


INTRODUCTION
Heart failure with preserved ejection fraction (HFpEF) is the most common form of heart failure (HF) in the elderly, which accounts for about 50% of HF [1]. With the aging of the population and the increasing burden of comorbidities, the prevalence of HFpEF is steadily increasing [2], whereas its prognosis is not improving. The mortality and acute decompensation rate of HFpEF are similar to that of heart failure with reduced ejection fraction (HFrEF) [3]. Moreover, the rehospitalization rate of HFpEF is as high as that of HFrEF [3,4]. Additionally, patients with HFpEF have a similar or poorer quality of life (QOL) than that of patients with HFrEF [5]. Despite the health and economic importance of HFpEF, optimal medical therapy remains unclear. The medical management of HFpEF is challenging because of the diverse phenotypes of HFpEF [5] and there are few therapies that are proven to be effective for HFpEF, regarding the improvement of mortality or HF hospitalization [6]. Here, we summarize the clinical management of HFpEF and review recent clinical trials, and then provide a therapeutic clue for HFpEF.
DIAGNOSIS OF HFpEF
HF is a clinical syndrome that results from a structural or functional impairment of contraction or filling of the heart [7]. Currently, the diagnostic process of HFpEF includes typical symptoms and signs of HF and natriuretic peptides, after that, it is categorized by left ventricular ejection fraction (LVEF) [7-9]. The cut-off LVEF for HFpEF varies between 40%, 45%, and 50% in clinical trials. In current guidelines [7-9], HFpEF is diagnosed when the patient presents with evidence of increased vascular volume (i.e., elevated natriuretic peptides) or myocardial abnormality to implicate the symptoms and signs of HF with LVEF ≥ 50%. The diagnostic criteria of the current guidelines are summarized in Table 1.
However, the diagnosis of HFpEF remains challenging. The gold standard test for confirming HFpEF is a demonstration of elevated left ventricular filling pressure (LVFP): elevated pulmonary capillary wedge pressure (PCWP) at rest ≥ 15 mmHg or during exercise ≥ 25 mmHg by right catheterization. Although the current guidelines recommend right catheterization in patients with an intermediate pretest probability of HFpEF, the performance of right catheterization is limited in routine clinical practice due to complex technique, cost, and invasiveness. Uncertainty exists in the diagnostic criteria of HFpEF in the current guidelines. The diagnosis of HFpEF depends on the level of natriuretic peptides and echocardiographic data, but the sensitivities of both are quite low [10-12]. In particular, natriuretic peptides might have limited value in evaluating HFpEF [11]. A considerable portion of HFpEF patients with clinical, echocardiographic, and hemodynamic evidence of HF had a normal range of natriuretic peptides [13]. Furthermore, as HFpEF is regarded to have several distinct phenotypes with different pathophysiology, uniform diagnostic criteria of current guidelines could be a major limitation in providing proper treatment of HFpEF.
Therefore, new diagnostic algorithms for HFpEF have been published [14,15]. Reddy et al. [14] reported an H2FPEF score based on six variables, which were important comorbidities and etiologies of HFpEF (Table 2) and demonstrated that the H2FPEF score was superior to the current algorithm (increase in area under the curve of 0.169; 95% confidence interval [CI], 0.12 to 0.22l; p < 0.0001). A higher H2FPEF score was significantly related to future cardiovascular (CV) or HF-related events [16,17].
The HF association of the European Society of Cardiology reported a new diagnostic algorithm for HFpEF and the Heart Failure Association (HFA)-PEFF diagnostic algorithm in the past year [15]. This algorithm is composed of four steps. First, in step P as a pre-test assessment: medical history, electrocardiogram, laboratory tests including natriuretic peptides, and echocardiography should be performed to exclude other causes of dyspnea in all patients with symptoms and signs of HF. In the next step (step E), the HFA-PEFF score is calculated for each patient (Table 3). If the HFA-PEFF score is ≥ 5, HFpEF is diagnosed and if the score is ≤ 1, HFpEF could be excluded. If the HFA-PEFF score is 2–4, which is the intermediate probability of HFpEF, a functional test is recommended in the third step (step F1). Exercise stress echocardiography and invasive hemodynamic test during exercise are common functional tests for HFpEF. Lastly, the specific etiologies of HFpEF should be evaluated for advanced targeted therapy of HFpEF (step F2). The validation of HFA-PEFF was evaluated in a small cohort, and it is useful to diagnose HFpEF [18].
The H2FPEF score is relatively simple and easy to apply. Contrarily, the HFA-PEFF score is complex and costly, but it is sophisticated and helps in finding the etiology of HFpEF. Moreover, no study has validated both scores in the same study population that could elucidate which score is more accurate in diagnosing HFpEF. The diagnosis of HFpEF is still challenging, despite the use of new diagnostic algorithms. Nevertheless, the insights from these new scores are changing the diagnostic paradigm of HFpEF, in which comorbidity, etiology, and phenotype of HFpEF are considered and evaluated in the process of diagnosis.
PATHOPHYSIOLOGY AND ETIOLOGY OF HFpEF
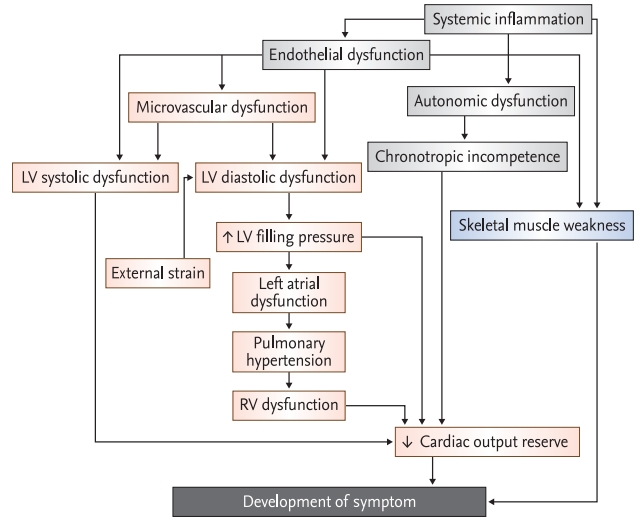
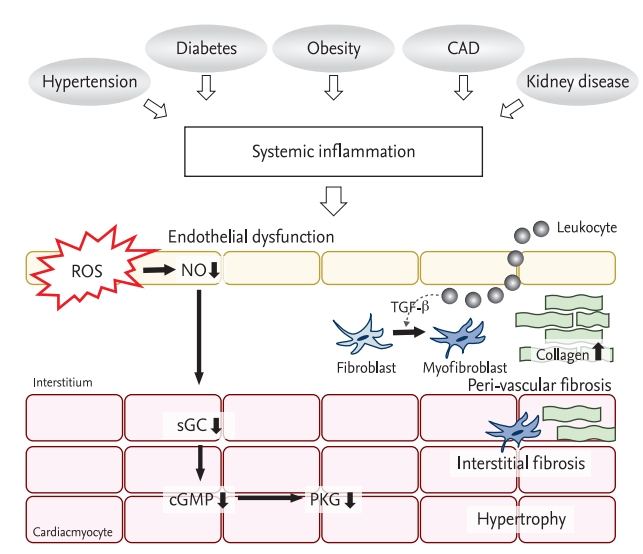
The pathophysiology of HFpEF is intricate and is not yet well understood. Patients with HFpEF are older, predominantly women, and have multiple comorbidities including hypertension, obesity, coronary artery disease (CAD), diabetes, anemia, atrial fibrillation (AF), renal insufficiency, and sleep apnea [13]. These comorbidities affect ventricular and vascular remodeling and are essential for the development of HFpEF (Fig. 1) [19,20]. These comorbidities induce a low-grade systemic inflammation, which induces endothelial dysfunction of systemic and coronary microvasculature [21,22]. The production and bioavailability of nitric oxide (NO) in the endothelium are impaired in HFpEF. Abnormalities in NO-cyclic guanosine monophosphate (cGMP) signaling, including soluble guanylate cyclase (sGC) activity and reduced protein kinase G (PKG) activity in cardiac myocytes, promote myocardial hypertrophy, increased stiffness of the myocardium, and interstitial fibrosis (Fig. 2) [21,23,24]. These result in left ventricular diastolic dysfunction (LVDD) and increased arterial stiffness.
Left ventricular diastolic dysfunction
LVDD is well-known pathophysiology of HFpEF. LVDD is caused by myocardial structural changes, microvascular dysfunction, systematic inflammation, and increased passive chamber stiffness [25]. The increased LVFP, the fundamental and pathologic hemodynamics of HFpEF, predominantly results from LVDD. The passive chamber stiffness is rapidly increased and the prolonged relaxation time is not shortened during exercise and these result in an increase of LVFP in HFpEF [26]. In the earlier stage, LVFP is normal but markedly increases during exercise, while in an advanced stage it increases continuously even at rest [27]. Elevated LVFP leads to elevation of left atrial (LA) pressure (passive LA hypertension) and contributes to an increase in pulmonary capillary hydrostatic pressure and an increase in vascular permeability, resulting in the development of interstitial edema [28]. Increased LVFP is closely related to the development of typical symptoms of HFpEF such as exercise intolerance and exertional dyspnea, symptom severity, and prognosis of HFpEF [29,30].
Left atrial dysfunction
Under the condition of prolonged increased LVFP, secondary structural and functional remodeling of the LA develops. The preservation of LA function might be crucial to the adaptation of HFpEF, which prevents pulmonary congestion and right ventricular (RV) dysfunction [31]. Impaired LA function is related to exacerbation of pulmonary congestion, a change in lung function, and the development and worsening of pulmonary venous hypertension [31-33]. In a recent meta-analysis, it was proven that impaired LA function is valuable for diagnosis as well as for estimating the prognosis of HFpEF [34]. Especially in HFpEF patients with AF, LA structural and functional remodeling is exacerbated, which is a major contributor to disease progression, such as the development of pulmonary hypertension (PH), and RV dysfunction [35].
Pulmonary hypertension and right ventricular dysfunction
The presence of PH in HFpEF patients is associated with poor prognosis [21,36]. PH not only develops from passive LA hypertension but also from increased pulmonary vascular resistance, which is derived from pulmonary vascular disorders such as pulmonary vasoconstriction and pulmonary vascular remodeling [36-38]. A considerable number of HFpEF patients had pulmonary vascular disorders and increased mortality compared to patients with pure passive PH [36]. Regardless of the type of PH, persisting PH eventually induces RV dysfunction. The development of RV dysfunction is associated with a markedly increased risk of mortality [39].
Left ventricular systolic dysfunction
The left ventricular systolic dysfunction evaluated by tissue deformation imaging analysis is present at rest and worsens during exercise in HFpEF [41-43]. Abnormal ventricular-vascular coupling by arterial stiffening is regarded as the cause of subtle left ventricular systolic dysfunction. It results in a significantly impaired proportional increase in stroke volume output in response to exercise, which is one of the major causes of exercise intolerance in HFpEF. The increased left ventricular strain is closely associated with common comorbidities of HFpEF [44], and it has a prognostic value for CV mortality and HF hospitalization in HFpEF [42].
Coronary microvascular dysfunction
A considerable portion of patients presenting with symptoms of ischemia referred for coronary angiography are found to have evidence of ischemia but no significant stenosis of the coronary artery [45]. Most of these patients who have ischemia and no obstructive coronary artery disease (INOCA) have CMD [45]. In epidemiologic studies, INOCA was more prevalent in women and in patients with multiple comorbidities, which are similar to HFpEF [46]. Furthermore, patients with INOCA are likely to have preserved LVEF and a higher incidence of HF hospitalization [47]. Therefore, a link between CMD and HFpEF was strongly suggested [46], and the interaction between LVDD and CMD was clearly associated with an increased risk of HFpEF [48- 50]. CMD has become one of the major phenotypes and pathogenic cause of HFpEF.
Skeletal muscle weakness
Recent studies have identified an important role of the skeletal muscle in HFpEF. In patients with HFpEF, skeletal muscle mass is decreased [51], the composition of skeletal muscle changes with increased fatty infiltration [52] and the capillary density within the muscle is reduced [53]. The oxidative metabolism of skeletal muscle fiber changes to a slow type and a decreased mitochondrial content and abnormal fusion of mitochondria in skeletal muscle are observed [54]. These changes reduce peak O2 uptake and result in exercise intolerance in patients with HFpEF.
TREATMENT
Currently, there are limited data on disease-modifying agents available for HFpEF, which improve clinical outcomes in randomized controlled trials (RCTs). Therefore, treatment guidelines, focused on optimal volume control using diuretics and proper management of risk factors and comorbidities are required. However, with increasing insight in the pathophysiology of HFpEF, various trials in treatment of HFpEF in accordance with the phenotype, have been published. The important trials of HFpEF treatment are described in Table 4.
TRADITIONAL PHARMACOLOGICAL STRATEGIES OF HF: BLOCKADE OF THE ACTIVATED NEUROHORMONAL SYSTEM
Renin-angiotensin-aldosterone system
Inappropriate activation of the renin-angiotensin-aldosterone system (RAAS) occurs in diseases that are associated with the development and progression of HFpEF, in common with HFrEF [55-58]. RAAS promotes the increase of arterial stiffness and myocardial stiffness and causes LVDD and LVH in HFpEF [55]. Therefore, several randomized clinical trials have been conducted to evaluate the prognostic value of RAAS blockade.
The angiotensin-converting enzyme inhibitor or angiotensin receptor blocker was not efficient for CV mortality and HF hospitalization in three large trials (CHARM-preserved [Candesartan in Heart Failure: Assessment of Reduction in Mortality and Morbidity], PEP-CHF [Perindopril in Elderly people with Chronic Heart Failure], and I-PRESERVED [Irbesartan in Heart Failure With Preserved Ejection Fraction]) [59-61]. They did not improve CV mortality, and only candesartan reduced HF hospitalization slightly [59]. A detailed summary of these trials is described in Table 4.
The Treatment of Preserved Cardiac Function Heart Failure With an Aldosterone Antagonist Trial (TOPCAT) is a large RCT to investigate the efficacy of aldosterone antagonists in symptomatic patients with HFpEF (LVEF ≥ 45%) [62]. The differences in the primary endpoint between spironolactone and placebo failed to reach a statistical significance; however, HF hospitalization was modestly decreased by spironolactone. Interestingly, in the subgroup analysis, spironolactone reduced primary outcome in patients with elevated natriuretic peptide levels at enrollment [62] in the Americas (hazard ratio [HR], 0.82; 95% CI, 0.69 to 0.98; p = 0.026) [63]. In Russia and Georgia, patients were enrolled by clinical judgment rather than having increased natriuretic peptides, and were relatively healthy and had lower compliance with study medication than in the Americas [64]. The result obtained in Russia/Georgia would not reflect a true response to spironolactone. For this reason, re-evaluation of the clinical efficacy of spironolactone in HFpEF is necessary. There is currently an ongoing trial in progress: Spironolactone Initiation Registry Randomized Interventional Trial in Heart Failure with Preserved Ejection Fraction (SPIRRIT, NCT 02901184), and their results are expected.
The angiotensin receptor-neprilysin inhibitor (ARNI) sacubitril-valsartan is a combination of inhibitors of neurohormonal activation and up-regulation of the adaptive natriuretic peptide pathway. In a phase-II study, (PARAMOUNT [65]) sacubitril-valsartan induced a greater decrease in N-terminal pro-B type natriuretic peptide (NT-proBNP), a larger reduction in LA size, and a greater improvement of symptoms than valsartan in patients with HFpEF. Therefore, the outcome trial, Efficacy and Safety of LCZ696 Compared to Valsartan, on Morbidity and Mortality in Heart Failure Patients With Preserved Ejection Fraction (PARAGON-HF) trial [66] was conducted in symptomatic HFpEF patients with increased natriuretic peptides. Despite a numerically lower event rate, the efficacy for HF hospitalization and CV death by sacubitril-valsartan approached but did not achieve a statistical significance (HR, 0.87; 95% CI, 0.75 to 1.01; p = 0.06). In post hoc analysis [13], the absolute risk reduction of sacubitril-valsartan was greatest in patients who were recently hospitalized within 1 month (approximately 25% to 30% risk reduction) and it gradually decreased with an increased interval from hospitalization. The sacubitril-valsartan might have alleviated the remaining neurohormonal activation after discharge. These data could provide clues for the initiation or switching time to sacubitril-valsartan in patients with HFpEF. The pre-specified analysis of outcomes by gender in the PARAGON-HF trial reported that the beneficial effect of sacubitril-valsartan was greater in women than in men (rate ratio [RR], 0.73, [95% CI, 0.59 to 0.90] in women vs. RR, 1.03, [95% CI, 0.84 to 1.25] in men, p interaction = 0.017) [67]. The possible reasons were further myocardial remodeling even in the same LVEF, more prominent age-related arterial stiffening in female patients with HFpEF, and differences in the signaling of natriuretic peptide [67]. Recently, Solomon et al. [68] reported the results of a pooled analysis of combined data from the Prospective Comparison of ARNI With ACEI to Determine Impact on Global Mortality and Morbidity in Heart Failure (PARADIGM-HF) [69] and PARAGON-HF [66] trials. The overall treatment benefit was at LVEF ≤ 42.5% and was maximized at lower ejection fraction. The sacubitril-valsartan was valuable in women with LVEF ≤ 60%, contrarily the threshold of LVEF at which efficacy of sacubitril-valsartan was highest was 45% to 50% in men. Therefore, it could be presumed that sacubitril-valsartan is effective for all patients with middle-ranged ejection fraction (HFmrEF). This result was consistent with the clinical characteristics of HFrEF and HFmrEF, which were similar and different from those of HFpEF [70].
There should be a careful application of RAAS blockade to patients with HFpEF because the phenotypes of patients in the real world are different from the inclusion criteria of trials. As the LVEF cutoff of trials varied, a considerable portion of registered patients to these trials might belong to HFmrEF. Neurohormonal activation is less prominent in HFpEF, rather than in HFmrEF or HFrEF. Furthermore, a large proportion of trial patients had already taken RAAS blocker (20% to 86% of the study population) and beta-blocker (55% to 80% of the study population) at enrollment [71], because of their comorbidities including CAD and arrhythmia and their neurohormonal system might be stabilized. Thus, it might leave a little room for the additional benefit from another RAAS inhibitor. Therefore, the messages of clinical trials should be interpreted and accepted judiciously.
Beta-adrenergic signaling
Beta-blockers are the cornerstone of the management of HFrEF [8] because of a significant improvement in mortality and morbidity [72]. Sympathetic activation induces an increment of HR and leads to a shortening of the left ventricular diastolic filling time. Therefore, slowing HR and reversal of sympathetic overactivation could provide a benefit in HFpEF. A lower heart rate at discharge was closely related to a survival benefit in patients with HFpEF [73]. Several observational studies reported a modest benefit of beta-blockers for survival in HFpEF [74-76]. However, in pre-specified sub-analysis of the Study of Effects of Nebivolol Intervention on Outcomes and Rehospitalization in Seniors With Heart Failure (SENIORS) [77] the effect of beta-blockers nebivolol was similar between patients with HFrEF (LVEF ≤ 35%) and patients with HFpEF (LVEF > 35%), although the efficacy of nebivolol to reduce mortality was not statistically significant in both the patient groups. In the Japanese Diastolic Heart Failure Study (J-DHF) [78], an RCT to evaluate the effect of carvedilol in HFpEF (LVEF > 40%), it did not decrease CV death and HF hospitalization. Even in several meta-analyses, the efficacy of beta-blockers for mortality as well as HF hospitalization, in HFpEF is still controversial [79-81]. Recently, a pre-specified TOPCAT trial reported that the use of beta-blockers was related to an increase in HF hospitalization and was not associated with CV mortality in HFpEF [82]. The explained mechanism of ineffectiveness, even harm, was due to an increase in central blood pressure (BP) and myocardial wall stress due to increment of left ventricular volume and pressure by prolonged diastolic filling time [83,84]. However, recently reported Korean registry data showed that the use of beta-blockers reduced all-cause mortality in patients with HFpEF (LVEF ≥ 40%) and acute exacerbation of HF [85]. This benefit existed in patients with global longitudinal strain (GLS) < 14%, but not in patients with GLS ≥ 14% [86]. The conflicting results regarding the efficacy of beta-blockers are still unknown. This is due to the difference in the definition of HFpEF, especially LVEF cut-off value, heart rate at enrollment, and their changes after medication and pre-existing comorbidities, such as AF and CAD [87]. Despite these, beta-blockers might be beneficial to patients with HFpEF, especially in patients with myocardial remodeling with reduced GLS.
DISEASE-MODIFYING PHARMACOLOGICAL STRATEGIES
As mentioned above, the deregulation of the NO-sGCcGMP-PKG pathway is a potentially key mechanism of HFpEF. Therefore, therapeutic approaches have been tried to use medications that act on this pathway, including nitrates, phosphodiesterase-5 inhibitors, and sCG stimulators. Several trials have evaluated the role of these agents in the pathogenesis and treatment of HFpEF, with limited success.
Organic and inorganic nitrates
In altered endothelium-cardiomyocyte signaling by inflammation, NO is absent in cardiomyocytes. Therefore, organic NO supplementation was supposed to be helpful for HFpEF due to the restoration of myocardial NO content as well as alleviation of increased arterial load [5]. In the Nitrate’s Effect on Activity Tolerance in Heart Failure with Preserved Ejection Fraction (NEAT-HFpEF) trial [88], organic nitrate isosorbide mononitrate did not improve QOL and NT-proBNP, even if the daily activity level was reduced and HF symptoms worsened in the isosorbide mononitrate group. The possible causes were excessive hypotension and decreased cardiac output due to preload reduction [89], the rapid development of tolerance, and endothelial dysfunction by organic nitrates [90]. In contrast, inorganic nitrate (NO3) has a different NO metabolism: the nitrate-nitrite pathway. The nitrate-nitrite pathway could be an important route to restore NO in HFpEF, especially in the presence of hypoxia and acidosis such as skeletal muscle during exercise [91]. In small trials, the delivery of inorganic nitration via NO3--rich beetroot juice improved the exercise capacity of HFpEF patients [92,93]. The administration of sodium nitrite via infusion or inhalation improved cardiac output reserve, ventricular filling pressure, and pulmonary artery pressure during exercise in HFpEF. However, Inorganic Nitrite Delivery to Improve Exercise Capacity in HFpEF (INDIE-HFpEF) trial [94] showed that inhaled inorganic nitrite for 4 weeks failed to improve exercise capacity and QOL. The nitrite inhalation with its short-acting nature could be the cause of this result, as other administrations of inorganic nitrite, which provide a persistent and higher level of NO, achieved positive results. It is necessary to confirm the effectiveness of NO3 in larger and long-term trials.
sGC stimulators
The sGC stimulators (riociguat and vericiguat) enhance cGMP production by acting on the NO receptor of sGC and activating sGC to generate cGMP. In Acute Hemodynamic Effects of Riociguat in Patients with Pulmonary Hypertension Associated with Diastolic HF (DILATE-1) [95] and Soluble guanylate Cyclase stimulatoR in heArT failurE patients with PRESERVED EF (SOCRATES-PRESERVED) [96] trials, sGC stimulators showed limited improvement in hemodynamic and echocardiographic parameters.
Sildenafil
Despite the possible positive effect of sildenafil in HFrEF [97], two separate studies for evaluating the efficacy of sildenafil in HFpEF with PH or RV dysfunction failed to show improvement in exercise capacity and QOL, and sildenafil was associated with impairment of renal function and increment of neurohormone level [98,99].
Other PKG-stimulating drugs, sacubitril
PKG is an intrinsic suppressor of ventricular hypertrophy and interstitial fibrosis [5]; therefore, stimulation of PKG is a potential therapy in HFpEF. cGMP is mandatory to stimulate PKG. As mentioned above, cGMP is synthesized by sGC via the NO-sGC-cGMP-PKG pathway and is generated by receptor guanyl cyclase linked to natriuretic peptide receptors. Therefore, the sacubitril, a neprilysin inhibitor, stimulates PKG by elevating the level of natriuretic peptides. The efficacy of ARNI in HFpEF is described above.
NON-PHARMACOLOGICAL THERAPY
Devices targeted to high LVFP
Pressure monitoring
As mentioned above, increased LVFP is a hallmark of the pathophysiology of HFpEF. PCWP is a hemodynamic parameter that reflects LA pressure and LVFP. A therapeutic strategy of hemodynamic monitoring accompanied by early therapeutic intervention might improve the clinical outcome of HFpEF patients. The CardioMEMS Heart Sensor Allows Monitoring of Pressure to Improve Outcomes in NYHA Class III Heart Failure Patients (CHAMPION) trial demonstrated that active reduction of LVFP guided by an assessment of central hemodynamics in HF patients regardless of LVEF significantly decreased HF hospitalization [100]. This finding persisted in additional analysis in HFpEF patients (LVEF ≥ 50%) [101] and real-word data [102].
Interatrial septal shunt
The other device targeted to high LVFP is an interatrial septal shunt to reduce LA pressure. In the Reduce Elevated Left Atrial Pressure in Patients with Heart Failure (REDUCE LAP-HF) study, an interatrial shunt was efficient in decreasing LAP and improving functional capacity [103] and these efficacies were confirmed in a long-term study with the improvement of hemodynamic data during exercise without significant complication [104,105]. The interatrial shunt might be helpful in the management of HFpEF, especially high LA filling pressure due to LA dysfunction, even though further studies to evaluate the long-term improvement are required.
Pacing
Chronotropic incompetence contributes to impaired cardiac output reserve, as described above. The restored normal heart rate response during exercise by pacemaker might be beneficial to HFpEF with chronotropic incompetence. The Rate-Adaptive Atrial Pacing In Diastolic Heart Failure (RAPID-HF) trial is ongoing to evaluate the impact of rate-adaptive atrial pacing on exercise capacity (NCT 02145351).
PREVENTIVE STRATEGIES FOR HFPEF: MANAGEMENT OF COMORBIDITIES
Hypertension
Hypertension is the most common comorbidity of HFpEF patients. In many previous RCTs of antihypertensive medication, optimal treatment of hypertension reduced the incidence of HF [106]. In HFpEF, the additional benefit of lowering BP is uncertain. As mentioned above, there was discordance between BP lowering and clinical outcome in large trials with neurohormonal inhibitors in HFpEF, even though neurohormonal inhibition had a favorable effect on ventricular hypertrophy, interstitial fibrosis, and myocardial stiffness [5]. Nevertheless, a recent meta-analysis showed that BP lowering was closely related to the reduction in HF hospitalization rather than all-cause mortality in HFpEF patients [107]. Furthermore, optimal BP control is important to prevent other major CV outcomes, including stroke and CAD, even in HFpEF patients.
Sodium-glucose cotransporter-2 inhibitors
The diabetes is prevalent in 20% to 40% of HFpEF patients [21]. Three RCTs on sodium-glucose cotransporter-2 (SGLT2) inhibitors in type 2 diabetes with high CV risk or established CV disease demonstrated a valuable effect of SGLT2 inhibitors [108]. McMurray et al. [109] reported that dapagliflozin significantly reduced worsening HF or CV death in HFrEF patients. The benefit of dapagliflozin on HF was similar between the patients with and without diabetes. The potential mechanism of the beneficial effect of SGLT2 inhibitors is not only to decrease intravascular volume via osmotic diuresis and natriuresis but also to reduce neurohormonal activation [110]. SGLT2 inhibitors increase metabolic efficiency and myocardial energy supply [110]. Furthermore, SGLT2 inhibitors induce a decrease in oxidative stress and fibrosis, an increase of endothelial function, and vascular compliance, which may be favorable in HFpEF [110,111]. The diastolic parameter was improved by the administration of SGLT2 inhibitors in patients with type 2 diabetes patients [112,113]. The RCTs for the efficacy of SGLT2 inhibitor in HFpEF (EMPagliflozin outcomE tRial in Patients With chrOnic heaRt Failure With Preserved Ejection Fraction [EMPEROR-Preserved; NCT 03057951], Effect of EMpaglifozin on ExeRcise ability and heart failure symptoms, In patients with chronic heArt faiLure with preserved ejection fraction [EMPERIAL-preserved; NCT 03448406], Dapagliflozin Evaluation to Improve the LIVEs of Patients With PReserved Ejection Fraction Heart Failure [DELIVER; NCT 03619213], dapagliflozin in PRESERVED Ejection Fraction Heart Failure [PRESERVED-HF; NCT 03030235]) are ongoing and we look forward to the results of these studies shortly.
Lifestyle modification
Lifestyle modifications, including exercise, weight reduction, and dietary composition, are beneficial in preventing and treating HF [114]. However, the potential benefit of lifestyle modification has not been fully elucidated in RCT or cohort studies. Nevertheless, the efficacy of exercise was reported in several studies that included endurance and resistance training, improved exercise capacity, and QOL in HFpEF [115,116]. About half of HFpEF patients have obesity, and an increase in body adiposity triggers systemic inflammation and impairment of cardiac, vascular, and skeletal muscle function [5]. Kitzman et al. [117] demonstrated that caloric reduction during 20 weeks significantly improved peak O2 consumption, symptoms, and QOL in older and obese patients. The additive benefit was derived by a combination of caloric restriction and exercise. Lifestyle modification might be important for the management of HFpEF as well as a cardiometabolic syndrome, representative comorbidity of HFpEF. Further investigation to prove the beneficial effect of lifestyle modification in HFpEF is required.
CONCLUSIONS
HFpEF is the most common form of HF with an increase in the elderly population, and its prognosis has not yet improved. The trials of medications have been neutral or less effective in terms of their primary outcomes. The possible explanations for this result are incomplete understanding of the pathophysiology, heterogeneity of the study populations, lack of universal diagnostic criteria of HFpEF, unconnected pathophysiological mechanisms related to treatment, and suboptimal designs for statistical power of the trials. Currently, the concept of HFpEF is evolving; HFpEF is a multifaceted syndrome. The pathophysiology of HFpEF is multifactorial, with several mechanisms and comorbidities involved, and different from that of HFrEF. HFpEF results from a complex interaction of heart, vasculature, and peripheries: LVDD, systolic functional reserve, autonomic imbalance, and macro- and microvasculature response to increased oxygen demand. Substantial heterogeneity exists in these interactions and dominance in each patient with HFpEF. Therefore, the definition of HFpEF by LVEF is bound to be limited. Recently, new diagnostic strategies have been proposed that appear promising; however, further validation is required. Treatment of HFpEF needs to be approached differently according to various phenotypes of HFpEF, and several treatment trials are on the way as per different therapeutic approaches (summarized in Table 5). In our daily clinical practice, we need to understand the nature of the diversity of HFpEF and approach each patient with HFpEF individually.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





