


INTRODUCTION
Rheumatoid arthritis-associated interstitial lung disease (RA-ILD), the most common manifestation of rheumatoid lung disease [1], occurs more frequently in patients with severe RA. An autopsy study of 81 patients with longstanding RA revealed that 16% died of respiratory failure, while 34% exhibited signs of ILD [2]. Based on United States national mortality statistics, the prevalence of RA-ILD in RA patients is approximately 10% in females and 6% in males [3].
Despite possible adverse events, including infection, the efficacy of anti-tumor necrosis factor (anti-TNF) therapy for the treatment of RA has been established in several randomized controlled trials [4]. However, the effect of anti-TNF therapy on RA-ILD patients remains unclear. Improvements in pulmonary function, and radiographic stabilization, have been observed in RA patients following anti-TNF therapy [5]; however, ILD exacerbation following administration of an anti-TNF agent has also been reported [6,7]. Moreover, the mortality odds ratio (OR) was increased 4.4-fold in RA patients with pre-existing lung disease treated with biological agents versus those without lung disease [8]. The present, retrospective study investigates the causes of, and risk factors for, death in RA-ILD patients treated with anti-TNF agents.
METHODS
The medical records of 100 RA-ILD patients, treated in our tertiary care center between June 2004 and June 2011, were reviewed retrospectively. A total of 24 patients treated with anti-TNF therapy was selected. All patients were diagnosed according to the 1987 American College of Rheumatology (formerly the American Rheumatism Association) classification criteria for RA [9]. The study was approved by the Institutional Review Board of Asan Medical Center.
Patients exposed to environmental agents or drugs, or with other underlying disorders known to cause pulmonary fibrosis, were excluded. RA-ILD was diagnosed by a pulmonologist based on a combination of clinical presentation, pulmonary function testing, and the presence of bibasilar reticular abnormalities with minimal ground-glass opacities, on high-resolution computed tomography. In certain cases, bronchoscopy with bronchoalveolar lavage was performed.
The baseline characteristics of patients were assessed. In addition, the nonsurvivor and survivor groups were compared to determine the effects of anti-TNF therapy on mortality. Data pertaining to age at diagnosis of RA-ILD, sex, disease duration, comorbidities, lung function, treatment regimen, and the number of acute exacerbations of ILD were also analyzed; patients who died were studied in detail.
Baseline patient characteristics were compared using either a Mann-Whitney U or chi-squared test. Group comparison of ORs and corresponding 95% confidence intervals (CIs), for each variable, were calculated using univariate and multivariate analyses. A value of p < 0.05 was taken to indicate statistical significance. All analyses were performed using the SPSS version 17.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
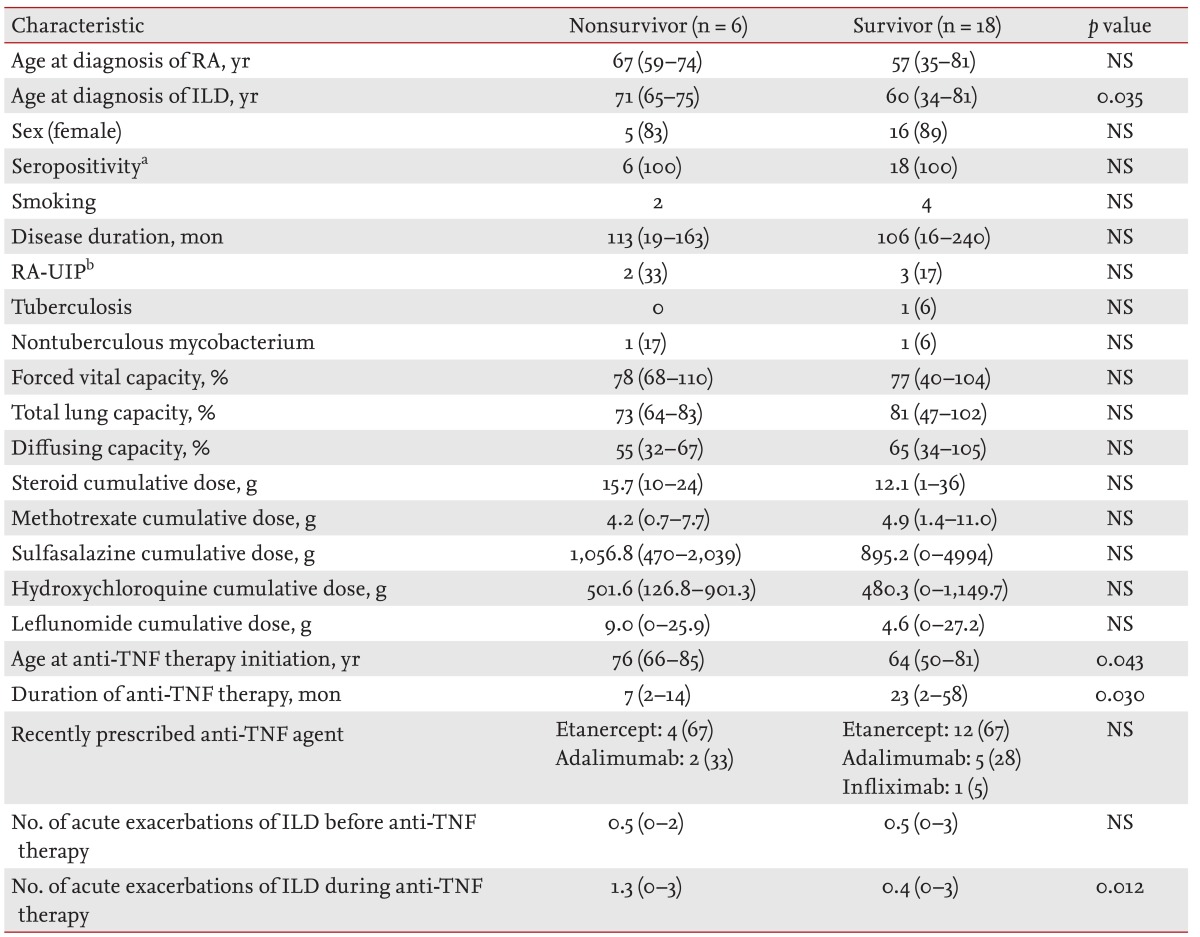
Of the 24 patients treated with anti-TNF therapy, six died (25%). The mean age at RA diagnosis was not significantly higher in the nonsurvivor versus survivor group (67 years [range, 59 to 74] vs. 57 years [range, 35 to 81], respectively) (Table 1). However, mean age at ILD diagnosis was significantly higher in patients who died (71 years [range, 65 to 75] vs. 60 years [range, 34 to 81], respectively; p = 0.035). There were more females in both groups and all patients were diagnosed as seropositive for RA. RA disease durations were similar between survivors and non-survivors (113 months [range, 19 to 163] vs. 106 months [range, 16 to 240], respectively). Five patients (three survivors and two nonsurvivors) were diagnosed with RA-UIP. Because no RA-ILD patients had undergone lung biopsy, their diagnoses were made according to clinical symptoms and imaging findings. Tuberculosis infection developed in one survivor, and one case of nontuberculous mycobacterium infection was observed in each group.
Pulmonary function test results at ILD diagnosis were analyzed, with no differences in the forced vital capacity of nonsurvivors versus survivors (78% [range, 68 to 110] vs. 77% [range, 40 to 104], respectively), nor total lung capacity (73% [range, 64 to 83] vs. 81% [range, 47 to 102], respectively), or diffusing capacity (55% [range, 32 to 67] vs. 65% [range, 34 to 105], respectively).
The cumulative dose of drugs, including steroids, methotrexate, sulfasalazine, hydroxychloroquine, and leflunomide was similar in both groups. However, mean age at anti-TNF therapy initiation was significantly higher in the nonsurvivor group (76 years [range, 66 to 85] vs. 64 years [range, 50 to 81], respectively; p = 0.043). The mean duration of anti-TNF treatment in the nonsurvivor group was shorter (7 months [range, 2 to 14] vs. 23 months [range, 2 to 58], respectively; p = 0.030). In both groups, the most common recently prescribed anti-TNF agent was etanercept.
Despite the shorter duration of anti-TNF treatment, a higher number of acute exacerbations of ILD following anti-TNF therapy was observed in the nonsurvivor versus survivor group (1.3 [range, 0 to 3] vs. 0.4 [range, 0 to 3], respectively; p = 0.012). However, there was no group difference in the number of acute exacerbations prior to anti-TNF therapy.
We analyzed risk factors for death using logistic regression (Table 2). In univariate analysis, the only risk factor for death was age at initiation of anti-TNF therapy (OR, 1.18; 95% CI, 1.01 to 1.39; p = 0.041). In multivariate analysis, no significant risk factor for death emerged.
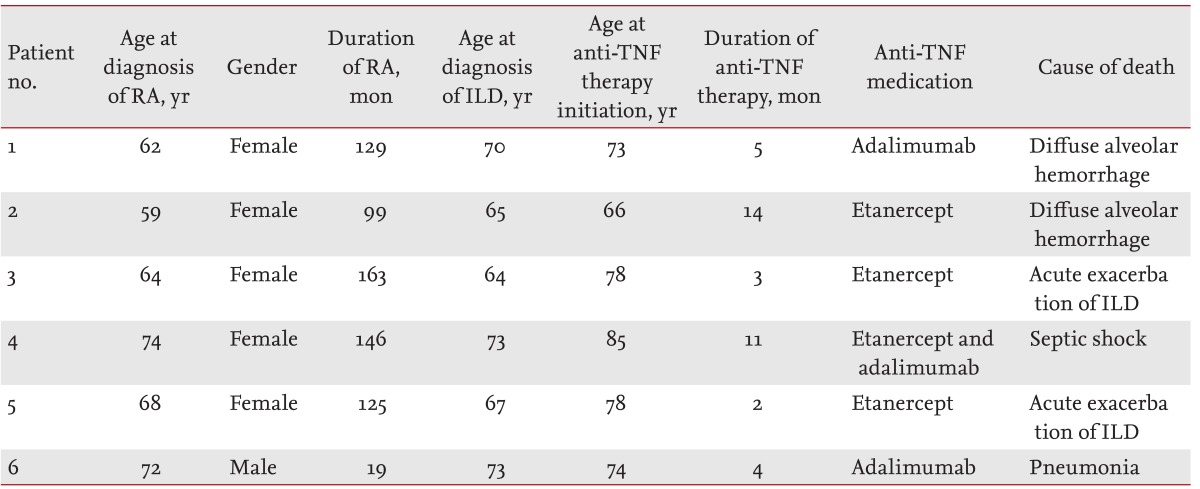
Patient clinical characteristics and causes of death are listed in Table 3; age at ILD diagnosis and initiation of anti-TNF therapy was Ōēź 64 years. Anti-TNF treatment duration ranged between 2 to 14 months. Patients 1 and 2, who died of diffuse alveolar hemorrhage, were treated with etanercept and adalimumab, respectively. Patient 3, who received adalimumab for 2 months following 9 months of etanercept treatment, died of septic shock following knee surgery. Patient 4, treated with etanercept for 3 months, died of acute exacerbation of ILD following knee surgery. Patients 5 and 6, who died of acute exacerbation of ILD and pneumonia, were treated with etanercept and adalimumab, respectively.
DISCUSSION
The safety and effectiveness of anti-TNF agents, for the treatment of RA, have been well-established in clinical trials and large cohort studies. The number of RA-ILD patients treated with anti-TNF agents continues to increase, due to the complications and treatment failures associated with disease-modifying anti-rheumatic drugs (DMARDs). However, it remains unclear whether anti-TNF agents are beneficial or detrimental to ILD patients; therefore, additional research is required.
Hagiwara et al. [6] reviewed a nine-case series in which RA-ILD developed following anti-TNF agent use: old age and preexisting ILD were risk factors for mortality in anti-TNF agent-induced ILD, which tends to occur shortly after treatment. The present, retrospective study determined the effects of anti-TNF treatment on mortality in RA-ILD patients. Preexisting ILD was documented in 23 of 24 patients (96%), of whom six died (26%). The majority of the deaths occurred in patients Ōēź 70 years of age, and within several months of initiating anti-TNF therapy. Although the OR, of age at anti-TNF therapy initiation for death, was not significant, our data indicates the possibility of severe complications in RA-ILD patients treated with anti-TNF agents.
The British Society for Rheumatology Biologics Register reported that RA-ILD mortality rate was not increased following treatment with anti-TNF therapy versus traditional DMARDs, but the proportion of deaths attributable to RA-ILD was higher in patients treated with anti-TNF agents [10]. In our study, five of six deaths (83%) were possibly related to lung complications; two patients died of diffuse alveolar hemorrhage, two of acute exacerbation of ILD, and one of pneumonia.
We also identified two diffuse alveolar hemorrhage cases, similar to previous reports [11,12]. Although the mechanism by which anti-TNF precipitates diffuse alveolar hemorrhage remains unclear, we speculate that hemorrhage of the lung may be particularly important.
In three patients Ōēź 70 years of age, the condition of whom failed to improve despite anti-TNF therapy (and who were subsequently treated with rituximab), attenuated RA progression without lung complications was observed. Rituximab can also induce radiographic stabilization and improved lung function in systemic sclerosis-associated ILD, suggesting a beneficial effect on B-cell depletion [13,14]. Further research is required to determine the safety of rituximab for RA-ILD patients.
Our study had several limitations: first, RA-ILD and fibrosis status differed among patients at anti-TNF therapy initiation, and older RA-ILD patients tended to be treated with etanercept to avoid possible infection.
In conclusion, anti-TNF agents should be prescribed cautiously in older RA patients predisposed to ILD, and physicians should be aware of the potential for lung-related complications in the first year of anti-TNF therapy.
KEY MESSAGE
The complications associated with anti-tumor necrosis factor (anti-TNF) therapy for rheumatoid arthritis-associated interstitial lung disease (RA-ILD) patients are still not well-established despite several randomized controlled trials.
Of 24 RA-ILD patients receiving anti-TNF therapy, six died (25%); their age at ILD diagnosis and anti-TNF therapy initiation was Ōēź 64 years.
Physicians should be aware of the potential for lung-related complications during the first year of anti-TNF therapy.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





