


INTRODUCTION
Acute upper gastrointestinal bleeding (AUGIB) is an urgent medical situation due to its high morbidity and mortality rates. Despite advances in our medical knowledge and equipment technology, the mortality rates of nonvariceal AUGIB remain approximately 3% to 6% [1-3] and the mortality rate of variceal bleeding reaches 20% [4]. Endoscopic hemostasis reduces recurrent bleeding and the surgical treatment rate and improves the survival of patients with AUGIB. Therefore, endoscopic intervention has been established as one of the main therapeutic modalities for the management of AUGIB with recent bleeding stigmata [5-8]. However, when and which patients with presumed AUGIB should undertake endoscopy treatment are unclear [9-11]. Some studies have suggested that endoscopy within 12 hours of arrival at the emergency room may be beneficial according to the patientsŌĆÖ critical settings [12,13]. Conversely, several studies have reported that emergent endoscopy (within a few hours after presentation) showed no benefits in the mortality of AUGIB patients [5,12,14]. Some guidelines recommend early endoscopy (within 24 hours of presentation) in patients with nonvariceal AUGIB [8,15,16].
Two representative scoring systems are known to be associated with the prognosis, including the rebleeding rate and mortality. The pre-endoscopic Rockall scoring system includes age, pulse rate, systolic blood pressure, and comorbidities [17], whereas the Blatchford scoring system includes presentation with syncope or melena, systolic blood pressure, pulse rate, hepatic disease, cardiac failure, hemoglobin level, and blood urea nitrogen (BUN) [18]. However, the identification of patients who need to undertake urgent endoscopic hemostasis is difficult based on their histories, physical examinations, and simple blood tests without scoring and calculation. Moreover, emergent endoscopy may have many difficulties and dangers, especially during nonregular working hours due to less skilled endoscopy teams and higher fatigue of the endoscopists.
Thus, predicting the patients with presumed AUGIB who require urgent endoscopic hemostasis is very important. For these reasons, we conducted this study to assess easily applicable factors for the prediction of cases in need of an urgent endoscopic procedure prior to endoscopy.
METHODS
This retrospective study was conducted in Kangdong Sacred Heart Hospital, which is one of five Hallym University medical centers located in Seoul, Republic of Korea. The inclusion criteria were as follows: (1) presumed AUGIB patients (both nonvariceal and variceal bleeding) presenting with hematemesis, melena, and hematochezia within 7 days and (2) at least 15 years of age. The exclusion criteria were as follows: (1) lower gastrointestinal bleeding, (2) gastrointestinal cancer bleeding, and (3) bleeding patients who did not undergo esophagogastroendoscopy.
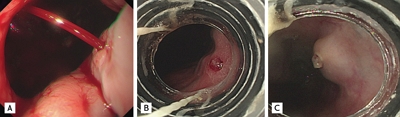
The consecutively included patients from September 2009 to December 2013 were divided into the endoscopic hemostasis and nonendoscopic hemostasis groups to evaluate simple predictive factors for endoscopic treatment. We defined the endoscopic hemostasis group as those who undergone endoscopic treatment because of spurting, oozing bleeding, or a protruding vessel with nonvariceal bleeding [19]. In case of variceal bleeding, the endoscopic hemostasis group was defined as those who undergone endoscopic treatment because of active bleeding, protruding vessel or white-nipple sign on varix as showed in Fig. 1.
The emergent endoscopy team of our hospital, which consists of one gastroenterologist, one resident trainee, and one endoscopy nurse, is on standby for AUGIB control every day. Endoscopic dual hemostasis was performed with epinephrine injection, hemoclipping, and/or argon plasma coagulation in the endoscopic hemostasis group of nonvariceal bleeding based on the decision of the gastroenterologist performing the endoscopy. One to three sessions of sclerotherapy (histoacryl 1 cc + lipiodol 1 cc/session), or band ligation was performed in the variceal bleeding patients with active bleeding or recent bleeding stigmata. The endoscopic timing was defined as the interval between the hospital visit and starting the endoscopy.
Nasogastric lavage (NGL) was performed at emergency room except the patients who refuse this procedure. About 1 L saline lavage and drainage was conducted via Levin tube after inserting in stomach. After endoscopic hemostasis, high dose proton pump inhibitor (PPI) continuous infusion (pantoprazole 8 mg/hr intravenous infusion for 72 hours after 80 mg intravenous loading) was performed. In case of nonendoscopic hemostasis patients underwent daily-standard dose PPI infusion for 24 to 72 hours. In variceal bleeding, 17 times injection of telipressin 1 mg per 4 hours after 2 mg loading and ceftriaxone 2 g/day for 5 to 7 days injetion was performed regardless of endoscopic hemosasis. Restart of antiplatelet agents or anticoagulants were recommended in 3 to 14 days after initial endoscopy based on the individual risk of rebleeding and thromboembolic event. The patients who had rebleeding was defined as follows: (1) active bleeding during the second-look endoscopy within 48 hours after initial hemostasis, (2) overt hematemesis, (3) passage of fresh blood from the rectum, and (4) a fall in the hemoglobin concentration of > 2 g/dL after the initial endoscopic hemostasis. Overall mortality was defined as death of any cause occurring during the hospital stay.
We reviewed the enrolled patientsŌĆÖ medical records and analyzed various variables, including comorbidities, medication history, symptoms, vital signs, laboratory findings, and parameters for the outcomes of AUGIB, such as the hospital stay, blood transfusion, surgery, rebleeding rate, and overall mortality.
This study protocol including exemption of informed consent was approved by the Institutional Review Boards of Hallym University Kangdong Sacred Heart Hospital (IRB N0:10-091).
Statistical analysis
The univariate analysis was performed to compare the clinical features or laboratory findings at initial presentation between the endoscopic hemostasis and nonendoscopic hemostasis groups using the chi-square test for categorical variables and the independent sample t test for continuous variables. Multivariate logistic regression analysis was used to assess the independent factors predicting endoscopic hemostasis patients. We used receiver operating characteristic curves to set the cut-off values for the continuous variables. The p values less than 0.05 were considered statistically significant.
All statistical analyses were performed with IBM SPSS for Windows version 19.0 (IBM Corp., Armonk, NY, USA).
RESULTS
A total of 613 patients were analyzed, including 329 patients in the endoscopic hemostasis group and 284 patients in the nonendoscopic hemostasis group. The baseline characteristics of each group are shown in Table 1. No significant differences in age and gender were observed between the two groups. Regarding comorbidities, liver cirrhosis (38% vs. 20%, p < 0.0001) and cancer (11% vs. 5%, p = 0.008) were presented more frequently in the endoscopic hemostasis group than in the nonendoscopic hemostasis group. Interestingly, the proportion of patients using aspirin, other antiplatelet agents, warfarin, or nonsteroidal anti-inflammatory drugs did not differ between the groups (Table 1).
The presence of hematemesis and syncope (including presyncope) as an initial symptom occurred more in the endoscopic hemostasis group than in the nonendoscopic hemostasis group (60% vs. 47%, p = 0.002 and 4% vs. 1%, p = 0.037, respectively). However, other symptoms, such as melena, hematochezia, dizziness, or epigastric pain, showed no significant differences between the two groups. The rate of positive findings in the digital rectal examination was not significantly different between the groups, whereas fresh blood was aspirated from the NGL more frequently in the endoscopic hemostasis group than in the nonendoscopic hemostasis group (126/204 [61.7%] vs. 40/206 [19.4%], p < 0.0001). The systolic and diastolic blood pressure was significantly lower in the endoscopic hemostasis group than in the nonendoscopic hemostasis group (101.5 ┬▒ 25.6 mmHg vs. 110.8 ┬▒ 22.0 mmHg, p < 0.0001 and 61.7 ┬▒ 21.2 mmHg vs. 69.7 ┬▒ 15.9 mmHg, p < 0.0001, respectively). However, the heart rate was not significantly different between the groups.
In the laboratory findings at presentation, the hemoglobin (8.9 ┬▒ 2.7 g/dL vs. 9.9 ┬▒ 3.2 g/dL, p < 0.0001), platelet count (190.0 ┬▒ 103.4 ├Ś 103 vs. 240.2 ┬▒ 126.8 ├Ś 103, p < 0.0001), international normalized ratio (1.4 ┬▒ 1.0 vs. 1.3 ┬▒ 0.9, p = 0.019), and BUN (37.0 ┬▒ 23.1 vs. 33.1 ┬▒ 23.4, p = 0.037) were significantly different between the groups. The endoscopic timing for the endoscopic hemostasis group was shorter than the timing for the nonendoscopic hemostasis group (3.9 ┬▒ 6.6 hours vs. 5.7 ┬▒ 10.1 hours, p = 0.010).
The endoscopic diagnoses of the included patients are shown in Table 1. A total of 321 patients (52.4%) had a peptic ulcer, 182 patients (29.7%) had varix, 58 patients (9.5%) had Mallory-Weiss tearing, and 52 patients (8.4%) had other diagnoses, such as hemorrhagic gastritis and angiodysplasia. Variceal bleeding was present at a higher proportion in the endoscopic hemostasis group than in the nonendoscopic hemostasis group (42% vs. 16%, p < 0.0001), whereas the other diagnoses did not significantly differ between the groups.
The outcomes of patients with AUGIB are shown in Table 2. A total of 65 patients (11%) had rebleeding, including 46 in the endoscopic hemostasis group and 19 in the nonendoscopic hemostasis group (14% vs. 7%, p = 0.003). The number of transfusions within 24 hours was significantly different between the groups (3.4 ┬▒ 2.9 units vs. 2.0 ┬▒ 1.9 units, p < 0.0001). The lengths of the hospital stays were also longer in the endoscopic hemostasis group (11.3 ┬▒ 9.5 days vs. 9.7 ┬▒ 9.7 days, p =0.033). In our series, 56 patients (9.1%) eventually died at the hospital, including 38 in the endoscopic hemostasis group (27 with varix bleeding and 11 with peptic ulcer bleeding) and 18 in the nonendoscopic hemostasis group (one with pneumonia, six with sepsis, four with cancer progression, six with cardiovascular disease, and one with pulmonary alveolar hemorrhage) (12% vs. 6%, p = 0.026).
The risk factors associated with endoscopic hemostasis in the univariate analysis were used to perform the multivariate analysis. The results of multivariate analysis for independent predictive variables of endoscopic hemostasisis were shown in Table 3. A bloody NGL (adjusted odds ratio [AOR], 6.786; 95% confidence interval [CI], 3.990 to 11.543; p < 0.0001) and hemoglobin < 8.6 g/dL (AOR, 1.768; 95% CI, 1.028 to 3.039; p = 0.039) were independent predictors of endoscopic hemostasis.
When a hemoglobin cut-off value of < 8.6 g/dL was used, the sensitivity was 47%, the specificity was 63%, the positive predictive value (PPV) was 59%, and the negative predictive value (NPV) was 51%. A bloody NGL, which was another independent factor for endoscopic hemostasis, showed a sensitivity of 62%, specificity of 81%, PPV of 76%, and NPV of 68% (Table 4).
To determine how well these variables predicted the need of endoscopic hemostasis, we developed predictive groups based on the number of predictive factors (bloody NGL and hemoglobin < 8.6 g/dL). When no predictors were present, 39.3% (97/247) of the patients underwent endoscopic hemostasis. A significant difference in the morbidity rates of endoscopic hemostasis group were observed between the group with no predictive factors and the group with one or more predictive factors (OR, 2.677; 95% CI, 1.920 to 3.733; p < 0.0001) (Table 5). The percentage of patients with endoscopic hemostasis increased with the number of predictive factors (59.9% [184/307] and 81.4% [48/59] in the one to two predictive factor group, p < 0.0001).
DISCUSSION
We cannot diagnose the exact causes of presumed AUGIB prior to endoscopy. The decision concerning the optimal timing to perform an endoscopy in patients with AUGIB is one the most important concerns after medical resuscitation. Thus, this study focused on predictors that could easily predict ongoing AUGIB, which is needed to prompt endoscopic hemostasis in a preendoscopy setting. The independent predictors of endoscopic hemostasis were a bloody NGL and hemoglobin less than 8.6 g/dL. The OR of endoscopic hemostasis was 2.677 in patients who had these predictors compared with patients who had no predictors. Importantly, the presence of more predictors in AUGIB patients indicated an increased risk of endoscopic hemostasis.
The good PPV (76%) of a bloody NGL can be interpreted that patients with fresh-blood drainage from a NGL need to undergo prompt endoscopic hemostasis. Some previous studies reported that a bloody NGL could predict high-risk bleeding stigmata or a high rebleeding rate [13,20-22]. For example, one study documented that 45% of patients with a bloody NGL compared to only 15% of patients with a clear NGL had high-risk bleeding stigmata on endoscopy [20]. A recent meta-analysis reported that an NGL with red blood increased the likelihood (likelihood ratio, 3.1; 95% CI, 1.2 to 14.0) of a severe AUGIB requiring urgent intervention [23]. Therefore, an international consensus has recommended considering NGL in selected patients for a pre-endoscopy workup due to its possible prognostic value [8]. However, Korean guideline [16] reported that NGL has limitation because NGL is an uncomfortable procedure for patients, has a high false-negative rate, and does not reduce the mortality rate [24].
A low hemoglobin level has been reported as one of the predictors for urgent endoscopy in previous studies [23,25,26]. A recent meta-analysis reported that the likelihood ratio of severe AUGIB ranged between 4.5 and 6.2, with a cut-off hemoglobin level of 8 g/dL [23]. One study with 3,386 patients with bleeding peptic ulcers after initial hemostasis reported that a hemoglobin level < 10 g/dL was one predictive values for rebleeding (OR, 1.87; 95% CI, 1.18 to 2.96) [25].
Two typical risk scoring systems (the pre-endoscopy Rockall and Blatchford scores) are used to predict the prognosis of AUGIB prior to the index endoscopy. However, neither the pre-endoscopy Rockall score nor the Blatchford score were useful for predicting the need for endoscopic therapy. The Blatchford score had a role only in identifying patients who might not require endoscopic hemostasis [27]. Furthermore, neither of these scoring systems could predict rebleeding [1].
Our study has some strengths. We included detailed demographic factors, comorbidities, symptoms, signs, and laboratory findings to better adjust for potential confounders. Second, our predictors can be acquired within 1 hour without calculation of prognostic scales in the emergency room in patients with not only nonvariceal bleeding but also with variceal bleeding. This ability would enable prompt decision making for urgent endoscopy.
This study also has some weaknesses. First, inevitable selection bias may be present. However, we enrolled AUGIB patients consecutively to minimize this selection bias, and all patients underwent endoscopy as soon as possible if their vital signs were maintained without active infection. Indeed, our study demonstrated that the endoscopic hemostasis group had a significantly worse prognosis based on the transfusion requirements within 24 hours, rebleeding rate, duration of hospital stay, and in-hospital all-cause mortality (Table 4), which was similar to the findings in previous studies [5,28]. Therefore, we believe that our predictors could be meaningful, reliable, and clinically applicable factors despite selection bias, although a prospective and randomized study is warranted to confirm the usefulness of NGL and hemoglobin in patients with AUGIB. Second, we may have another bias from the differences of the gastroenterologistsŌĆÖ skill and relatively small sample size for analyzing retrospective data.
In conclusion, a fresh bloody NGL and hemoglobin < 8.6 g/dL might be useful, easily applicable, and independent predictors for endoscopic hemostasis in patients with AUGIB.
KEY MESSAGE
1. A fresh bloody nasogastric lavage and hemoglobin < 8.6 g/dL might be useful, easily applicable, and independent predictors for endoscopic hemostasis in a pre-endoscopy setting.
2. The odds ratio of endoscopic hemostasis was 2.677 in patients who had these predictors compared with patients who had no predictors.
3. The presence of more predictors indicated an increased risk of endoscopic hemostasis.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





