


INTRODUCTION
The dramatic and rapid increase in the number of people with type 2 diabetes worldwide is no longer surprising. Accordingly, strict glycemic control with lifestyle modifications has been emphasized to prevent microvascular and macrovascular diabetic complications [1,2]. However, three large clinical trials, Action in Diabetes and Vascular Disease (ADVANCE), Action to Control Cardiovascular Risk in Diabetes (ACCORD), and the Veterans Affairs Diabetes Trial, failed to demonstrate that intensive glucose control improved the primary cardiovascular outcomes in patients with type 2 diabetes [3,4,5]. In addition, patients who were assigned randomly into the intensive treatment group experienced more frequent episodes of hypoglycemia than did those assigned to the standard treatment group. Moreover, all three trials revealed that episodes of severe hypoglycemia were associated with an increased risk of subsequent mortality and morbidity [6].
Intensive glucose control is always accompanied by an increased risk of hypoglycemic episodes, and an increased incidence of hypoglycemic events is accompanied by direct and indirect health and economic burdens [7]. Hypoglycemic events, even if not severe, have negative effects on diabetes self-management, sleep quality, and the daily function of patients with both type 1 and type 2 diabetes [8]. The mean medical cost per severe hypoglycemic event was reported to be ~1.35-fold higher than the annual treatment cost for a patient with diabetes without complications in Korea [7]. Considering the indirect costs such as productivity, missed work, and the time lost by patients and their family members, the overall economic and social costs are huge. Therefore, the identification of measures to prevent hypoglycemia in patients with type 2 diabetes is needed urgently.
DEFINITION OF HYPOGLYCEMIA
Hypoglycemia was described originally by Whipple, and is known as Whipple's triad: symptoms consistent of hypoglycemia, a low plasma glucose level, and relief of the symptoms when the plasma glucose concentration is raised [9]. Generally, a plasma glucose concentration ≤ 70 mg/dL is the cut-off value for the definition of hypoglycemia [10]. Because the glycemic thresholds for hypoglycemic symptoms could be lower in patients who experience recent antecedent hypoglycemia and higher in diabetic patients with uncontrolled plasma glucose concentrations [11,12], this simple biochemical cut-off method cannot be used to define hypoglycemia accurately, particularly in diabetic patients with recurrent or uncontrolled hyperglycemia. Hypoglycemic symptoms can occur in patients with biochemically normoglycemia or uncontrolled, prolonged hyperglycemia, even within the normoglycemic range [13].
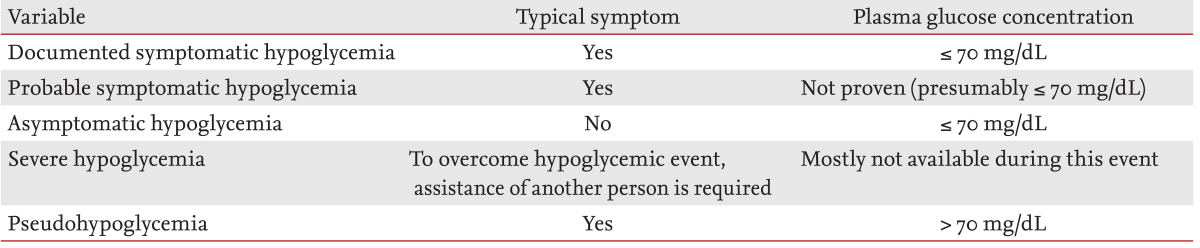
According to a report by a workshop of the American Diabetes Association and the Endocrine Society, hypoglycemia in diabetes could be defined and classified as shown in Table 1 [10]. Among the categories of hypoglycemia hypoglycemia, severe hypoglycemia could be defined as an event that requires the assistance of another person to actively administer carbohydrates, glucagon, or take other corrective actions [10]. It is a serious clinical situation in subjects with both type 1 diabetes and advanced type 2 diabetes. If severe hypoglycemia is not managed promptly, it can be life threatening.
NORMAL RESPONSE TO HYPOGLYCEMIA
The brain uses glucose as its primary energy source. Under normal physiological conditions, the brain is unable to synthesize or store glucose and is vulnerable to glucose deprivation. Several physiological mechanisms have evolved to protect the integrity of the brain to respond to and limit the effects of hypoglycemia.
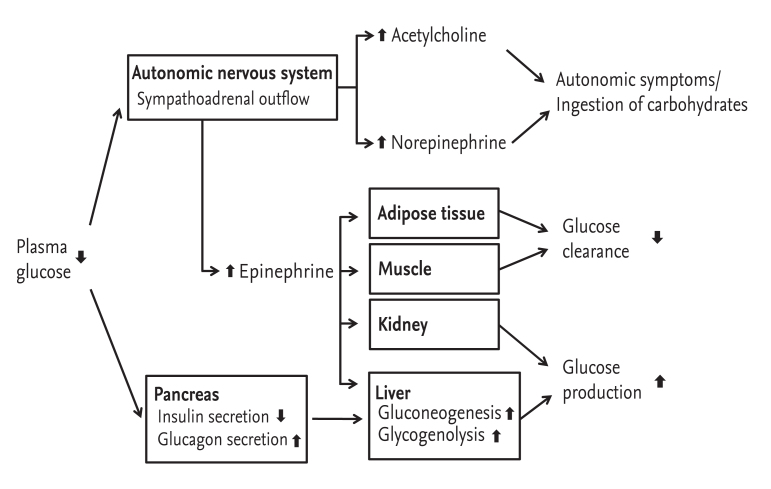
If blood glucose concentrations fall below the normal range, physiological defense mechanisms to overcome hypoglycemia become activated in nondiabetic individuals. This includes a consecutive decrease in insulin secretion, an increase in glucagon secretion and, in the absence of an increase in glucagon, enhanced secretion of adrenomedullary epinephrine (Fig. 1) [14]. The clinical symptoms and signs of hypoglycemia are derived from these counter-regulatory hormonal responses. The typical symptoms of hypoglycemia can be classified into two groups: autonomic (nervousness, anxiety, tremulousness, sweating, palpitation, shaking, dizziness, hunger, and tingling) and neuroglycopenic (confusion, weakness, tiredness, drowsiness, difficulty with concentration, speech difficulty, odd behavior, and incoordination) [15,16,17,18]. In serious cases stupor, seizure, coma, or death can occur. Diaphoresis, pallor, increased heat rate or systolic blood pressure, disorientation, hypothermia, and focal neurological deficits are often observed, but these symptoms are not specific to hypoglycemia; instead, they are the result of a perception of the physiological changes caused by the central nervous system-mediated sympathoadrenal discharge triggered by hypoglycemia [18].
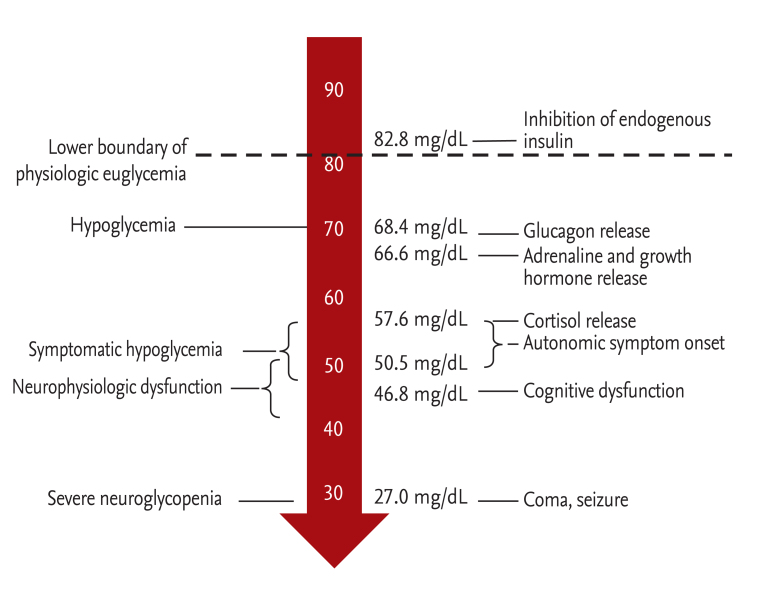
The subjective recognition of the hypoglycemia is fundamental for effective patient self-management and preventing severe progression [19]. A lack of awareness of hypoglycemia can be defined as onset of the neuroglycopenic symptoms before the onset of autonomic warning symptoms [20]. If the sympathoadrenal response to hypoglycemia is delayed the autonomic warning symptoms are not recognized, which allows the patient to fall into severe neuroglycopenia (Fig. 2) [21]. Impaired autonomic symptoms during hypoglycemia are warning signs of hypoglycemic unawareness, and results in an ~6-fold higher frequency of severe hypoglycemia [22].
COMPROMISED DEFENSES AGAINST HYPOGLYCEMIA: THE PATHOGENESIS OF HYPOGLYCEMIA-ASSOCIATED AUTONOMIC FAILURE
Patients with type 1 diabetes and long-standing type 2 diabetes with β-cell failure or absolute insulin deficiency have compromised defense mechanisms against hypoglycemia. This results in a lack of endogenous insulin secretion and subsequent glucagon secretion, and impaired epinephrine release (Fig. 2). Therefore, plasma glucose levels fall but hypoglycemic symptoms are absent, which reflects an attenuated sympathetic neural response [14,23].
In patients with hypoglycemia unawareness, the subjective responses to early hypoglycemia fail and so cognitive impairment is the first response [9]. Individual experience of severe hypoglycemia or a self-reported history of impaired perception of autonomic symptoms during hypoglycemia is important clue for diagnosing hypoglycemia unawareness [24,25,26,27]. It is largely the result of reduced sympathetic neural, rather than adrenomedullary, responses to hypoglycemia [28]. Hypoglycemia-associated autonomic failure is a functional disorder that differs from classical diabetic autonomic neuropathy, and is caused most frequently by recent antecedent hypoglycemia [29]. However, it is partly reversible by avoiding hypoglycemia [30,31], which restores the autonomic symptoms of hypoglycemia within 2 weeks, and reverses hypoglycemic unawareness by 3 months [24,31].
PREVALENCE AND INCIDENCE OF HYPOGLYCEMIA
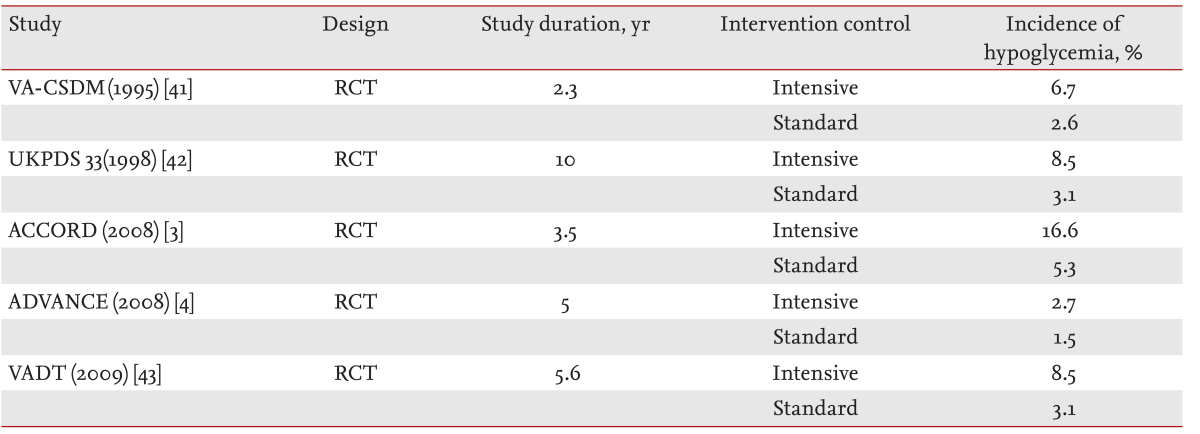
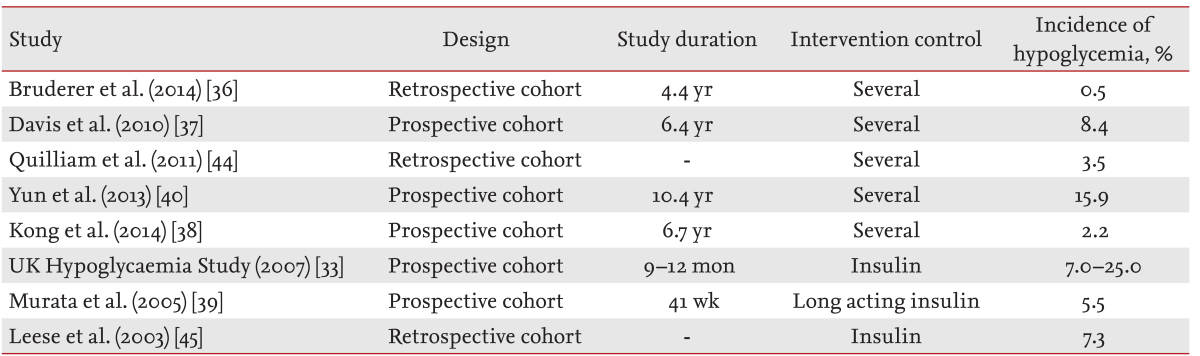
Non-severe hypoglycemia occurs commonly in patients with both type 1 and type 2 diabetes. A recent study by Wendel et al. [32] reported that 84% of individuals with type 2 diabetes experienced at least one hypoglycemic event, and that 42% of hypoglycemic episodes were asymptomatic. Severe hypoglycemia caused by glucose-lowering treatment (sulfonylurea, glinide, or insulin) occurs more frequently in type 1 than type 2 diabetes [33,34]. In a population-based study of type 1 diabetes, the overall rate of severe hypoglycemia was 1.3 episodes/patient-year (36.7% of subjects) [35]. The incidence of severe hypoglycemia in patients with type 2 diabetes has been reported to be 0.1 to 35 per 100 patient-years (Tables 2 and 3) [3,4,33,36,37,38,39,40,41,42,43,44,45]. In addition, the mean incidence of mild hypoglycemia was also reported to be 1 to 2 and 0.3 to 0.7 episodes/patient/week in patients with type 1 diabetes and insulin-treated type 2 diabetes, respectively [17]. However, the distribution of severe hypoglycemia is highly skewed, since 5% of subjects accounted for 54% of all episodes [35]. We reported recently that the incidence of severe hypoglycemia was 1.55 per 100 patient-years, and that ~25% of type 2 diabetic patients with severe hypoglycemic events experienced antecedent hypoglycemia within 3 to 6 months [40]. However, ethnic differences regarding the prevalence of hypoglycemic events are unknown.
CLINICAL SIGNIFICANCE OF HYPOGLYCEMIA
Hypoglycemia can be fatal [46,47], and the increased mortality is mediated via an increased risk of cardiovascular death. In the ADVANCE and ACCORD trials, severe hypoglycemia was associated with a significantly increased risk of major cardiovascular events and a 1.4 to 3-fold higher risk of mortality [6,48]. Hypoglycemia changed cardiac repolarization and induced arrhythmias in patients with type 1 and type 2 diabetes [49,50,51]. The previously reported EURODIAB IDDM complication study demonstrated that severe hypoglycemia events were independently associated with a prolonged corrected QT (QTc) interval in type 1 diabetic patients [52]. A prolonged QTc interval reflects abnormalities in ventricular myocardial repolarization, and is an independent risk factor for mortality in patients with type 1 diabetes [53]. Similarly, myocardial ischemic changes with a prolonged QT interval have been also observed during insulin-induced hypoglycemia in patients with type 2 diabetes [49,50,54].
A study using a continuous glucose-monitoring device revealed that most hypoglycemic episodes occurred overnight (between 10:00 PM and 6:00 AM), and were not likely to result in recognized hypoglycemic symptoms [55]. During sleep the sympathoadrenal response to hypoglycemia is blunted [56]. Attenuated sympathoadrenal activity at night leads to compensatory activation of the parasympathetic system [17]. These factors contribute to induce ventricular arrhythmia, bradycardia, and atrial or ventricular ectopic beats during nighttime hypoglycemia [57].
The stress hormones that are secreted in response to hypoglycemia increase blood viscosity and promote coagulation, leading to endothelial dysfunction and the release of inflammatory cytokines into the circulation. The recovery from such an inflammatory response could take upto 1 week [17,58]. The cardiovascular outcome of patients who experience nighttime hypoglycemia might be related to the increased circulating levels of inflammatory markers, vascular adhesion molecules, and markers of thrombosis and platelet activation [59].
The effects of severe hypoglycemia on the structure and function of the brain have not been well defined. The ACCORD-MIND (ACCORD-Memory in Diabetes) MRI trial showed that severe symptomatic hypoglycemic events in treated type 2 diabetic patients were not associated with the accentuated loss of total brain volume and/or increased abnormal white matter volume compared with patients with type 2 diabetes without hypoglycemia [60]. However, a meta-analysis demonstrated that, compared with diabetic children without hypoglycemia, children with type 1 diabetes and recurrent severe hypoglycemia had slightly lower performance in some cognitive domains, including intelligence, memory, learning, and verbal fluency/language. The highest impairment was found in memory and learning [61]. In the Edinburgh Type 2 Diabetes Study, both the history and incidence of hypoglycemia were associated with a greater cognitive decline after adjusting for vascular risk factors and cardiovascular and microvascular disease [62]. Although there was a gross lack of structural changes in the brain, functional changes related to recurrent or severe hypoglycemic events should not be neglected and should be avoided.$
Hypoglycemia was a significant factor for the incidence of patient adherence to medication and glycemic control [63]. The fear of hypoglycemia might make many patients using insulin reluctant to use the recommended insulin dose or achieve the target range of glycemic control [64]. Individuals who experienced recent hypoglycemia, also reported an increased interference with social activities, missed work, work impairment, and decreased overall health-related quality of life [63]. Approximately one in seven patients with type 2 diabetes complained that they missed a work appointment or meeting or did not finish a task on time due to their recent non-severe nocturnal hypoglycemic events [8]. The loss of productivity was estimated to range from US $15 to $94 per non-severe hypoglycemic event, corresponding to 8.3 to 16 hours of lost work time per month and a mean 4.2 to 5.6 additional blood glucose test strips [7,65].
According to the recently published Hong Kong Diabetes Registry, cancer occurred more frequently among type 2 diabetic patients who experienced severe hypoglycemia. This suggests that severe hypoglycemia might reflect the coexistence of concurrent medical conditions that require additional clinical attention [66].
RISK FACTORS FOR HYPOGLYCEMIA IN PATIENTS WITH TYPE 2 DIABETES
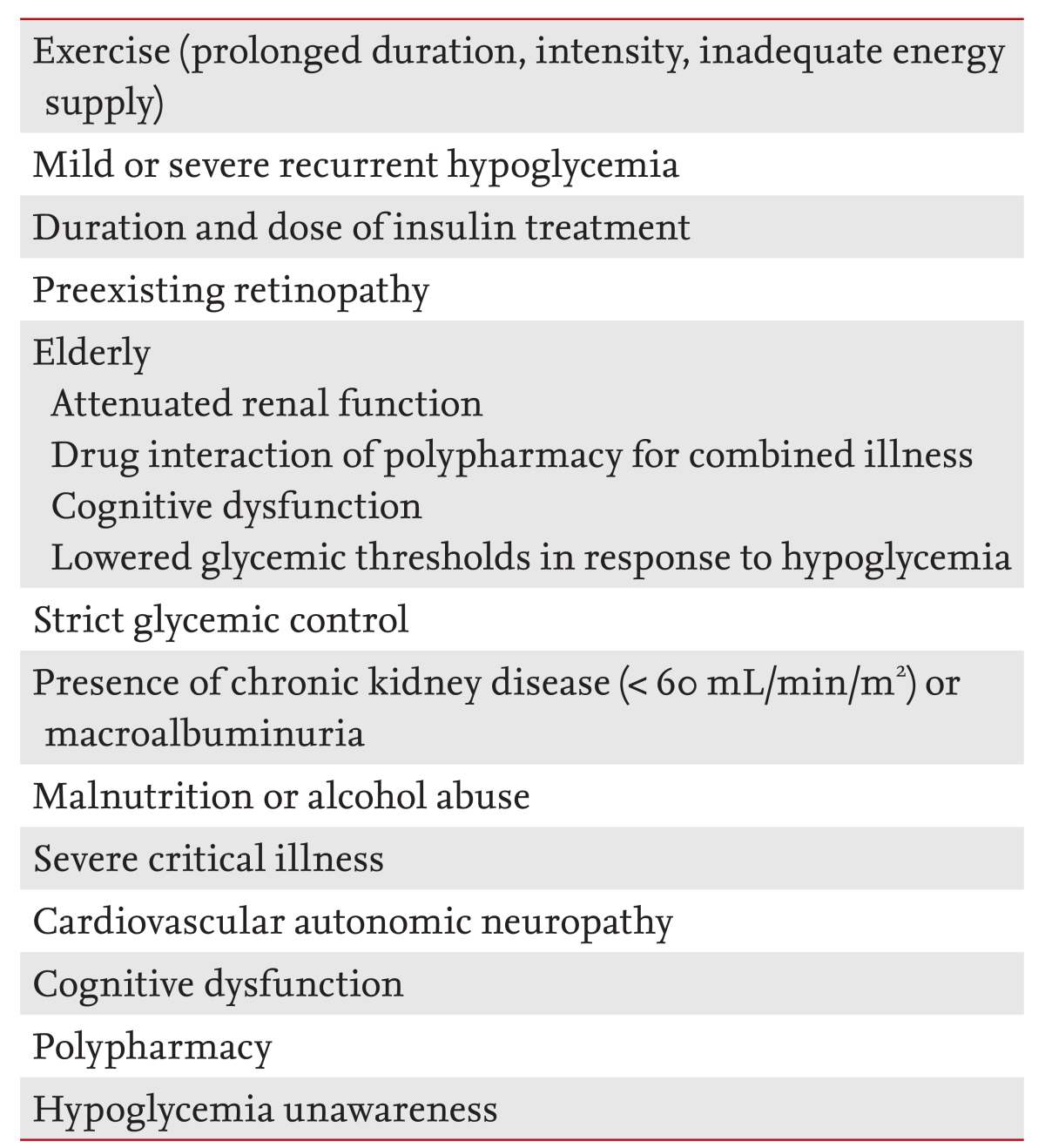
The causes of most hypoglycemic episodes are related to exercise, missing a meal or excessive dieting, and changes in medication; however, 56% of hypoglycemic events have an unknown cause [32]. The previous experience of hypoglycemia should be evaluated in all patients treated with insulin, sulfonylurea, or glinide. If patients complain of a history of recurrent hypoglycemia or hypoglycemia unawareness, they will require additional attention. Elderly diabetic patients, and individuals decreased performance in self-care activity, cognitive impairment, or advanced diabetic vascular complications are vulnerable to hypoglycemia, and the clinical outcomes of their hypoglycemic episodes are serious [67,68]. They also exhibit a higher risk of hypoglycemia that is associated with multiple medications and a reduced glycemic threshold in response to hypoglycemia. Diabetic patients with chronic kidney disease have a higher risk of hypoglycemia [66,69], due to the prolonged clearance of renal insulin or hypoglycemic agents and reduced renal gluconeogenesis (Table 4) [69].
MANAGEMENT AND PREVENTION OF HYPOGLYCEMIA
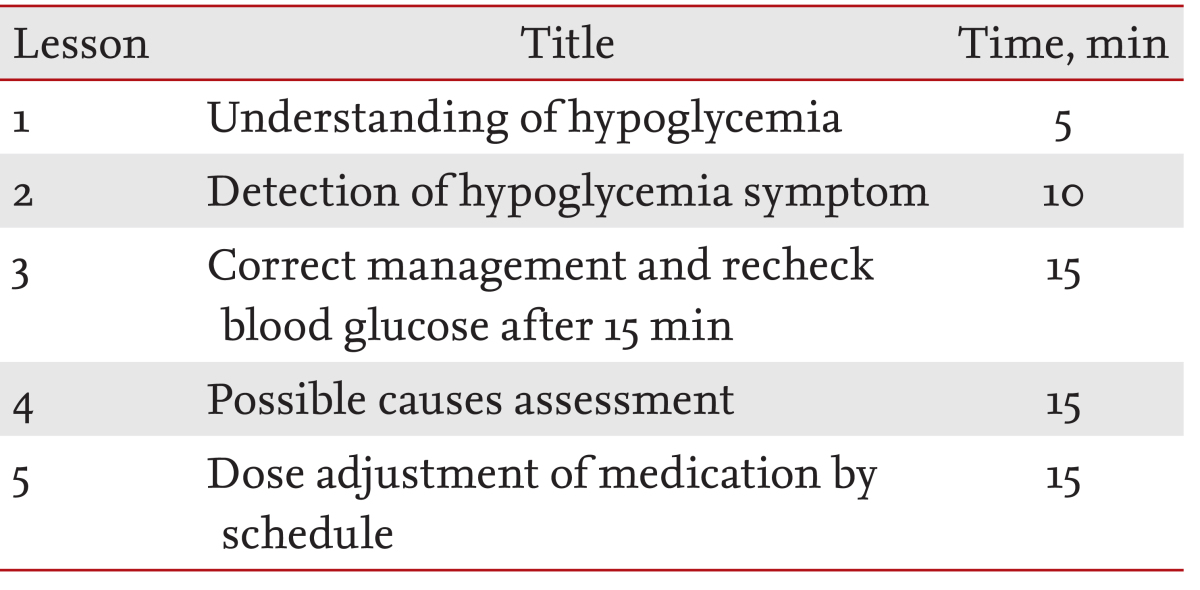
Structured diabetes education is an essential start for diabetes care [70]. Education is particularly important for patients with a higher risk of hypoglycemia. A structured education program can improve hypoglycemia awareness and the self-management ability of patients to reduce the incidence of hypoglycemia [71]. For intensive education, patients should be trained in hypoglycemia management skills, including the frequent self-monitoring of blood glucose (SMBG), glucose supplementation, re-checking blood glucose after a hypoglycemic episode, and dose adjustment of their medication. We found previously that intense individualized education programs improved the skills by which patients managed hypoglycemia as well as dose adjustment according to fasting glucose levels significantly [72]. In particular, education regarding the dose adjustment schedule for medications after a hypoglycemic event played an important role for preventing recurrent hypoglycemia. Similar to individualized glycemic goal setting according to the individual clinical situation, the educational curriculum and reinforcement should be individualized to focus on preventing hypoglycemia (Table 5).
Meal plans should also be individualized according to the patients' hypoglycemic medications. Patients taking long-acting sulfonylureas or a fixed insulin regimen are instructed not to skip or delay their meals. If patients are treated with postprandial insulin injections, the dose and meal times should be coupled [10]. Long-acting basal analogs, such as insulin glargine, insulin detemir, and insulin degludec, are preferable to neutral protamine Hagedorn because of their more physiological profiles and lower variability [73,74]. These analogs reduce the incidence of symptomatic hypoglycemic events by ~30% in patients with type 2 diabetes [74]. In addition, healthcare professionals should train patients to recognize and respond promptly to early neuroglycopenic symptoms [10].
SMBG using a point-of-care glucose meter is mandatory in patients at risk of hypoglycemia. Specifically, SMBG allows patients treated with glucose-lowering medication to detect hypoglycemic events, even in the absence of symptoms. In particular, nocturnal hypoglycemia can cause major problems with therapeutic management due to challenges with the detection and prevention [64,75]. Therefore, patients with nocturnal hypoglycemia, especially those with pre-existing ischemic heart disease or recurrent hypoglycemia, are encouraged to perform SMBG more frequently, and greater clinical attention is needed.
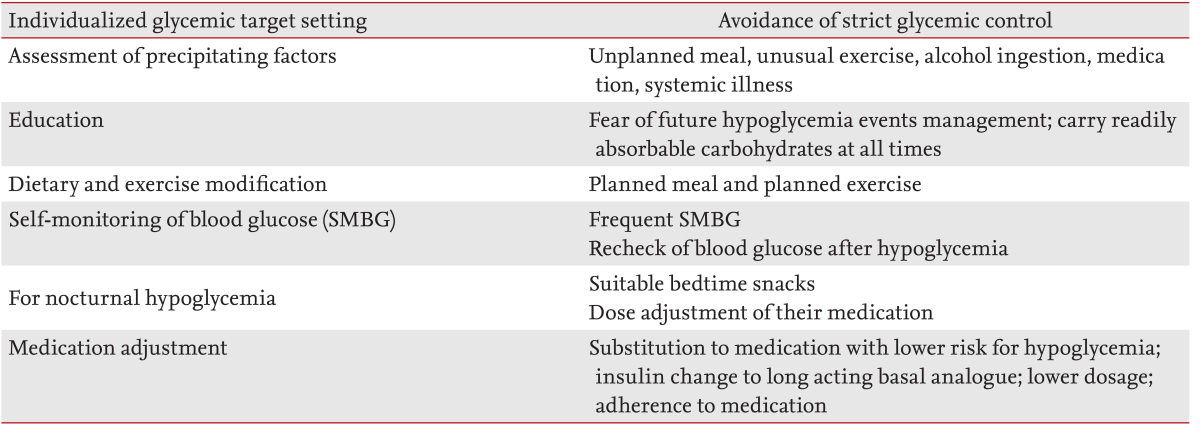
Elderly patients are at an increased risk of impaired renal function, cognitive impairment, and presenting with atypical hypoglycemic symptoms such as delirium or neurological events. Cognitive dysfunction is an important risk factor for hypoglycemia, and hypoglycemic events might further worsen cognitive function [76,77]. In older patients with poorly controlled diabetes, the most common barrier to achieving proper glycemic targets was inadequate medication caused by patient reluctance to make changes to their medication doses between clinical visits or during conditions such as illnesses [78]. Poor medication adherence in patients with type 2 diabetes and hypoglycemia might be caused by fear of further episodes of hypoglycemia [63]. Physicians educate and make recommendations to patients regarding self dose adjustment. Therefore, a practical approach that provides safe and helpful care using phone calls or more frequent patient contact is important. The total approach for type 2 diabetic patients with frequent hypoglycemia is summarized in Table 6.
CONCLUSIONS
The management of hypoglycemia is a critical clinical issue for patients with type 2 diabetes. If possible, hypoglycemia and severe hypoglycemia should be avoided in all patients with type 2 diabetes. However, a considerable number of diabetic patients are at risk of hypoglycemic episodes during their daily lives. Recurrent hypoglycemic or severe hypoglycemic attacks usually have unfavorable and serious clinical consequences; therefore, health care providers should recognize the risk of hypoglycemia and its clinical importance when making decisions. A considerable number of hypoglycemic episodes are asymptomatic and usually occur at night. Only a small number of patients experience multiple events of hypoglycemia, but these individuals might be prone to developing severe hypoglycemia. For patients at a higher risk of hypoglycemia glycemic goals should be determined according to their clinical situations. At the same time, diabetic education should be implemented promptly and appropriately.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





