


INTRODUCTION
Patients with cirrhosis are in a state of immune dysfunction and bacterial translocation; hence, bacterial infection is common, causing a poor prognosis, and is a major cause of mortality in such patients [1]. The outcome of patients with cirrhosis and septic shock has improved over time, but in-hospital mortality is still reported to be approximately 70% in 2010 [2].
The hospital mortality rate for sepsis and septic shock is approximately 30%, and this varies significantly among different geographic regions of the world [3]. Early detection of sepsis is important in order to improve the chances of survival. Sepsis screening is associated with earlier treatment, and lack of timely recognition delays therapy [4]. The Surviving Sepsis Campaign was established in 2002 to assess the public and clinicians’ awareness of sepsis and develop evidence-based guidelines for the management of sepsis and septic shock [5].
The European Society of Intensive Care Medicine and the Society of Critical Care Medicine's Third International Consensus task force assembled to re-examine sepsis definitions. Sepsis-3 was defined as life-threatening organ dysfunction provoked by a dysregulated host response to infection [6]. The quick Sepsis-related Organ Failure Assessment (qSOFA) is a recently developed risk stratification tool, which has been presented along with a new sepsis definition, to classify infected patients outside of the intensive care unit (ICU). qSOFA was based on incorporating altered mentation, systolic blood pressure of ≤ 100 mmHg, and respiratory rate of ≥ 22/minutes [7]. Questions have been raised whether qSOFA is appropriate for predicting sepsis outside of the ICU although qSOFA is composed of simple parameters [8,9].
It is difficult to predict sepsis in patients with cirrhosis because cirrhosis itself can lead to clinical presentation of sepsis including low systemic vascular resistance, systemic hypotension, and increased heart rate. Thus, a new tool is needed for early detection of sepsis in patients with cirrhosis [10]. In addition, published data are scant on predicting factors of sepsis in liver cirrhosis. We evaluated the clinical usefulness of qSOFA for predicting adverse outcomes in sepsis patients with liver cirrhosis.
METHODS
Study design and study subjects
We conducted a retrospective cohort study to analyze the usefulness of qSOFA for predicting adverse outcomes in sepsis patients with liver cirrhosis at an academic tertiary care hospital with approximately 2,700 beds (Asan Medical Center, Seoul, Korea). Clinical data were collected and analyzed for sepsis patients with liver cirrhosis who triggered activation of the medical emergency team (MET) in general wards between March 1, 2008, and December 30, 2015. We excluded patients aged < 18 years and those with a confirmed do-not-resuscitate (DNR) order at MET activation.
The MET was implemented in 2008 and operates for 24 hours, 7 days a week. The team is activated by a medical doctor or nurse using an electronic medical recording-based monitoring system if a patient's condition deteriorates. The calling criteria for MET intervention include crisis components based on physiological parameters: threatened airway, respiratory rate >30 breaths/min or < 6 breaths/min, oxygen saturation < 90% on venturi mask 40% or O2 12 L/min, pulse rate < 40 beats/min or > 140 beats/min, systolic blood pressure < 90 mmHg, sudden mental change.
The experimental plan and waiving of informed consent for the present study received approval from our Institutional Review Board (IRB No: 2017-0430) and was conducted in accordance with the Korea Food and Drug Administration and the International Conference on Harmonization Good Clinical Practice guidelines.
Data collection and definitions
We extracted the following data on patients with sepsis triggering MET activation from the MET registry and electronic medical records and recorded characteristics such as age, sex, and comorbidities.
Several scores were collected to evaluate the clinical usefulness of qSOFA for predicting adverse outcomes in sepsis patients with liver cirrhosis [11-14]. There are scoring system tools that can predict adverse outcomes in patients with sepsis: systemic inflammatory response syndrome (SIRS), which was included in the previous definition of sepsis; qSOFA, which was a new tool in the 2016 definition of sepsis; sequential (sepsis-related) organ failure assessment (SOFA), and modified early warning score (MEWS), which predicts deterioration of the patient (Table 1).
The qSOFA incorporated altered mentation, systolic blood pressure ≤ 100 mmHg, and respiratory rate ≥ 22/minutes [11]. The SIRS comprises four criteria: body temperature > 38°C or < 36°C, heart rate > 90 minutes, hyperventilation indicated by a respiratory rate of > 20 minutes or PaCO2 of < 32 mmHg, and white blood cell count of > 12,000 cells/μL or < 4,000 cells/μL [12]. The MEWS consists of a simple algorithm based on physiological parameters such as heart rate, systolic blood pressure, respiratory rate, temperature, and mental state [13]. SOFA is a weighted organ dysfunction score comprised of PaO2/FiO2 ratio, Glasgow Coma Scale score, mean arterial pressure, serum creatinine, bilirubin, and platelet count [14]. Each score was calculated according to the data at MET activation.
Illness severity was assessed by the Acute Physiology and Chronic Health Evaluation II (APACHE II) score and Child-Turcotte-Pugh (CTP) class measured within 6 hours after MET activation. The Model for End-Stage Liver Disease (MELD) score was calculated to examine compensated and decompensated liver cirrhosis [15]. We classified compensated liver cirrhosis as MELD < 15 and decompensated liver cirrhosis as MELD ≥ 15. MELD score was calculated based on the data at MET activation.
The primary outcome of the study was to evaluate the prediction ability of qSOFA, SIRS, MEWS, and SOFA for ICU transfer, 28-day mortality, and in-hospital mortality in sepsis patients with liver cirrhosis. A secondary outcome was to compare ICU transfer and hospital mortality rates according to qSOFA scores.
Statistical analysis
Statistical analysis of the collected data was performed using IBM SPSS Statistics software, version 21 (IBM Co., Armonk, NY, USA).
Data are presented as median and interquartile range (IQR) for continuous variables, including age, APACHE II score, and laboratory data, and as number (%) for categorical variables, including sex, type of sepsis, and source of infection. Statistical analysis was performed using the Mann-Whitney U test for continuous variables and the chi-square or Fisher exact test for categorical variables as appropriate. The areas under the curve (AUC) for the ICU transfer and hospital mortality prediction models of qSOFA, SIRS, MEWS, and SOFA were calculated on the receiver operating characteristic curve.
All tests of significance were 2-tailed, and p values < 0.05 were considered significant.
RESULTS
Fig. 1 shows the flow diagram for the study. During the study period, the MET was activated for 2,145 sepsis patients. Overall, 46 of 234 liver cirrhosis patients with a DNR order at MET activation were excluded from analysis. Among the 188 included patients, qSOFA score was 0 or 1 point in 69 (36.7%, group 1) and ≥ 2 points in 119 (63.3%, group 2).
CTP class C was higher (6.3% vs. 69.2%, p < 0.001) in decompensated liver cirrhosis but etiology of liver disease and reason for admission were not significantly different between compensated and decompensated liver cirrhosis. SOFA score was higher in decompensated liver cirrhosis (5.0 [IQR, 4.0 to 6.8] vs. 8.0 [IQR, 6.0 to 10.0], p < 0.001), but qSOFA, SIRS, and MEWS were not different between compensated and decompensated liver cirrhosis (2.0 [IQR, 1.0 to 2.0] vs. 2.0 [IQR, 1.0 to 2.0], p = 0.494; 3.0 [IQR, 1.3 to 4.0] vs. 2.0 [IQR, 1.3 to 3.0], p = 0.066; and 5.5 [IQR, 4.0 to 7.0] vs. 5.0 [IQR, 3.0 to 6.0], p = 0.103, respectively) (Table 2).
Initial management of shock within 6 hours was not different between compensated and decompensated liver cirrhosis. A total of 87 patients (46.3%) were transferred to the ICU, but the rate of ICU transfer was not different between compensated and decompensated liver cirrhosis (34.4% vs. 48.7%, p = 0.138). Overall 28-day mortality rate (28.7%) was significantly higher in decompensated compared to compensated liver cirrhosis (12.5% vs. 32.1%, p = 0.026) as was in-hospital mortality rate (18.8% vs. 41.7%, p = 0.0.15) (Table 3).
Median age of our patients was 59 years (IQR, 52 to 66). APACHE II score was higher (15 [IQR, 10 to 20] vs. 18 [IQR, 12 to 25], p = 0.010) and septic shock was more frequent (39.1% vs. 61.3%, p = 0.003) in group 2. Type of activation, source of new infection, and laboratory findings were not significantly different between the two groups. SIRS criteria and MEWS were higher in group 2 (2.0 [IQR, 1.0 to 3.0] vs. 3.0 [IQR, 2.0 to 3.0], p < 0.001; and 4.0 [IQR, 3.0 to 5.0] vs. 5.0 [IQR, 4.0 to 7.0], p < 0.001, respectively), but SOFA score was not different between the two groups (7.0 [IQR, 5.0 to 9.0] vs. 8.0 [IQR, 6.0 to 10.0], p = 0.091) (Table 4).
Initial management of shock within 6 h differed in the two study groups. Group 2 patients more frequently required vasopressors (49.3% vs. 74.8%, p < 0.001) and mechanical ventilation (10.1% vs. 21.8%, p = 0.042). A total of 87 patients (46.3%) were transferred to the ICU, but the rate of ICU transfer was not different between the two groups (37.7% vs. 51.3%, p = 0.072). Overall 28-day mortality rate (28.7%) was significantly higher in group 2 than in group 1 (15.9% vs. 36.1%, p = 0.003) as was in-hospital mortality rate (26.1% vs. 44.5%, p = 0.012) (Table 5).
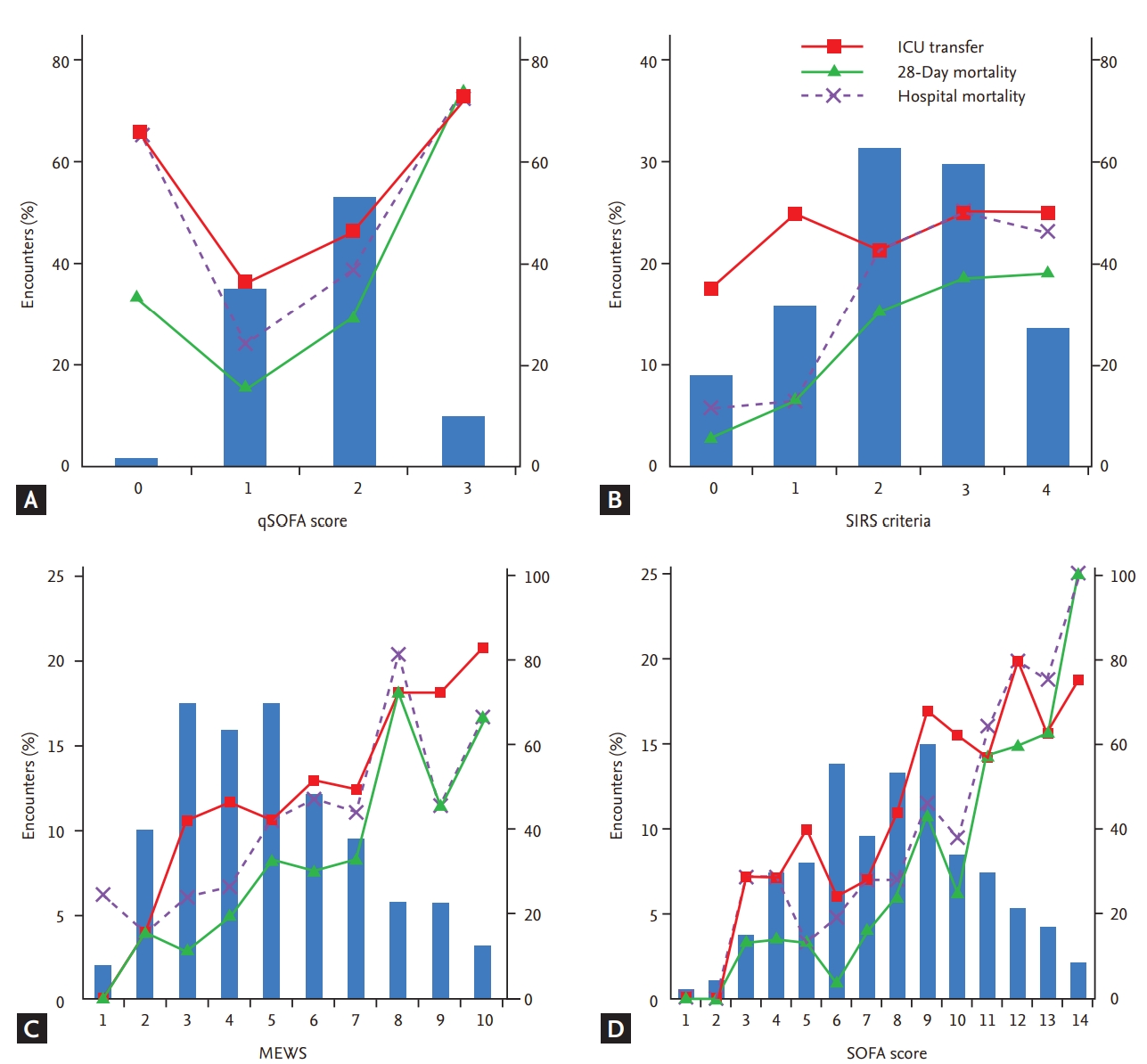
Fig. 2 presents the distribution of qSOFA, SIRS, MEWS, and SOFA score. Increased scores were associated with increased ICU transfer and mortality rates in the MEWS and SOFA scores. The 28-day mortality rate was 33.5% (SIRS), 32.0% (SOFA), and 36.1% (qSOFA) for each group.
The areas under the receiver operating characteristic curve (AUROC) for ICU transfer of SOFA (AUROC, 0.691; 95% confidence interval [CI], 0.615 to 0.767), 28-day mortality (0.757; 95% CI, 0.678 to 0.835), and in-hospital mortality (AUROC, 0.722; 95% CI, 0.644 to 0.799) or MEWS (AUROC, 0.663; 95% CI, 0.586 to 0.739; AUROC, 0.699; 95% CI, 0.617 to 0.782; and AUROC, 0.674; 95% CI, 0.595 to 0.753, respectively) were significantly higher compared to those for qSOFA (AUROC, 0.589; 95% CI, 0.507 to 0.671; AUROC, 0.671; 95% CI, 0.582 to 0.759; and AUROC, 0.626; 95% CI, 0.542 to 0.710, respectively) or SIRS (AUROC, 0.533; 95% CI, 0.451 to 0.616; AUROC, 0.638; 95% CI, 0.556 to 0.721; and AUROC, 0.649; 95% CI, 0.571 to 0.727, respectively) (Fig. 3).
DISCUSSION
Our study attempted to determine the clinical usefulness of the qSOFA score for predicting adverse outcomes in sepsis patients with liver cirrhosis. The results revealed that qSOFA score had limited value in such patients. In total, 36.7% of patients with sepsis and liver cirrhosis could not be detected with ≥ 2 points of qSOFA score. In our study, qSOFA score had more prognostic accuracy for ICU transfer and hospital mortality compared to SIRS but a lower prognostic accuracy compared to MEWS or SOFA scores. A new screening tool is needed for use in these patients. Importantly, our study confirms the clinical usefulness of qSOFA as a risk classification tool for predicting adverse outcomes in sepsis patients with liver cirrhosis.
Choosing an appropriate screening tool is important because early recognition of sepsis is associated with earlier treatment. Potentially preventable secondary infections are associated with a significantly high mortality rate independent of liver disease severity and were predictors of mortality in a multicenter cirrhosis cohort [16]. The model for mortality included secondary infection (odds ratio, 4.42) as a significant variable. Therefore, selecting the most appropriate tools for sepsis screening in patients with liver cirrhosis is necessary. The most important index for diagnosing sepsis was SIRS criteria and infection [17]. Hyperdynamic circulation, hepatic encephalopathy (HEP), tense ascites, and hypersplenism in cirrhotic patients may change heart and respiratory rate, temperature, and white blood cell count despite the absence of bacterial infection [10]. SIRS has been described in 10% to 30% of patients with cirrhosis without bacterial infection [18]. Thus, the lack of sensitivity and specificity of conventional parameters for the definition of SIRS makes a sepsis diagnosis difficult in these patients. In this study, SIRS demonstrated the lowest predictive power for ICU transfer and hospital mortality in sepsis patients with liver cirrhosis, which supports previous research that SIRS is not a useful screening criterion for sepsis in patients with liver cirrhosis and does not help predict clinical deterioration.
Unlike previous results, our main finding indicated that qSOFA score was a poor screening tool. The diagnosis of sepsis recently was revised for the third time, and diagnostic criteria based on qSOFA and SOFA have been suggested. Seymour et al. [7] reported that qSOFA score results are much simpler and faster compared to other screening tools for infected patients outside of the ICU and reported the predictive validity of qSOFA as a good predictor of in-hospital mortality (AUROC, 0.81). Studies to determine the usefulness of qSOFA since the introduction of the new definition (Sepsis-3) are currently in progress. A previous study showed that mortality analyses performed during the hospital stay and at 1 year after discharge supported the use of SOFA and qSOFA as screening tools and demonstrated that these criteria can identify infected patients at high risk for poor outcomes [19]. The most interesting findings of the present study were that 36.7% of patients had a qSOFA score of 0 to 1, of whom 37.7% were high-risk patients requiring ICU care, and the hospital mortality rate in these patients was 26.1%. Furthermore, qSOFA had lower discrimination for hospital mortality; however, this result has not been described previously to our knowledge. In patients with liver cirrhosis, the clinical exacerbation course may cause mental changes, such as HEP, and breathing and consciousness are likely to change accompanied by decreased lung capacity due to increased ascites [20]. Indeed, bacterial infection is a common cause of acute decompensated cirrhosis, and patients with liver cirrhosis and acute organ failure are at high risk for early death. Therefore, qSOFA score may be under- or overestimated depending on the clinical changes in patients with liver cirrhosis [10]. A large number of patients have a qSOFA score of ≤ 1 but there is a risk of ICU care or death. Screening for sepsis based on a qSOFA score of ≥ 2 may delay diagnosis in deteriorating patients. Raith et al. [11] demonstrated that, among adults with suspected infection admitted to the ICU, an increase in SOFA score of ≥ 2 points had greater prognostic accuracy for hospital mortality (AUROC, 0.753) compared to SIRS criteria or qSOFA. They showed that SIRS and qSOFA may have limited use in predicting mortality.
In our study, SOFA score was the most accurate of the evaluated scores for predicting ICU transfer and hospital mortality, followed by MEWS. In a large population of nonintubated sepsis patients, Innocenti et al. [21] demonstrated that SOFA score was significantly higher in patients with an adverse outcome in terms of 28-day mortality and ICU transfer compared to those with a good outcome. Since the SOFA score should be reported in the laboratory results for calculation, which is complicated, it may be difficult to confirm immediately after admission or when the patient's condition changes. In addition, in the Sepsis-3 definition, SOFA was reported to be useful in diagnosing sepsis in the ICU setting. Conversely, MEWS is measured easily but is based only on clinical conditions such as vital signs and consciousness and might be more useful for risk stratification of sepsis patients in general wards.
Our study was performed in acutely deteriorated patients who were referred to MET despite being in general wards (APACHE II score, 17 [IQR, 12 to 22]). The difference in severity was evident when comparing with previous studies. SOFA score was 1 (0 to 2) and 6 (3 to 9) points outside and inside of the ICU, respectively, and the existing study. The qSOFA score had statistically worse predictive validity in the ICU [7]. In our study subjects, the SOFA score was 8 (6 to 10) points, suggesting that acutely deteriorated patients referred to MET require the same level of stratification as that of ICU patients. Therefore, measuring MEWS or SOFA rather than qSOFA would be useful for assessing and predicting patient prognosis, since those referred to MET are typically high-risk patients in general wards.
We analyzed our study patients using the MELD score. There were no differences in qSOFA, SIRS, and MEWS score between compensated and decompensated liver cirrhosis by MELD score. In addition, mortality was different but detecting and managing sepsis was not.
Our study has several limitations. First, it was a retrospective single-center study, thus the findings may not be generalizable to other settings. However, we assembled a large sample size of sepsis patients with liver cirrhosis and used several different screening tools to compare their prediction ability for ICU transfer, 28-day mortality, and in-hospital mortality. Second, the severity was higher in our study objectives because the patients were referred to MET, and patients with liver cirrhosis also had higher severity. Further study is needed to clarify the clinical usefulness of qSOFA in mild sepsis patients with liver cirrhosis in general wards.
In conclusion, among sepsis patients with liver cirrhosis, 36.7% could not be detected with ≥ 2 points of qSOFA score, suggesting that qSOFA score may have limited utility in predicting adverse outcomes in sepsis patients with liver cirrhosis at MET activation. Either MEWS or another screening tool is required for detecting early sepsis in these patients.
KEY MESSAGE
1. This study evaluated the clinical usefulness of quick Sepsis-related Organ Failure Assessment (qSOFA), Systemic Inflammatory Response Syndrome (SIRS), Modified Early Warning Score (MEWS), SOFA scores on predicting factors of sepsis in liver cirrhosis. In our study, qSOFA score and SIRS had a lower prognostic accuracy than MEWS or SOFA scores.
2. Rather than qSOFA, a new screening tool is needed to predict adverse outcomes in sepsis patients with liver cirrhosis.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





