and nearly 100% of SPTs display the characteristic strong cytoplasmic/nuclear immunoreactivity of ╬▓-catenin [7].
The cytomorphological features of SPTs are distinctive, highly cellular smears that show numerous pseudopapillary tissue fragments with slender, branching fibrovascular stalks. The tumor cells form two or more layers on the fibrovascular core [1,2,8]. The immunophenotype for SPTs is somewhat variable, but helpful in defining the diagnosis. Most SPTs are immunoreactive for ╬▓-catenin, ╬▒-1-antitrypsin, and vimentin. The immunoreactivity for neuroendocrine cell markers, such as chromogranin and synatophysin, are not consistent in the literature, although chromogranin is usually negative while synaptophysin is identified as positive in ~30% of cases [3,7-9].
No single specific protocol is superior for preparing cell blocks for immunohistochemical staining. At our institute, we are in the process of investigating the adequate times of aspiration. Typically, we have selected 25- to 22-gauge needles depending on the mass size. The specimens obtained by needle aspiration are usually prepared in two ways: one method for cell blocks, another for smears. We select a lump of cells and stromal tissue, place it on the paper, and fix it in formalin. These fixed tissues are cut into fine sections. The rest of the aspirated samples are smeared on glass slides and fixed immediately in 95% alcohol. Immunohistochemical studies may be necessary for diagnosing SPTs in many cases, so it is helpful to obtain a specimen for the cell block.
Surgical specimens have been critical for SPT diagnosis. Nowadays, an aspirated specimen obtained by EUS-FNA is used for definitive diagnosis. Accurate preoperative diagnosis enables minimal surgery to preserve the pancreas. Mass excision or spleen-preserving distal pancreatectomy have been reported in some cases [10]. In addition, prior knowledge of the diagnosis may prevent complications such as intraoperative hemorrhaging. Because SPTs are hypervascular tumors, hemoperitoneum is prone to occur during surgery [2].
In summary, we diagnosed SPTs preoperatively by EUS-FNA using cytopathologic and immunochemical characteristics. We then treated the SPTs successfully by laparoscopic surgery. SPTs are rare tumors that require only minimal surgery and are associated with long-term survival, so long as the preoperative diagnosis is accurate.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





