


INTRODUCTION
Providencia species are members of the Enterobacteriaceae and an uncommon cause of infections, unlike many other bacteria in this family. Among the species in this genus, Providencia stuartii and Providencia rettgeri are the most common causes of infections, especially urinary tract infections (UTIs), in hospitalized patients or nursing care facilities [1,2]. However, Providencia bacteremia is uncommon and few studies on the subject have been published [3,4,5]. Although the prevalence of Providencia bacteremia is low, proper empirical antibiotic therapy is important because Providencia species are often resistant to multiple antibiotics [6].
The purpose of this study was to investigate the clinical features, outcome of patients with Providencia bacteremia, and antibiotic susceptibility of Providencia species.
METHODS
Study design and patients
This cross-sectional study was conducted at a tertiary care university hospital in Wonju, Korea. Microbiology laboratory records were obtained for the period starting in May 2001 and ending in April 2013. Patients whose blood cultures grew Providencia species were identified and pertinent medical records were retrospectively reviewed. This study was approved by our Institutional Review Board (YWMR-13-05-037).
Identification and antimicrobial susceptibility testing
Identification and antimicrobial susceptibility testing for Providencia species were performed using the microplate method, VITEK 2 system (BioM├®rieux, Marcy l'├ētoile, France), or MicroScan WalkAway System (Siemens Healthcare Diagnostics, Sacramento, CA, USA). The results were interpreted according to Clinical and Laboratory Standards Institute guidelines [7]. Intermediate susceptibility to antibiotics was considered to be drug resistance.
Definitions
Providencia bacteremia was defined as the isolation of Providencia species from one or more blood culture sets in a patient having two or more systemic inflammatory response syndrome criteria [8]. All positive blood cultures taken within a 72-hour period were considered to represent the same episode. Nosocomial bloodstream infection was defined as a positive blood culture obtained 48 hours after admission with no evidence of infection at the time of admission, or if the infection was acquired at another hospital before transfer to the study hospital. Polymicrobial bacteremia was defined as more than one organism isolated from blood culture sets during one episode of bacteremia. The severity of underlying disease was classified into three categories according to the criteria of McCabe and Jackson [9]: rapidly fatal, ultimately fatal, and nonfatal. The severity of illness at the onset of bacteremia was assessed by the Pitt bacteremia score [10] and the Acute Physiologic and Chronic Health Evaluation (APACHE) II score. The source of bacteremia was determined on the basis of clinical data and a culture result that was positive for the same organisms. Primary bacteremia was defined as bacteremia without an apparent focus or portal of entry. Empiric antibiotic therapy was considered to be appropriate when at least one effective drug was included in the empirical regimen and the dose and pattern of administration were in accordance with current medical standards.
Statistical analysis
The descriptive analysis consisted of the absolute number (percentage) or median (range) for various parameters. Continuous variables were compared by the Mann-Whitney U test. Fisher exact test or the chi-square test was used to test whether differences existed between groups for categorical variables. For all analyses, p < 0.05 was considered to be statistically significant. All statistical analyses were performed using IBM SPSS version 20 (IBM Co., Armonk, NY, USA).
RESULTS
During the 13-year study period, 14 cases of Providencia bacteremia occurred. None of the patients had recurrent bacteremia. The incidence rate was 0.41 per 10,000 admissions. The occurrence of Providencia bacteremia was sporadic and showed no evidence of an outbreak during the study period.
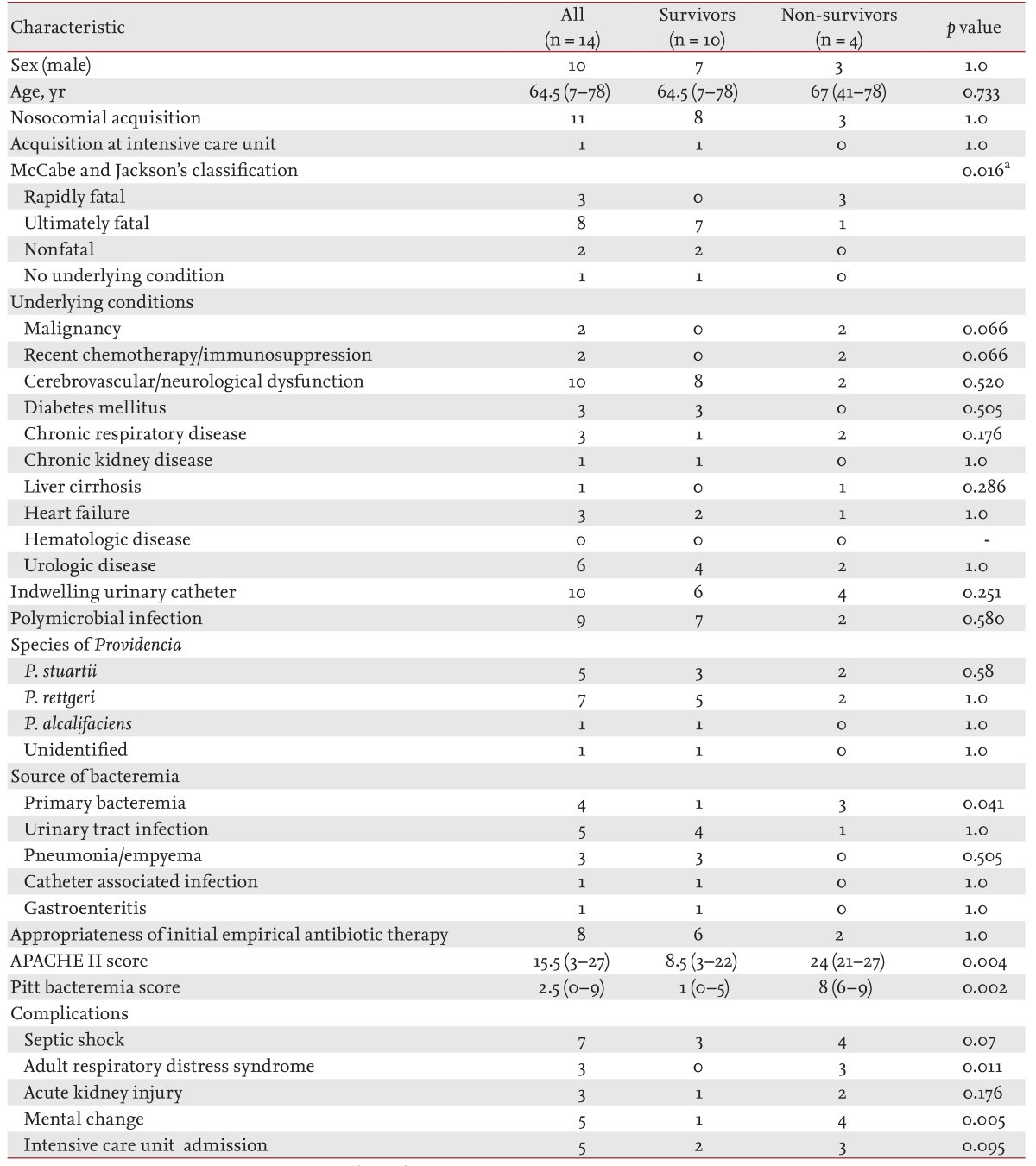
The demographic data and clinical characteristics of the patients are shown in Table 1. Ten of the patients (71.4%) were male. The median patient age was 64.5 years (range, 7 to 78). Seven patients (50%) were older than 65. Eleven cases (78.6%) were nosocomial infections, and only one patient developed bacteremia in the intensive care unit. One or more underlying conditions were present in 13 patients (93%): rapidly fatal (three patients), ultimately fatal (eight patients), and nonfatal (two patients). Cerebrovascular or neurological disease was the most common underlying disease (71.4%), followed by urologic disease (42.9%). Urinary catheters had been inserted in 10 patients (71.4%).
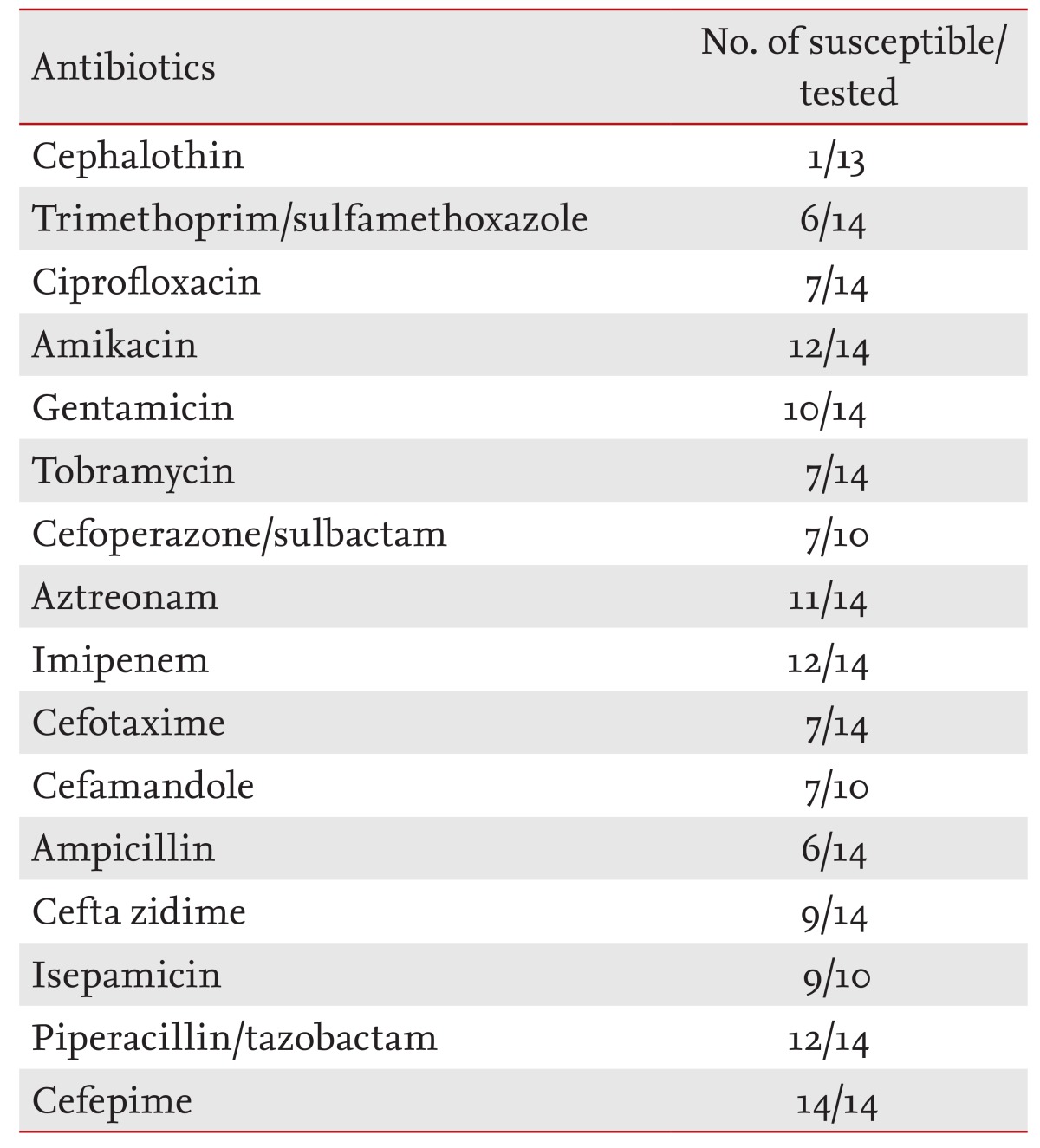
There were nine cases (64.3%) of polymicrobial bacteremia. In seven of these cases, only one other bacterium was isolated with Providencia: Escherichia coli (two patients), Streptococcus agalactiae (one patient), Pseudomonas aeruginosa (one patient), Enterococcus (one patient), viridans group streptococci (one patient), and Proteus mirabilis (one patient). Two additional organisms were isolated with Providencia in two patients: E. coli and Enterococcus (source of bacteremia: gastroenteritis), and P. aeruginosa and Burkholderia cepacia (source of bacteremia: central venous catheter). The most frequently isolated co-pathogen was E. coli (3/9, 33.3%). P. rettgeri was the most common species (n = 7, 50%), followed by P. stuartii (n = 5, 35.7%). The antimicrobial susceptibility testing results are shown in Table 2. The Providencia species in this study showed resistance to tobramycin but were susceptible to amikacin and isepamicin. Susceptibility to ciprofloxacin was only seen in 50% of the isolates. More than 80% of the isolated strains were susceptible to cefepime, imipenem, and piperacillin/tazobactam. The most frequently prescribed empirical antimicrobial was cefoperazone/sulbactam (seven patients); 70% of the isolated Providencia species were susceptible to cefoperazone/sulbactam.
The most common source of bacteremia was a UTI, followed by unknown sources. P. rettgeri was the most frequently isolated species in patients with a UTI or primary bacteremia (3/5 and 3/4, respectively). In contrast, 2/3 of pneumonia cases were due to P. stuartii. In one case of gastroenteritis, P. rettgeri was the responsible pathogen.
The overall in-hospital mortality was 28.6% (4/14). All of the nonsurvivors had rapidly fatal or ultimately fatal underlying conditions, and the underlying illness severity was significantly higher in nonsurvivors (p = 0.016). The most common underlying conditions were malignancy, recent chemotherapy or immunosuppressive therapy, cerebrovascular or neurological dysfunction, and urologic disease. All of the nonsurvivors had indwelling urinary catheters. Among the nonsurvivors, 50% had polymicrobial bacteremia. A fatal outcome was more common in patients with primary bacteremia than in those with other types of bacteremia (3/4 vs. 1/10, p = 0.041). All four of these patients died before antibiotic susceptibility results were available; three patients died within 48 hours and one patient died 4 days after the onset of bacteremia. Eight patients (57.1%) received appropriate empirical antibiotic therapy, while six did not. The appropriateness of the initial empirical antibiotic regimen was similar between the survivors and nonsurvivors. Since all of the nonsurvivors died within 4 days, we could not evaluate the appropriateness of the definitive therapy. The APACHE II and Pitt bacteremia scores on the day of blood culture were significantly higher in the nonsurvivors (p = 0.004 and p = 0.002, respectively). Complications such as septic shock, respiratory failure, and mental change developed more frequently in nonsurvivors (Table 1).
DISCUSSION
The genus Providencia of the family Enterobacteriaceae consists of five species: P. alcalifaciens, P. heimbachae, P. rettgeri, P. rustigianii, and P. stuartii. Among them, P. stuartii and P. rettgeri are most commonly associated with UTIs. They frequently colonize indwelling urinary catheters in nursing home residents and can cause hospital outbreaks [1]. However, Providencia bacteremia is uncommon. In a review by Woods and Watanakunakorn [4], the incidence of P. stuartii bacteremia was 0.17 per 1,000 admissions during a 12-year period. In a review by Kim et al. [5], the incidence of Providencia bacteremia was 0.16 per 10,000 admissions over a decade. Our study confirms that Providencia bacteremia is uncommon; however, the incidence rate in our study was three times higher than that in the review of Kim et al. [5], and four times lower than that in the review of Woods and Watanakunakorn [4]. Providencia species are ubiquitous and can be isolated from urine, the throat, perineum, axilla, stool, blood, and wounds in humans [1]. Among these specimen types, Providencia are most frequently isolated from the urine of elderly patients with urinary catheters. The reasons for the variable incidence of Providencia bacteremia are not apparent, but the types of patient and institution might contribute to such a difference. For example, the proportion of elderly patients in our hospital is higher than that in other urban areas in Korea.
Except for one study [5], the urinary tract was the most common source of Providencia bacteremia in previous studies (71% and 100%, respectively) [3,4]. In this study, the most common cause of bacteremia was a UTI. P. rettgeri and P. stuartii were the most common species. Almost all of the patients had urinary catheters. On the other hand, P. alcalifaciens and P. rettgeri have been suggested as a cause of diarrhea [11,12,13]. One patient with P. rettgeri bacteremia had gastroenteritis in this study.
The mortality rate for Providencia bacteremia is different according to various studies. In the reviews of Prentice and Robinson [3] and Woods and Watanakunakorn [4], the mortality rate for Providencia bacteremia was 33 and 24%, respectively. On the other hand, four out of eight patients (50%) with Providencia bacteremia died of the infection in a review by Kim et al. [5]. In this study, the mortality rate of bacteremia was 29%. We presume that this is due to differences in the sources of bacteremia included in the studies. In our study, primary bacteremia had the highest mortality rate (75%), while the mortality rate of UTI-associated bacteremia was 20%. In previous studies with lower mortality rates [3,4], a UTI was the source in 100% and 71% of cases, respectively. In a study by Kim et al. [5], primary bacteremia was the most common source of bacteremia; only two UTI-associated cases were included. Therefore, the mortality associated with Providencia bacteremia depends on the source of bacteremia, and the mortality rate for UTI-associated Providencia bacteremia is not high. Not surprisingly, the high mortality in patients with primary bacteremia and favorable outcome of urosepsis are consistent with previous studies of gram-negative bacteremia [14,15]. In contrast, all three patients with pneumonia survived.
The underlying disease severity was significantly higher in nonsurvivors. This finding emphasizes that host factors may play an important role in the outcome of patients with Providencia bacteremia.
In our study, cefepime, amikacin, isepacin, imipenem, and piperacillin-tazobactam had excellent activity against Providencia species. Virtually all Providencia species can produce inducible AmpC ╬▓-lactamases, and many isolates may also produce extended-spectrum ╬▓-lactamases in nosocomial settings [1,16]. Providencia species are intrinsically resistant to polymyxins and tigecycline, which are considered last resort antibiotics for resistant pathogens [17,18]. The susceptibility to ciprofloxacin also decreased from 100% to 46% over a 6-year period [19]. In a report by Kim et al. [5], 50% of the isolates were resistant to ciprofloxacin, similar to our findings. Plasmid-mediated resistance (e.g., extended-spectrum ╬▓-lactamases and metallo-╬▓-lactamases) has been reported in clinical isolates [16,20,21]. An outbreak of carbapenem-resistant P. stuartii due to a non-carbapenemase production mechanism was also reported [22]. The susceptibility of Providencia isolates should be closely monitored, and the treatment regimen should be guided by the susceptibility results. However, the mortality cases in our study died before the susceptibility test results were available. Limited antimicrobial options and the possible rapid progression of sepsis highlight the need for early detection in patients with Providencia bacteremia. New diagnostic technologies for the rapid detection of pathogens in the bloodstream (e.g., polymerase chain reaction, microarrays, and matrix-associated laser desorption/ionization time-of-flight mass spectrometry) are expected to reduce the time to organism identification. Moreover, effective infection control and antibiotic stewardship are emphasized to prevent the development of invasive infections and antibiotic resistance in Providencia species. In this study, most of the cases of Providencia bacteremia had nosocomial infections and urinary catheters. Therefore, urinary catheter infection control measures, including an avoidance of the routine use of urinary catheters, might reduce the risk of Providencia bacteremia.
Our study has some limitations. First, this is a cross-sectional study with a small number of patients conducted at a single university hospital in Korea. Therefore, well-designed large-scale studies are warranted. Second, a sequence analysis of the Providencia isolates was not performed; thus, we cannot exclude the possibility of misidentification. Third, more than half of the episodes in this study were polymicrobial bacteremia. We cannot exclude the effects of co-pathogens on clinical features and outcomes.
In summary, in this study, Providencia bacteremia was: (1) primarily due to a nosocomial infection occurring in elderly patients with cerebrovascular or neurologic disease; (2) frequently associated with indwelling urinary catheter use and a UTI; (3) more fatal in cases with primary bacteremia and severe underlying disease; and (4) frequently associated with polymicrobial infection, making the selection of appropriate empirical antibiotic therapy difficult.
KEY MESSAGE
Providencia bacteremia was primarily due to a nosocomial infection occurring in elderly patients with cerebrovascular or neurologic disease.
Providencia bacteremia was frequently associated with indwelling urinary catheter use and an urinary tract infection.
Providencia bacteremia was more fatal in cases with primary bacteremia and severe underlying disease.
Providencia bacteremia was frequently associated with polymicrobial infection, making the selection of appropriate empirical antibiotic therapy difficult.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





