


INTRODUCTION
Pulmonary paragonimiasis is a food-borne parasitic disease of the lungs caused by the lung fluke Paragonimus westermani or other Paragonimus species. Human infection most often occurs by the ingestion of raw or undercooked freshwater crab or crayfish infected with metacercaria [1,2,3].
The classic signs of pleuropulmonary paragonimiasis include a chronic cough with rusty-brown sputum, hemoptysis, pleurisy, and fever, and radiographic findings of patchy densities, linear infiltration, nodules, pleural effusion, and pulmonary cavities [4,5,6,7]. As these symptoms and radiologic findings are similar to those of tu berculosis, lung cancer, and other pulmonary infections, many patients with paragonimiasis face a considerable burden of long-term hospitalization as well as unnecessary procedures and treatments before receiving the correct diagnosis [8,9,10,11,12].
In South Korea, where paragonimiasis is endemic, the incidence of the disease has decreased recently as a result of improvements in public health and changes in dietary habits [13]. However, we continue to observe clinical cases of pulmonary paragonimiasis with features that differ from those of previously reported cases [14]. Many of these patients were initially suspected to have pulmonary tuberculosis and, particularly, pleural tuberculosis.
Therefore, we retrospectively analyzed the data from patients diagnosed with pleuropulmonary paragonimiasis during the last 10 years to determine how this disease can be differentiated from other pleural diseases.
METHODS
From January of 2001 through September of 2011, 81 patients were diagnosed with pulmonary paragonimiasis in the Pulmonary Department of Wonkwang University Hospital (Iksan, Korea). The medical records of 20 patients who were diagnosed with pleuropulmonary paragonimiasis after the suspicion of pleural tuberculosis were reviewed. The diagnoses of pleuropulmonary paragonimiasis were based on seropositivity for P. westermani and/or the detection of Paragonimus eggs (in sputum, aspirated pleural effusion, or feces) as well as pleuropulmonary involvement.
The medical records of the patients included in this study were reviewed for clinical data, including symptoms, a history of eating raw or undercooked freshwater crab or crayfish, laboratory test results, and other diagnostic procedures performed. Abnormal findings on chest radiographs (CXRs) or computed tomography (CT) scans were classified into two types: intrapulmonary parenchymal lesions, including air-space consolidation and nodular, linear, or cystic opacification, and pleural lesions, including pleural effusion, pneumothorax, and hydropneumothorax. Thoracentesis and needle pleural biopsy were performed in patients with pleural effusion to rule out other diseases. The sputum and pleural effusion fluid specimens were cultured and stained by Ziehl-Neelsen staining to identify acid-fast bacilli (AFB). A tuberculin skin test (TST) was also performed.
RESULTS
Clinical manifestations
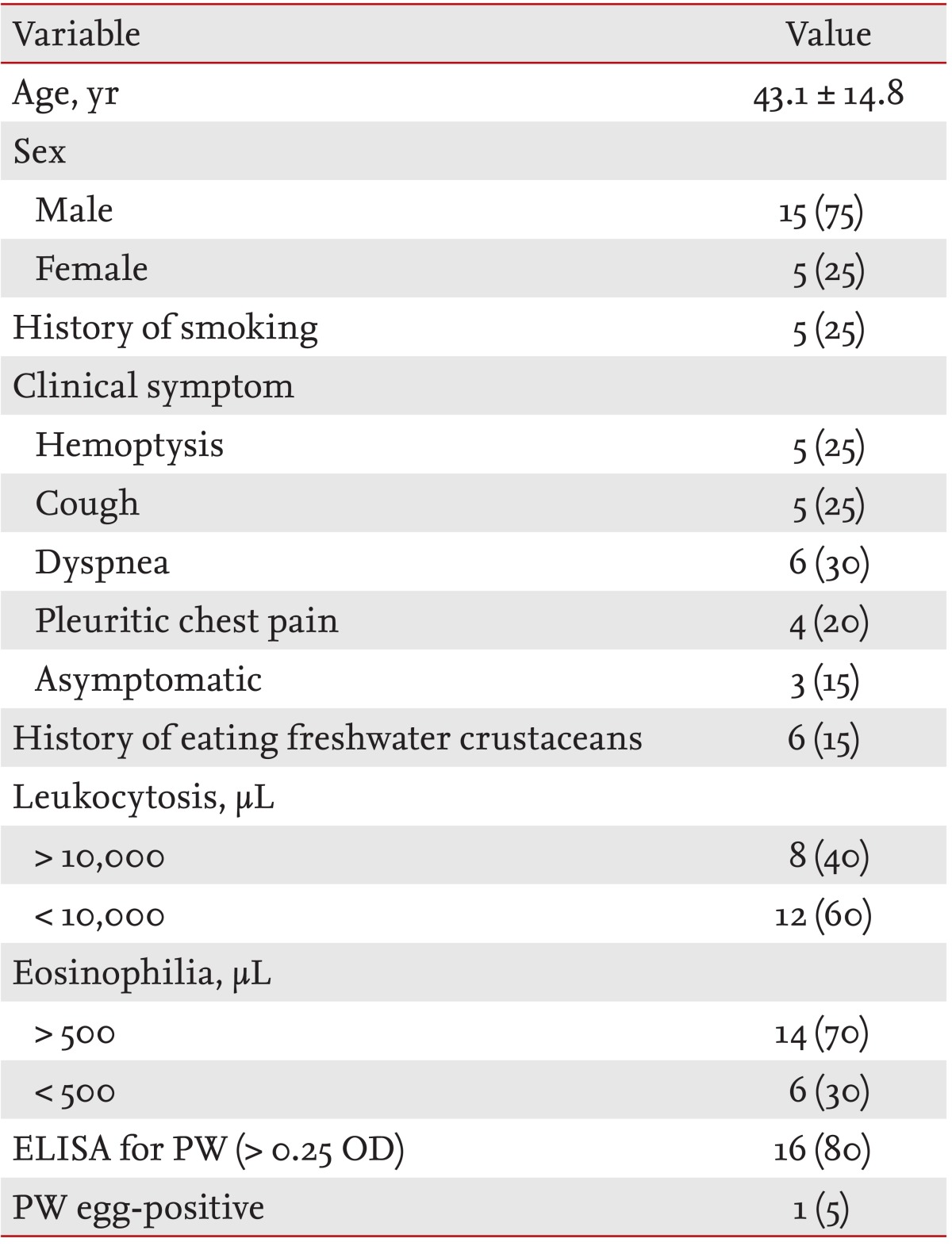
A total of 20 patients (15 males and five females) with a median age of 43 years (range, 5 to 65) were diagnosed with pleuropulmonary paragonimiasis. Of these, 17 patients (85%) presented with respiratory symptoms, including dyspnea, hemoptysis, cough, and pleuritic chest pain. Three patients (15%) were asymptomatic, and in these cases the disease was discovered from abnormal CXRs obtained during general health examinations. Six (30%) patients had a history of consuming freshwater crustaceans (Table 1). No dietary history was available for the remaining 14 patients (70%).
Laboratory findings
Peripheral blood leukocytosis (> 10,000/µL) was present in eight patients, while the white blood cell counts were within the normal range in the remaining 12 patients. Peripheral blood eosinophilia (> 500/µL) was detected in 14 patients (Table 1). A sputum smear examination for Mycobacterium tuberculosis was negative in 16 patients; four patients were not tested because of a small sputum sample. Five patients had a positive TST result while three patients had an intermediate TST result.
CXRs and CT findings
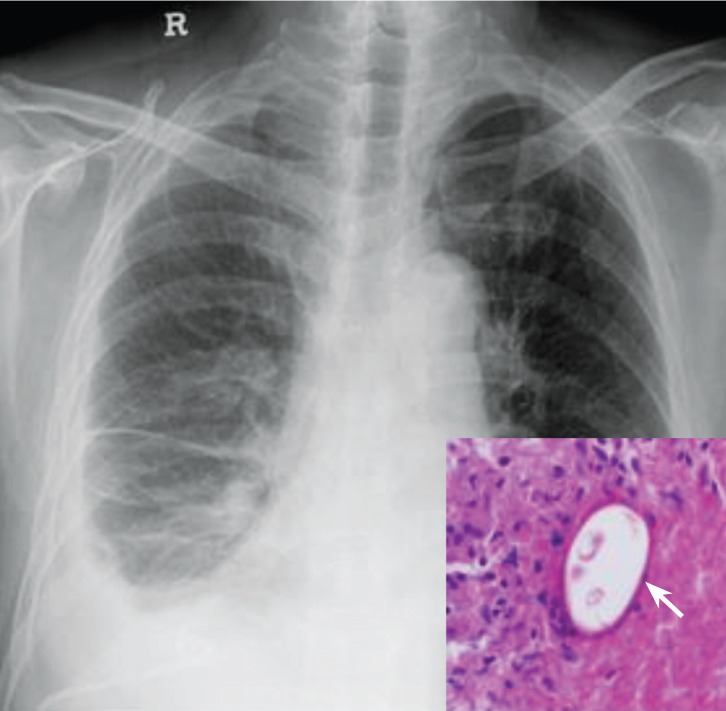
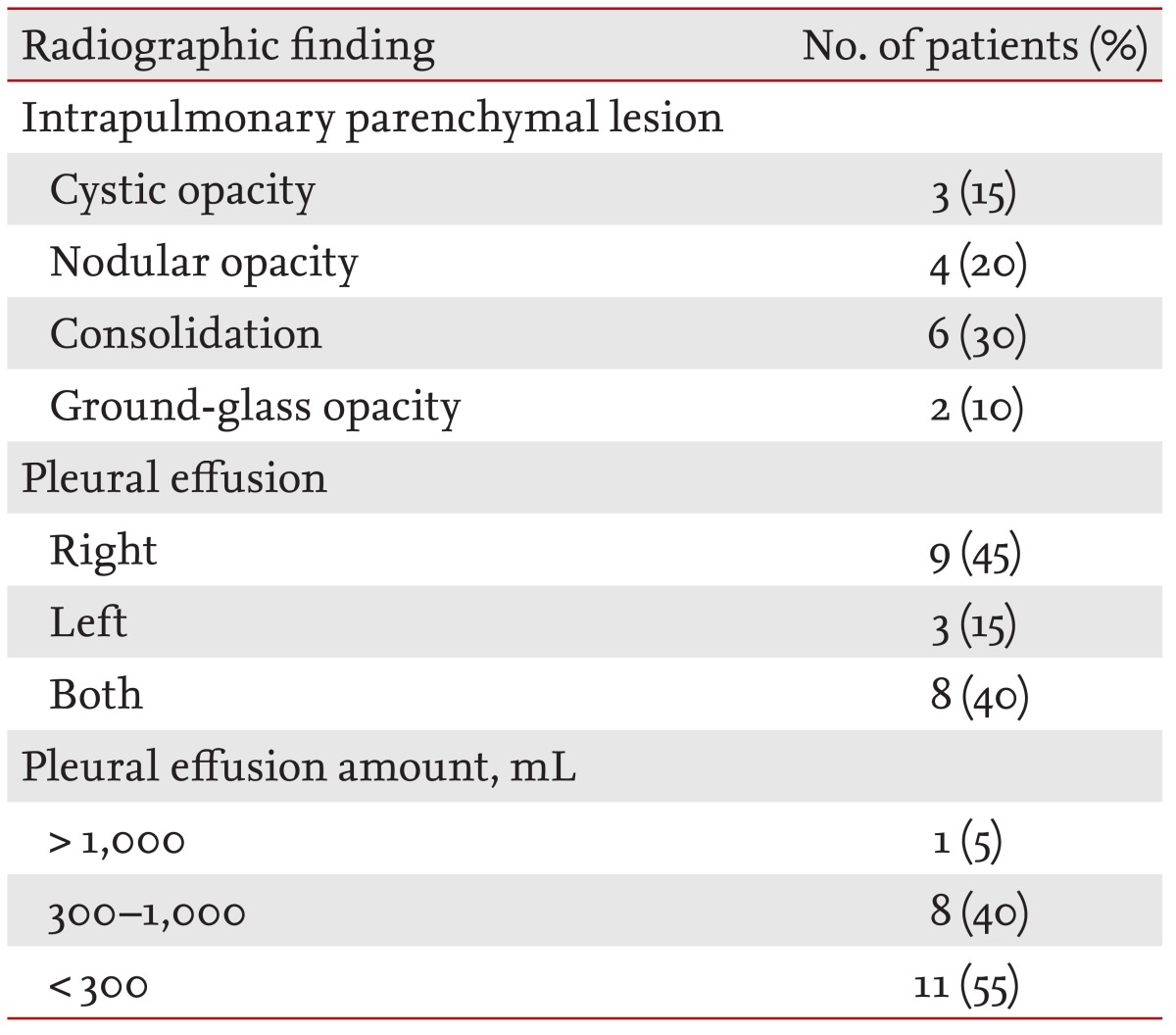
A retrospective review of the CXRs and CT scans of the 20 patients revealed a variety of intrapulmonary parenchymal lesions as well as pleural effusion. The intrapulmonary parenchymal lesions included air-space consolidation, nodular opacities, cystic lesions, and ground-glass opacities. Unilateral pleural effusion was observed in 12 patients (60%) and bilateral effusion in eight patients (40%). A small amount of pneumothorax was concomitantly observed in one patient (5%) (Table 2).
Examination of pleural effusion
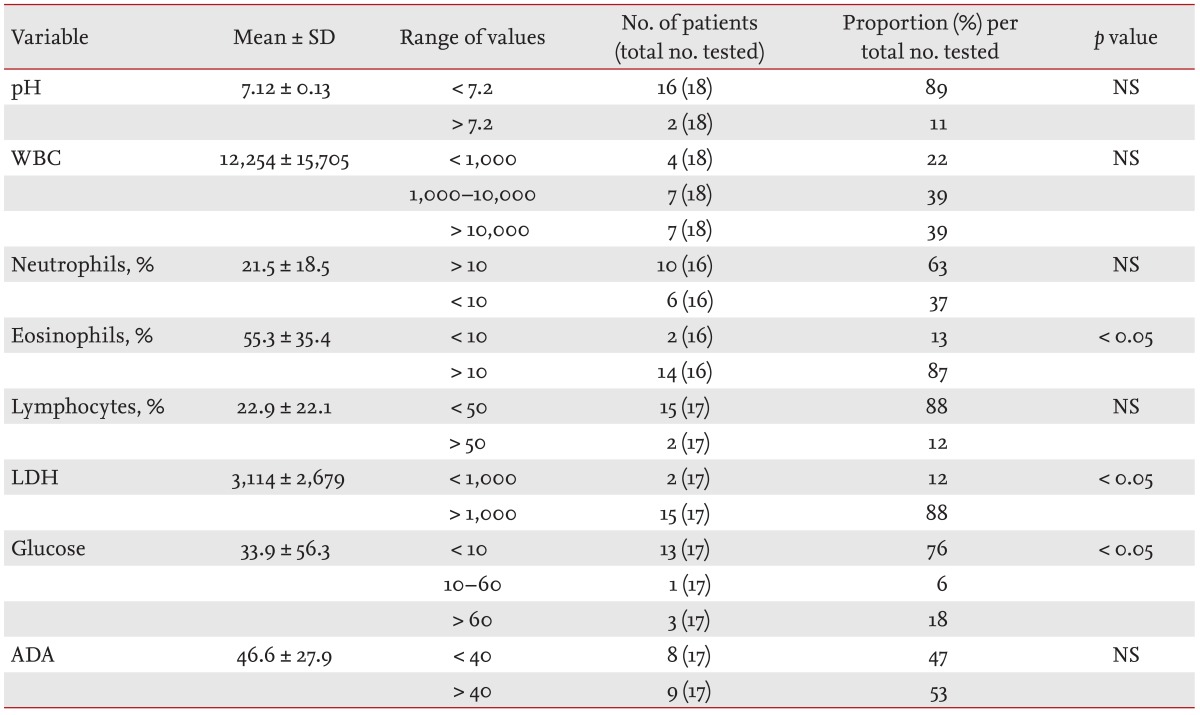
The pleural fluid samples obtained by thoracentesis appeared grossly turbid and yellowish (35%) or brownish (65%). The volume of the pleural fluid was < 1 L in most cases. On pleural fluid analysis, the mean lactate dehydrogenase (LDH) and glucose levels were 3,114 ± 2,679 U/L and 33.9 ± 56.3 mg/dL, respectively. The mean percentage of eosinophils in the pleural fluid was 55.3% ± 35.4%. The mean adenosine deaminase (ADA) level was 46.6 IU/L. The pleural effusion data are shown in detail in Table 3.
Confirmation of paragonimiasis
The diagnosis of paragonimiasis was confirmed based on a positive enzyme-linked immunosorbent assay result (80%) or by the identification of characteristic Paragonimus eggs in the pleural fluid (5%) (Fig. 1). One patient had a positive result for both tests. The remaining four patients were diagnosed clinically after other diseases had been ruled out.
DISCUSSION
The objective of this retrospective study was to describe how pleuropulmonary paragonimiasis with pleural effusion could be differentiated from other pleural diseases such as malignancy, parapneumonic effusion, and pleural tuberculosis. The cause of pleural effusion in patients with paragonimiasis is unclear and may involve pleural invasion by the organism with or without a hypersensitivity reaction. The prevalence of pleural effusion in patients with pleuropulmonary paragonimiasis has been reported to vary from 2.9% [15] to 69% [5]. However, a recent study of CXRs from patients with pulmonary paragonimiasis indicated that intrapulmonary parenchymal lesions were more common than pleural lesions [14,16]. Therefore, pleural effusion, when detected, was suspected to stem from causes other than pleuropulmonary paragonimiasis.
The classic symptoms of pulmonary paragonimiasis include fever, chest pain, and respiratory symptoms such as chronic cough with rusty-brown sputum or hemoptysis [6]. The majority of patients in this study exhibited dyspnea, hemoptysis, cough, and pleuritic chest pain and demonstrated consolidations and nodular opacities as well as pleural effusion on CXRs. More common causes of pleural effusion, including parapneumonic effusion, malignancy, and pleural tuberculosis, were preferentially suspected. The patients in our study had a median age of 43 years and did not for the most part exhibit signs of infection such as fever and peripheral leukocytosis; therefore, we suspected pleural tuberculosis rather than parapneumonic effusion and malignancy. Distinguishing between paragonimiasis and tuberculosis has frequently proven to be difficult and constitutes a diagnostic dilemma in regions in which tuberculosis and paragonimiasis coexist [17]. Peripheral blood leukocytosis was seen in 40% of the patients in this study. However, peripheral blood eosinophilia was observed in 70% of the patients. Although the degree of eosinophilia varies according to the stage of infection, its presence should increase the index of suspicion for paragonimiasis in the differential diagnosis of pleural effusion resembling pleural tuberculosis [5,9].
All patients with a newly discovered pleural effusion should undergo thoracentesis. Thoracentesis is required to ascertain the nature of the effusion and to differentiate it from manifestations of other conditions. The pleural fluid of patients with pleural tuberculosis is an exudate with a normal-to-low concentration of glucose, a pH of ~7.3 (occasionally < 7.2), and a predominance of lymphocytes [18]. AFB are seen on direct smears of pleural fluid in only 10% to 25% of cases of pleural tuberculosis. The pleural concentration of ADA is a more useful screening test for pleural tuberculosis. However, high ADA levels can also be found in pleural effusion secondary to pneumonia, empyema, or a neoplasm [19]. The determination of ADA and its isoenzymes can help to differentiate the causes of pleural effusion. Since ADA2 may be an indicator of monocyte/macrophage activation, increased ADA2 activity is a marker of pleural tuberculosis [20]. Increased ADA1 activity, on the other hand, is an indicator of parapneumonic effusions, especially originating from lymphocytes and monocytes. However, there may be little to be gained clinically by performing this additional difficult and costly step. Additional studies should be performed to investigate the diagnostic value of ADA and its isoenzymes in pleural effusion.
Most patients with pleuropulmonary paragonimiasis have significant eosinophilia in their pleural fluid [21,22,23], and their exudates have a low level of glucose (< 10 mg/L), a low pH (< 7.10), and a high level of LDH (> 1,000 IU/L). Although eggs may be present in the pleural fluid [21], they are usually not observed [9]. In this study, Paragonimus eggs were detected in only one patient. The major differences in the pleural fluid of patients with pleural tuberculosis and those with pleuropulmonary paragonimiasis are the proportions of lymphocytes and eosinophils and the LDH and ADA levels. In our study, the majority of patients with pleuropulmonary paragonimiasis had low levels of lymphocytes (< 50%), significant eosinophilia (> 10%), and high LDH levels (> 1,000 IU/L) in their pleural fluid. These are characteristic findings of pleural fluid analysis that can contribute to the diagnosis of paragonimiasis. The mean ADA level in patients with pleuropulmonary paragonimiasis was 46.6 ± 27.9; however, the results of pleural fluid testing in terms of lymphocyte, eosinophil, and LDH levels and the patients' histories were helpful in diagnosing pleuropulmonary paragonimiasis despite the elevated ADA levels.
The present study has several limitations, including its retrospective nature. It is possible that selection bias influenced the significance of our findings. Our study was from a single institution and has a small sample size, which limits the extension of our findings to the general population.
In conclusion, pleuropulmonary paragonimiasis with pleural effusion may be confused with other pleural diseases. Physicians should include pleuropulmonary paragonimiasis in their list of differential diagnoses for pleural effusion, especially for patients who live in or have travelled to areas in which pulmonary paragonimiasis is endemic. In patients with unexplained pleural effusion, pleural fluid should be obtained by thoracentesis. When the results of pleural fluid testing reveal marked eosinophilia, a high LDH level, and a low glucose level, physicians could consider a diagnosis of pleuropulmonary paragonimiasis.
KEY MESSAGE
Physicians should include pleuropulmonary paragonimiasis in their list of differential diagnoses for pleural effusion, especially for patients who live in or have travelled to areas in which pulmonary paragonimiasis is endemic.
In patients with unexplained pleural effusion, pleural fluid should be obtained by thoracentesis. When the results of pleural f luid testing reveal marked eosinophilia, a high lactate dehydrogenase level, and a low glucose level, physicians should consider a diagnosis of pleuropulmonary paragonimiasis.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





