


INTRODUCTION
Pulmonary arterial hypertension (PAH) is a disease with elevated mean pulmonary arterial pressure (mPAP) and pulmonary vascular resistance that eventually results in right ventricular heart failure [1-6]. Over the past two decades, there have been great advances in PAH treatment due to the advent of targeted therapies modulating the three classical pathophysiological pathways: the nitric oxide (NO), endothelin, and prostacycline pathways. However, poor prognoses for PAH patients remain a reality despite advances in treatment [7-13]. In addition, late detection and poor governmental support for aggressive, targeted therapy have constituted an obstacle for effectively treating this disease [10,12,14,15]. In this article, we review past and current challenges as well as future directions in the treatment of PAH in Korea.
EARLY INITIATIVES FOR A NATION-WIDE PAH REGISTRY
Due to the rarity of PAH, nation-wide efforts to document PAH characteristics among Koreans were not made until the late 2000s. Several single-center studies were published showing better prognoses for idiopathic PAH (IPAH) patients with vasoreactivity and targeted therapy [16-18]. The advent of targeted therapies, however, imposed the need to develop a nation-wide approach to oversee and manage PAH patients. Accordingly, four academic societies in Korea (The Korean Society of Cardiology, The Korean Academy of Tuberculosis and Respiratory Diseases, The Korean College of Rheumatology, and The Korean Pediatric Heart Society) collaborated to design a joint registry for PAH patients in Korea. The Korean Registry of Pulmonary Arterial Hypertension (KORPAH) enrolled 625 patients (328 patients previously diagnosed [prevalent] and 297 patients newly diagnosed [incident]) between 2008 to 2011 across 35 tertiary centers [9].
DEMOGRAPHICS AND ETIOLOGY OF KOREAN PATIENTS
For the total patient population enrolled in KORPAH, either incident or prevalent, 80.5% of PAH patients were women and the mean age at enrollment was 47.6 ┬▒ 15.7 years [9]. The percentages of congenital heart disease-related PAH (CHD-PAH), connective tissue disease-related PAH (CTD-PAH), and heritable PAH (HPAH) were 25.4%, 49.8%, and 23.2%, respectively, among the total cohort [9]. The proportion of patients diagnosed with right heart catheterization (RHC) was 40%. For incident patients who were first diagnosed during the enrollment period, the mean age was 50.0 ┬▒ 16.6 years and 78.5% were female [9]. Interestingly, up to 57.6% of the incident population had CTD-PAH. Authors explained this high percentage by the possible overestimation of mPAP for CTD-PAH patients being evaluated by echocardiography and not RHC [9]. The baseline demographic, clinical, and hemodynamic properties were similar to those registries from the USA, France, Spain, and China as shown in Table 1 [8,9,11-13]. The proportion of patients with New York Heart Association (NYHA) class III/IV heart failure was 48.7%, which was lower than other international registries, probably due to the aggressive screening procedures for the CTD-PAH population during enrollment (Table 1) [19].
PAH THERAPY AND SURVIVAL
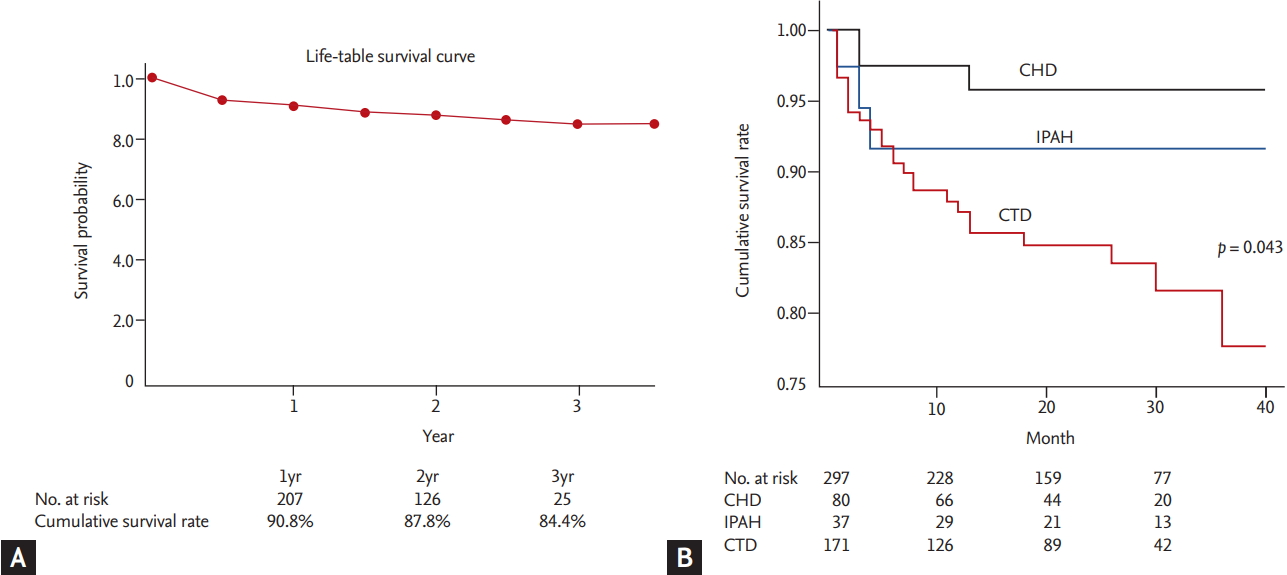
Among the 297 patients who were first diagnosed during the 2008 to 2011 enrollment, only 61.3% of patients were treated by PAH-specific medical therapies [9]. Of those, 154 patients (84.6%) received single medications (Table 2). Strikingly, only 28 patients (15.4% of the patients on PAH-specific therapy) received combination therapy, a mere 9.4% of the newly diagnosed population [9]. The mean time to follow-up was 1.7 years among the 297 incident cases, and 35 mortalities occurred [9]. The cumulative patient survival is shown in Fig. 1A. The 1-, 2-, and 3-year cumulative survival rates were 90.8%, 87.8%, and 84.4%, respectively [9]. The 3-year survival rate was relatively high compared to other registries, probably due to the low percentage of NYHA III/IV heart failure patients at enrollment (Table 1) [9,19]. Fig. 1B shows that patients with CHD-PAH had the highest survival rate (p = 0.043), followed by IPAH and CTD-PAH, which were consistent with the findings of other studies [9,20,21].
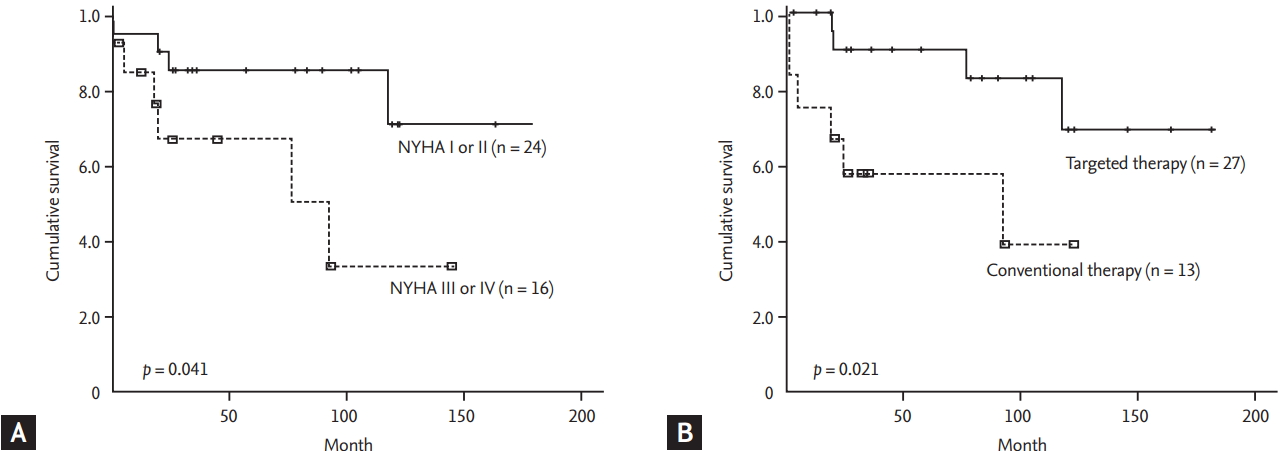
Interestingly, when survival data of a Korean single-center study were analyzed based on initial World Health Organization (WHO)-NYHA class, an incremental decrease in survival was noted along with increasing WHO-NYHA class (p = 0.041), as shown in Fig. 2A [18]. The survival data were additionally analyzed in terms of the type of treatment (Fig. 2B), where targeted therapy showed significantly improved survival compared with conventional therapy (p = 0.021) [18].
HEALTH INSURANCE DATA FOR PAH IN KOREA
Health insurance data on the epidemiology of PAH in Korea were also analyzed [22]. Data from 2008 to 2016 were analyzed based on International Classification of Diseases (ICD) codes, and a total of 1,307 new patients were diagnosed during this period. Similar to the KORPAH data, the mean age was 44 ┬▒ 12 years and 69.3% were women [22]. IPAH was defined as patients with pulmonary hypertension (ICD codes I27.0 and I27.2) who did not have ICD codes for other underlying diseases such as left-sided heart disease, CTD-PAH, CHD-PAH, human immunodeficiency virus, schistosomiasis, or chronic hemolytic anemia [22]. IPAH was the most common diagnosis (51.6%) in the pulmonary hypertension population, followed by CHD-PAH (25.8%), and CTD-PAH (17.2%) [22]. Bosentan monotherapy was the most frequently prescribed treatment [22]. Consistent with the findings of the KORPAH registry, only 18.4% of patients received combination therapy, among which a combination of bosentan and beraprost was most common (32.9% of all combination therapies) [9,22]. The 3- and 5-year survival rates were 54% and 46%, respectively [22]. This is significantly lower compared to the KORPAH registry data, where the 3-year survival rate was 84.4% [9]. The actual 3-year survival of Korean PAH patients may lie between 54% and 84.4%, as other modern registry data have shown a 3-year survival between 60% and 70% [19].
LESSONS FROM KORPAH AND OTHER COHORTS
The key messages that we have learned from Korean cohorts were: (1) the low performance rate of RHC may contaminate data, and (2) early detection and targeted therapy show better overall survival. The current trend in PAH therapy points to early, aggressive, combination therapy in patients with high risk symptoms [1,23,24]. Although the KORPAH did not stratify patients via a risk assessment, worse outcomes were associated with patients with severe symptoms (Fig. 2A) and better survival was seen in patients treated with PAH-specific therapy (Fig. 2B). This suggests that risk stratification and early combination therapy should be adopted in the future [1,18,23,24].
GENETICS OF KOREAN PAH PATIENTS
A family history of PAH has been shown to be associated with the onset of 6% to 10% of patients without other underlying pathology [25]. In the Korean population, heterozygous germline mutations of BMPR2, a gene encoding bone morphogenetic protein receptor type 2, are highly prevalent [26,27]. It has recently been demonstrated that the BMPR2 mutation is the most common gene mutation in all categories of PAH, with a 70% to 80% incidence in HPAH and 10% to 20% in IPAH [28]. Other identified gene mutations with a high level of incidence include EIF2AK4, TBX4, ATP13A3, GDF2, SOX17, AQP1, ACVRL1, SMAD9, ENG, KCNK3, and CAV1 [29].
To identify genetic characteristics of the Korean PAH population further, a prospective, investigator-initiated, and multi-institutional cohort study named the Effect of BMPR-2 Gene Mutations on Hemodynamic Response by Iloprost Inhalation in Pulmonary Arterial Hypertension (PILGRIM) trial was conducted (NCT01054105, clinicaltrials.gov) [30]. The primary objective of this study was to examine the prevalence of BMPR2 mutations and identify differences in hemodynamics between patients with or without BMPR2 mutations [30]. Patients diagnosed with either IPAH or HPAH were enrolled between 2010 to 2016 from 12 participating tertiary hospitals. A total of 73 patients who were thought to have IPAH were enrolled, among whom, seven patients were later identified as having HPAH. An additional 17 family members of seven HPAH patients were also enrolled [30]. Out of the 73 patients enrolled in the study, 16 patients (21.9%) had BMPR2 mutations [30]. The prevalence of BMPR2 mutations seen in IPAH/HPAH patients is consistent with the findings of other groups [31-36].
CURRENT PAH TREATMENT STRATEGIES AND FUTURE DIRECTIONS
Over the past decade, we have seen the emergence of novel pharmacotherapeutic developments for the treatment of PAH. Drugs that target the classical PAH pathways have been validated by randomized trials. The phosphodiesterase inhibitors (PDEi) that modulate the NO pathway, endothelin receptor antagonists that inhibit the endothelin pathway, or prostacyclin analogues (PCA) that activate the prostacyclin pathway have all been shown to have clinical benefits. The most recently approved drugs, macitentan [37], riociguat [38], and selexipag [39] and their corresponding clinical trial results are summarized in Table 3. The most notable trend is the evidence-based migration to combination therapy from monotherapy in newly diagnosed patients [40]. This has been reflected in current PAH treatment guidelines that promote starting combination therapy as early as possible, especially in high risk patients.
The efficacy of combination therapy in PAH treatment has long been debated. Sequential combination refers to adding on a second PAH-specific treatment as needed, whereas initial or upfront combination therapy indicates initiation of combination PAH-specific therapy in treatment-naïve patients. The efficacy and safety of sequential combination therapy has been shown by many randomized clinical trials [37,41-48], and is well reflected in current guidelines [1,4,6] and medical practices in Korea [9]. Although initial combination therapy has been shown to be efficacious and safe in smallscale, retrospective studies [49], there were no randomized clinical trials conducted until recently. A Study of First-Line Ambrisentan and Tadalafil Combination Therapy in Subjects With Pulmonary Arterial Hypertension (PAH) trial is the first trial to show the results of initial combination therapy in patients with PAH (Table 3) [40]. It showed that an initial double combination therapy of ambrisentan (10 mg) and tadalafil (40 mg) once a day respectively, was superior to monotherapy or placebo. These findings were also replicated with scleroderma-associated PAH patients (Table 3) [50]. Japanese registry data have also shown a significant hemodynamic benefit with initial combination therapy over monotherapy (Table 3) [51,52]. Similar to these trends, a high dose of epoprostenol, a well-established PCA treatment for severe PAH patients, soon after the initiation of treatment has shown very promising results in a study by a pioneering Japanese group [53]. These results collectively suggest that initial com bination therapy together with high-dose epoprostenol may be the future direction of PAH therapy.
The PAH treatment strategies in Korea are based on monotherapy or sequential combination therapy. As Koreans and Japanese share significant ethnic similarities, it may be acceptable for Korean specialists to adopt aggressive, initial combination therapies that are suggested by Japanese medical groups [51,52]. The major obstacle to implementing such practices is that of the strict regulations instituted toward initial combination therapy by the current Korean health insurance system, which is in contrast to the situation in Japan and other countries where regulations are less strict [4,54]. Additionally, the most efficacious drug, epoprostenol, is currently not marketed in Korea, which limits the options for early, aggressive treatment strategies (Table 4). Collaborative efforts between governmental authorities and pharmacological companies are currently underway to bring epoprostenol to Korea so that early aggressive PAH therapies become an available option.
LIFESTYLE MODIFICATION AND BETTER SUPPORTIVE CARE
As patient survival has improved, lifestyle modification and better supportive care have become equally important in PAH [55] as it is the case with other chronic diseases [56-59]. Lifestyle modification and supportive care have been overlooked in PAH because it has previously been considered untreatable. Exercise-based rehabilitation has been shown to improve quality of life in PAH patients [60]. European Society of Cardiology guidelines recommend patients consult with PAH specialists for exercise rehabilitation recommendations [1].
In PAH patients, iron levels have been shown to be decreased [61]. Although there are no randomized trial data, a single high-dose iron supplement has been suggested to be beneficial [62]. Additionally, since vitamin D levels are often low in PAH patients, vitamin D supplementation may also be helpful to PAH patients. It has been suggested that vitamin D replacement can improve right ventricular size and exercise tolerance [63]. As constant supportive care and lifestyle modification are considered crucial in other chronic diseases such as heart failure or hypertension, such efforts may be necessary for favorable outcomes and quality of life for Korean patients with PAH.
EARLY DETECTION LEADS TO BETTER OUTCOMES
It has been demonstrated that the initial diagnosis of PAH is often delayed, as the percentage of patients with NYHA class III/IV is up to 70% [12,13]. The mean duration between symptom onset and initial diagnosis is 2 to 4 years according to registry data [12,15,64]. Interestingly, the French PAH registry showed that in patients initially diagnosed with PAH without screening, the percentage of NYHA class III/IV was much higher (75%), as compared to their screened counterparts (44%) [12]. Epidemiological and clinical trial data have revealed that delay of diagnosis may be one of the major causes of decreased survival [65-67]. Consistent with such findings, Korean data show that patients with less severe symptoms (NYHA class I/II) have better long-term survival [18]. Accordingly, it is crucial to detect PAH as early as possible through proactive screening. Screening tools for early detection, such as echocardiography, N-terminal pro-brain natriuretic peptide (NT-proBNP) detection, or pulmonary function tests may be useful in patients with predisposing factors for PAH [68]. In particular, RHC should be evaluated for high NT-proBNP levels, FVC/DLCO ratio > 1.6, or abnormal echocardiographic findings in patients with systemic sclerosis [68]. Patients with human immunodeficiency virus infection, a family history of PAH, portal hypertension, or CHD should also be proactively screened through routine echocardiography [68].
INDIVIDUALIZED THERAPEUTIC STRATEGIES THROUGH DEEP PHENOTYPING
PAH registries from Europe, North America, and Asia have provided a better understanding of the prevalence of each PAH subtype and its prognosis [9,69-72], and a high degree of phenotypic variability between IPAH and HPAH has been increasingly recognized. This phenotypic diversity has brought into question the current uniform PAH treatment strategies, regardless of individual patient characteristics, which may bring about variable treatment responses among patients [73,74]. Accordingly, it is necessary to develop better methods for predicting outcomes from the current classes of PAH medications. Deep phenotyping allows the acquisition of large amounts of data from gene sequencing, protein identification, and metabolic profiling [75]. For example, through gene sequencing, single nucleotide polymorphisms or mutations can be identified that are cornerstones in delineating phenotypic variability [29,76,77]. Pioneering efforts are currently being made worldwide to consolidate our understanding of phenotypic variability. The new generation of PAH registries such as the National Biological Sample and Data Repository for PAH [78] and the Biomedical Research Identification of Genetic Etiology of PAH (BRIDGE-PAH) [79] are actively recruiting patients in the United States and United Kingdom, respectively, and are focusing on describing deep phenotypes. These trends create an urgent need for an East Asian population-based PAH registry that incorporates deep phenotyping, including robust genetic, epigenetic, and multi-genomic level data from PAH patients. The PAH Platform for Deep Phenotyping in Korean Subjects (PHOENIKS) is aimed at building a database based on clinical data and biospecimens for PAH patients across South Korea (NCT03933579, Clinicaltrials.gov) [80].
CONCLUSIONS
PAH has become a treatable disease over the last decade in Korea due to the introduction of targeted therapies. As current registry and observational studies within Korea show, proactive screening and early detection together with early aggressive combination therapy is warranted to improve survival for PAH patients.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





