


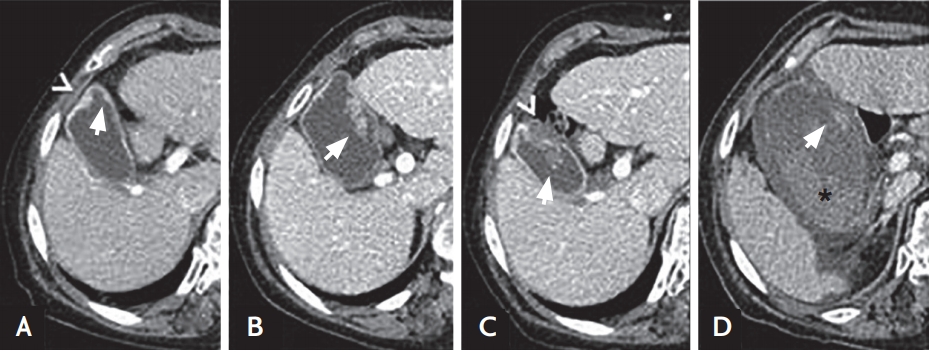
A 78-year-old woman who had been diagnosed with a gallbladder polyp presented to the emergency department with epigastric pain and dizziness. Nineteen months prior to presentation, a 5 mm-sized enhancing polyp of the gallbladder was first detected on an abdominal computed tomography (CT) scan (Fig. 1A). Seven months prior, the polyp had grown to 2.5 cm (Fig. 1B). One month prior, the polyp had grown to 3.5 cm, and focal low-density nodular lesions with pericholecystic infiltration were newly detected (Fig. 1C). At the initial diagnosis, the patient had refused a cholecystectomy. On presentation, physical examination revealed conjunctival pallor and epigastric tenderness. The patient denied any history of hematochezia or hematemesis. A complete blood count revealed anemia (hemoglobin level, 7.8 g/dL). The patient’s blood chemistries including liver function test were normal. CT of the abdomen disclosed an extremely distended and edematous gallbladder with a large hematoma in the lumen (Fig. 1D). Ultrasound-guided percutaneous gallbladder drainage was first performed, followed by laparoscopic cholecystectomy.
The gallbladder showed polypoid masses underlying the hemorrhagic mass, measuring 4 × 3 × 2 cm (Fig. 2A). The tumor was located 3 cm away from the resection margin. Pathologically, an intracystic papillary neoplasm (ICPN) with focal adenocarcinoma (3.5 × 2.0 × 0.9 cm) (Fig. 2B and 2C) and angiosarcoma (2.0 × 2.0 × 0.3 cm) (Fig. 2D) was diagnosed. The ICPN and angiosarcoma were immunopositive for cytokeratin and CD31, respectively (Fig. 2E and 2F). Three months after surgery, the patient is doing well without evidence of recurrence.
Although ICPN is associated with invasive cancer, the prognosis is better than that of other gallbladder cancers. However, the prognosis of gallbladder angiosarcoma is poor, and the clinical presentation can be mistaken for that of acute cholecystitis. Precise early diagnosis using imaging techniques and pathological examination is important. To our knowledge, this is the only case of collision tumor with adenocarcinoma arising in ICPN and angiosarcoma in the gallbladder.
Written informed consents were obtained.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





