


INTRODUCTION
Acute nonvariceal upper gastrointestinal bleeding (NVUGIB) is a commonly encountered medical emergency situation with a reported incidence that ranges from 50 to 150 cases per 100,000 adults per year [1-5]. NVUGIB carries a substantial mortality risk of 10%. In NVUGIB patients, esophagogastroduodenoscopy (EGD) plays a key role when investigating hemorrhage and the treatment of bleeding foci. However, inadequate visualization during emergency endoscopy precludes the identification of the bleeding focus and performing endoscopic hemostasis.
Erythromycin (EM), a motilin receptor agonist, accelerates gastric emptying by inducing gastric antral contractions that are similar to phase III of the interdigestive migrating motor complex [6-8]. EM has been administered to patients with diabetic gastroparesis. Recently, randomized controlled studies have shown that the infusion of EM prior to endoscopy effectively improves visualization and decreases the need for repeat EGD in patients with upper gastrointestinal (GI) bleeding [9-11]. The American College of Gastroenterology (ACG) recommends the intravenous infusion of 250 mg EM before emergent endoscopy for patients with upper GI bleeding, and gastric tube lavage is no longer recommended [12]. However, in many Asian countries, nasogastric tube placement and gastric lavage (GL) are routinely performed on patients presenting with melena or hematemesis. Furthermore, previously reported studies on the effects of administering EM prior to endoscopy in patients with upper GI bleeding were conducted in the United States and in European countries. Therefore, we performed our present pilot study to identify the effect of administering EM infusion in order to improve the quality of visualization during emergency endoscopy in Korean patients with NVUGIB.
METHODS
Study population
A prospective, randomized controlled trial was conducted. Patients > 20 years of age who presented with hematemesis or melena within 12 hours and were referred to the Emergency Department at Asan Medical Center between December 2012 and August 2013 were included. A stratified randomization procedure was used wherein randomization was stratified as hematemesis and melena. Patients were excluded for the following criteria: (1) known or suspicious liver cirrhosis; (2) known allergy to EM or other macrolides; (3) corrected QT (QTc) interval > 0.45 seconds on electrocardiography; (4) Glasgow Coma Scale score < 15; (5) systolic blood pressure < 90 mmHg and pulse rate > 110 beats/min despite fluid resuscitation; (6) the concomitant use of theophylline, warfarin, terfenadine, astemizole, carbamazepine, or cyclosporine because of possible interactions with EM; (7) prior gastrectomy; (8) hepatic dysfunction (aspartate transaminase or alanine transaminase ≥ 2× the normal upper limit); or (9) currently pregnant or lactating.
Study protocols
The eligible patients were randomly assigned to one of three groups: (1) the EM group (intravenous infusion of EM); (2) GL group (nasogastric tube placement with GL); or (3) EM + GL group (both EM infusion and GL). For EM infusion, 250 mg EM was mixed with 50 mL isotonic saline solution and intravenously administered over 30 minutes. Emergency endoscopy was performed 20 to 60 minutes after EM infusion. For GL, a 16-French nasogastric tube was positioned in the stomach and GL with 1L of tepid water was performed. GL was repeated every hour, and the endoscopic exam was performed within 30 minutes after the last gastric irrigation. All adverse effects were recorded during and after infusion or GL. All patients were underwent emergency endoscopy within 4 hours after arrival at the emergency department. An endoscopist, who was unaware of the assignment group, evaluated the quality of visualization during EGD and performed endoscopic hemostasis if the bleeding focus was identified. The method of hemostasis was chosen by the performing endoscopist. The patients who were treated with endoscopic hemostasis received an intravenous proton pump inhibitor for 72 hours.
The decision to admit the patient or not was made based on clinical implications. The results of the laboratory tests (white blood cell count, hemoglobin level, platelet count, prothrombin time, and blood urea nitrogen), the number of transfused blood units, instances of rebleeding, and mortality ratings on days 7 and 30 were recorded. The Glasgow-Blatchford score and pre-endoscopic and post-endoscopic Rockall score were calculated. The discharged patients who failed to attend their follow-up visit were contacted by telephone. The current study protocol was approved by the Institutional Review Board of the Asan Medical Center (No. 2012-0696). This clinical study was also approved by the Korean Food and Drug Administration (No. S2012-1361-0002). Written informed consent was obtained from each patient at the time of enrollment.
End points
The primary end point was the quality of GI visualization according the scoring system used by Frossard et al. [11]. An endoscopist scored each of the four areas of stomach and duodenum (fundus, corpus, antrum, and bulb) from 0 to 2 (0, < 25% of the surface was visible; 1, 25% to 75% visible; 2, > 75% visible). The total score was the sum of the scores for each of these four areas. Therefore, the score ranged from 0 to 8. A score ≥ 6 was considered satisfactory visualization, while ≤ 5 was considered unsatisfactory visualization. The secondary end points included the ability to identify the bleeding source, the success rate of hemostasis, duration of the emergency endoscopy, adverse effects related to EM infusion or GL, number of transfused blood units, rebleeding rate, and bleeding-related mortality.
Statistical analysis
The categorical variables are expressed as percentages and were compared between groups using the chisquare test and Fisher exact test. The quantitative variables are expressed as the mean ± standard deviation. Analysis of variance was conducted to compare the numerical variables between the three groups. Data that were not normally distributed were compared among groups using the Kruskal-Wallis test. Analyses were performed on an intention to treat basis and included all patients who underwent randomization. Statistical significance was established at p < 0.05. All statistical analyses were conducted using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
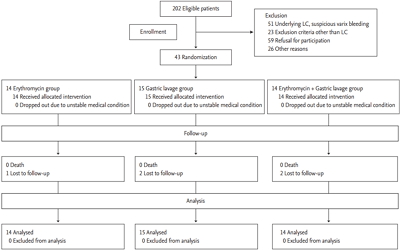
Fig. 1 shows the flow of the study patients. A total 202 patients were assessed for eligibility between December 2012 and August 2013. Of these patients, 43 patients were included in the study and randomized as follows: 14 patients were randomly assigned to receive EM alone before EGD; 15 patients were assigned to receive GL; and 14 patients were assigned to receive both EM and GL. All patients received the allocated interventions. Among these patients, 41 patients were followed for 7 days, and 38 patients were followed for 30 days.
Table 1 lists the baseline characteristics of the study population. The groups were well matched in terms of age, sex, and presenting symptoms. The onset time of bleeding, comorbidities, premedication, initial systolic blood pressure, initial diastolic blood pressure and pulse pressure, mean hemoglobin, and mean platelet counts did not significantly different between the three groups. Even though there was a significant difference between the three groups with regard to the mean prothrombin time (95% ± 10% in EM group, 88% ± 14% in GL group, and 106% ± 12% in the EM + GL group, p < 0.001), all values are within the normal range. For the patients in the GL group and in EM + GL groups, the mean number of performed GL was 1.4 (range, 1 to 3).
The endoscopic features and treatments in each group are presented in Table 2. The identification of the bleeding focus was possible in all patients. The mean duration of the endoscopic procedure, endoscopic findings, hemostatic treatments, and hemostatic methods did not significantly differ between the groups.
Table 3 indicates the primary and secondary end points. No statistical difference in terms of the median visualization score (interquartile range) was found between the three study groups. Although the percentage of patients with a satisfactory visualization score did not differ significantly between these three groups, it tended to be lower in the GL group. Each of the visualization scores of the three groups are shown in Fig. 2. The success rate of hemostasis was 100% (seven of seven patients) in the EM group, 85.7% (six of seven patients) in the GL group, and 100% (nine of nine patients) in EM + GL group. One patient in the GL group demonstrated spurting bleeding from the gastric ulcer base, and endoscopic hemostasis failed. He additionally underwent emergency angiographic embolization and was successfully treated. There were no complications associated with EM infusion or GL. Rebleeding occurred in three patients (one patient in each group). Bleeding-related mortality was not reported.
DISCUSSION
Our current study findings show that intravenous EM infusion may be of help to improve visualization during emergency endoscopy. Even though there were no statistically significant differences found between our three study groups, the percentage of satisfactory visualization in the EM infusion group was high at 92.9%, and that in GL group was low at 60.0%. Furthermore, additive GL after EM infusion did not show a clinical benefit over EM infusion alone. This implies that intravenous EM infusion alone can be effective enough to obtain satisfactory endoscopic view. A prospective multicenter randomized controlled trial in France reported results that are consistent with our current findings. When 253 patients with upper GI bleeding were randomly assigned to the EM infusion group without a nasogastric tube, nasogastric tube placement without EM, or intravenous EM infusion combined with nasogastric tube placement, overall satisfactory visualization was achieved in 85% of patients and the between-group differences were not significant [13]. Additionally, as the results of our current analyses show, the mean number of blood units transfused, the rebleeding rate, and the mortality rate did not significantly differ between the study groups. Several prospective randomized trials have reported the benefit of EM over treatment without EM infusion in patients with acute upper GI bleeding [9-11]. Satisfactory visualizations were achieved 65% to 90% of the patients who were treated with intravenous EM injection in those previous trials. In our present study, the percentage of patients who achieved satisfactory visualization was as high as 92.9%. The reason for this is likely that we excluded patients with unstable vital signs (systolic blood pressure < 90 mmHg and pulse rate > 110 beats/min) despite fluid resuscitation as these cases had the possibility of massive bleeding into the stomach.
Previously reported randomized controlled trials on the effects of EM prior to endoscopy in patients with upper GI bleeding were conducted in the United States and in some European countries [9-11,13,14]. Therefore, the guidelines for patients with upper GI bleeding in these countries recommend EM treatment prior to an emergency endoscopy. In 2012, ACG first recommended the intravenous infusion of 250 mg EM before emergent endoscopy for patients with upper GI bleeding [12]. The European Society of Gastrointestinal Endoscopy guidelines also recommend intravenous EM for patients with clinically severe or ongoing, active upper GI bleeding [15]. However, international consensus recommendations regarding the management of patients with NVUGIB do not recommend the routine usage of prokinetic agents before endoscopy in order to increase the diagnostic yield [16]. The Asian Pacific Working Group consensus on NVUGIB did not refer to the use of prokinetics, including EM, before emergency endoscopy [17]. Notably, nasogastric tube insertion and GL with normal saline are usually performed in many Asian countries to check for active bleeding and clear the stomach. Therefore, our current study is clinically significant in that it demonstrates the beneficial effects of EM treatment before emergency endoscopy in a Korean cohort.
In our current study series, we found no adverse events related to EM infusion. Allergic drug reactions to macrolides are known to be extremely rare [18]. As one of the most severe adverse events, QTc-interval prolongation is only likely to be a potential problem in patients with heart disease or other factors, or patients who are receiving agents that may further delay ventricular repolarization [19]. Drug interactions such as EM-induced digoxin toxicity are reported to occur when EM is repeatedly administrated [20,21]. No adverse events related to the use of EM before emergency endoscopy were reported in previous studies [9-11]. Hence, if high-risk patients are properly excluded, EM infusion can be safely used. Furthermore, EM infusion is a cost-effective treatment. In a previous study on the cost-effectiveness of EM infusion before EGD for patients with acute upper GI bleeding, EM prior to EGD resulted in a cost saving of US$486 and 0.00007 quality-adjusted life-years [22].
Our study had some limitations of note. First, we did not include patients with severe comorbidities or unstable vital signs, and this prevented conclusions about significant mortality-related differences between our study groups. Second, our patients underwent emergency endoscopy within 4 hours after arrival at the emergency department, and it is difficult to conduct an emergency endoscopy in clinical settings. However, our present analyses indicated beneficial effects of EM infusion before emergency endoscopy in a Korea population with well-defined end points of visualization.
In conclusion, intravenous EM infusion prior to emergency endoscopy for acute NVUGIB may be of help to provide satisfactory endoscopic visualization. Considering the potential adverse effects of clearing the stomach and the good safety profile of EM, nasogastric tube placement and GL can be replaced by EM infusion in patients with NVUGB.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





