Phase II Study to Topotecan and Cisplatin in Advanced Hepatocellular Carcinoma
Article information
Abstract
Background:
Hepatocellular carcinoma remains a highly chemoresistant neoplasm and is a common malignancy with poor prognosis in Korea. We performed a phase II study to evaluate the efficacy and toxicities of topotecan and cisplatin combination chemotherapy for advanced hepatocellular carcinoma.
Methods:
Between November 1999 and May 2001, ten patients with histologically proven hepatocellular carcinoma were enrolled in this study. The median age was 54 (range: 53–74) years and all were male. Six patients demonstrated stage IV, 1 stage IIIC, 2 stage IIIB and 1 stage IIIA. Six patients showed a ECOG performance status of 1. The treatment regimen consisted of topotecan 1.25 mg/m2 and cisplatin 20 mg/m2 for 5 days. The treatment was repeated every 4 weeks. Toxicities were evaluated according to WHO toxicity criteria.
Results:
All ten patients were evaluable for response and toxicity. There was only one patient who achieved partial response. The overall response rate was 10% (95% C.I.) and the response duration was 46 weeks. The median survival of all patients was 21 (range: 17–54+) weeks. During a total of 24 cycles, neutropenia of WHO grade 3 and 4 occurred in 33%, thrombocytopenia in 33% and anemia in 21%. In non-hematologic toxicity, diarrhea and hepatoxicity of grade 3 occurred in 1 and 2 patients, respectively. But there was no treatment-related death.
Conclusion:
When used in this dose and schedule, topotecan and cisplatin combination chemotherapy does not seem to be effective for patients with advanced hepatocellular carcinoma.
INTRODUCTION
Primary liver cancer is the third most common malignant tumor and the second leading cause of death from malignant disease in men in Korea. Hepatocellular carcinoma occupies about two thirds of primary liver cancer1). The drug therapy of unresectable hepatocellular carcinoma is in a desperate situation. A variety of single agents has been tested in phase II trials without documented success. And combinations of drugs have performed no better2). Therefore, studies of new agents, especially drugs with novel mechanisms of action, are needed.
Topotecan [(S)-9-dimethylaminomethyl-10-hydroxycamtothecin hydrochloride] is a semisynthetic analog of camptothecin which is an early topoisomerase I inhibitor and causes unpredictable, severe myelosuppression, gastrointestinal toxicity and hemorrhagic cystitis in clinical trials3). Topotecan was specifically designed to have a more favorable toxicity profile due to better water solubility. Like camptothecin, its mechanism of cytotoxicity involves inhibition of topoisomerase I by stabilizing the cleavable complex formed by the uncoiling enzyme topoisomerase I and DNA. This results in single strand breaks at the replication fork, allowing the intact strand to pass through. Therefore, cells in the S-phase are primarily affected4).
In preclinical studies, topotecan demonstrated a broad spectrum of in vitro and in vivo antitumor activity. Phase I studies with topotecan in a variety of schedules were performed, with neutropenia described as the dose limiting toxicity5, 6). The Southwest Oncology Group undertook a phase II trial of topotecan in hepatocellular carcinoma patients. In this phase II study of topoisomerase I inhibitor topotecan, a response rate of 13.9% was obtained utilizing a five-consecutive-day bolus infusion schedule7). As previously reported with topoisomerase I inhibitors and ciaplatin, a synergic cytotoxicity has been observed in vitro between topotecan and ciaplatin8). Therefore, it can be reasonable to evaluate the effect of a combination of topotecan and cisplatin in patients with heptocellular carcinoma and we initiated a phase II study of topotecan and cisplatin in inoperable hepatocellular carcinoma with the aim of assessing the response to therapy and verifying the toxicity.
MATERIALS AND METHODS
1 Patient selection and evaluation
Ten patients were entered into the study. All patients had to have histologically confirmed hepatocellular carcinoma. To be eligible for the study, a patient had to have 1) an ECOG performance status of 0, 1 or 2, 2) one or more lesions that could be measured from each side, 3) no prior systemic chemotherapy, 4) adequate baseline organ function, defined as a WBC count of at least 4,000/μL, a platelet count of at least 100,000/μL, a total bilirubin level of less than 3.0 mg/dL, serum transaminases levels of less than 3 times the upper limit of normal, and a serum creatinine value of less than 1.5 mg/dL or a creatinine clearance more than 50 mL/min.
However, patients with symptomatic brain metastases or other severe illnesses were excluded from the study. Written informed consent was required from each patient.
A complete history, physical examination, recording of performance status according to ECOG criteria, complete blood cell count with differential, serum biochemistry, alpha-fetoprotein, urinalysis and ECG were obtained at baseline for each patient. Chest radiographs and liver CT scans were routinely performed on all patients. Other radiographic examinations, eg, isotope bone scans, brain CT scan and abdominal ultrasonography were performed if clinically indicated. Pathologic test was performed with fine-needle aspiration biopsy.
2) Treatment
It was planned that each patient would receive chemotherapy every 28 days until evidence of progression but the course of chemotherapy was limited to a maximal six cycles. The treatment regimen consisted of cisplatin 20 mg/m2/day and topotecan 1.25 mg/m2/day intravenously on days 1 through 5, respectively. Cisplatin infusion preceded topotecan infusion by 30 min.
Full doses of chemotherapy were given if WBC and platelet counts were at least 4,000/μL and 100,000/μL on day 0, respectively. In case of WHO grade 1 leukopenia or thrombocytopenia, treatment was given at doses reduced by 25%. In patients with grade 2 or higher leukopenia or thrombocytopenia, treatment was delayed for 1 week. Granulocyte colony-stimulating factor was given if necessary. Prophylactic antiemetics were routinely administered on the day of chemotherapy with 5-HT3 receptor antagonists.
3) Efficacy and toxicity assessment
Physical examinations, complete blood counts and biochemistry profiles were repeated every 4 weeks. Toxicities were graded according to WHO toxicity criteria. Radiographic evaluations for tumor response, including isotopic bone scan and CT scan, were performed every two courses of chemotherapy. Responses were defined as follows: a complete response was the disappearance of all clinical and radiographic signs of tumor for at least 4 weeks; a partial response was a more than 50% reduction in the sum of products of the biperpendicular diameters of all measurable lesions, with no increase in size of any lesion and no new lesions; stable disease was a decrease of less than 50% or an increase of the less than 25% in the product of the longest perpendicular diameters of measurable lesions and no new lesion; and disease progression was a 25% or greater increase in size of any lesion or the appearance of any new lesion.
The response duration was measured from the date of confirmation of the least partial tumor response to the date of disease progression. Survival was measured from the date of the beginning of therapy until the date of death or last follow-up evaluation.
Statistical analysis was performed with SPSS (version 10.0) statistical program for personal computers. Response rates were calculated by ninety-five percent confidence interval. Survival was estimated by the Kaplan-Meier method.
RESULTS
1) Patient Characteristics
From November 1999 to May 2001, a total of 10 patients have been treated by topotecan and cisplatin in our institute. The main characteristics of the patients are summarized in Table 1. All patients were male. Their median age was 54 with a range of 53 to 74 years. The ECOG performance status was 0 or 1 in 6 (60%) patients and 2 in 4 (40%) patients. All patients had been pathologically proven hepatocellular carcinoma. According to UICC/AJCC staging system, one patient had stage IIIA disease, two had IIIB, one had IIIC and six had IV. Previous hepatic resection was performed with curative intent in 2 patients (20%) who relapsed thereafter. Two patients had received transarterial chemopatient embolizations. The others had no previous treatment. One had received involved field radiation therapy due to spinal metastasis. Extrahepatic metastases were observed in six patients. Sites of metastasis included spine (1 patient), intraabdominal lymph nodes (3 patients) and lung (4 patients). Among all patients, the serum alpha-fetoprotein (AFP) was 10–568,700<μg/mL (normal range, <2.5 ng/mL). A total of 24 courses of treatment were given, for a median of two courses per patients (range, 1 to 6 courses).
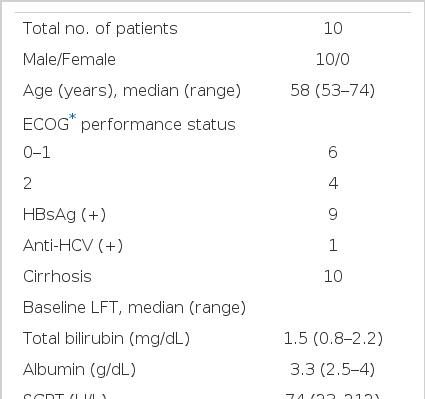
Patient characteristics
2) Response and Survival
All of the patients were evaluable for response and toxicity. After a median two cycles of chemotherapy, there were no complete response and one partial response, for an overall response rate of 10% (95% CI, 0% to 29%). The response duration of responder was 46 weeks. Four patients demonstrated stable disease as their best response to therapy and the other five patients had progressive disease. At the time of this analysis, 9 patients were reported dead. The median progression-free survival was 16 weeks (range, 0 to 47 weeks). The median survival time was 21 (range, 17 to 54+) weeks and 1-year survival rate was 10% (Figure 1).

Time to progression and overall survival curves of total patients.
3) Toxicities
Hematologic and non-hematologic toxicities are listed in Table 2. WHO grade III–IV neutropenia and thrombocytopenia occurred in 33% and 33% of cycles, respectively. WHO grade III anemia occurred in 21% of cycles. Four patients experienced the life-threatening (WHO grade IV) neutropenia or thrombocytopenia. Four episodes of fever with neutropenia were observed but resolved with empiric antibiotics and granulocyte colony-stimulating factor. There were no toxic deaths and life-threatening bleeding.

Toxicities of topotecan and cisplatin chemotherapy
All ten patients were assessable for symptomatic toxicity. There was no grade IV non-hematologic toxicity. Nausea and vomiting were documented in the majority of patients.
Three patients had experienced WHO grade III vomiting. One patient had WHO grade III diarrhea. Stomatitis of WHO grade II occurred in two patients. Alopecia occurred in a half of the patients. Renal toxicity was not developed. WHO grade III hepatotoxicity occurred in two patients who had progression of disease.
DISCUSSION
Hepatocellular carcinoma remains a highly chemoresistant neoplasm. In this study of the topoisomerase I inhibitor topotecan and cisplatin, a response rate of 10% was obtained. There were no complete responses and the median survival was 21 weeks. The Southwest Oncology Group’s study with topotecan alone used at full doses has reported a 13.9% response rate in 38 chemotherapy naive patients, but was associated with life-threatening (grade IV) neutropenia in 69% of patients, including one toxic death7). In an Eastern Cooperative Oncology Group randomized phase II study in patients with hepatocellular carcinoma, the upper 95% confidence interval of response rate of cisplatin was 17%9).
As previously reported with topoisomerase I inhibitors, including topotecan and cisplatin, a significant schedule-dependent synergistic cytotoxicity was found in some of the cell lines used with cisplatin followed by topotecan8). Therefore, we clinically expected more effective results than previous single-agent studies in terms of response rate. But our experience did not verify the possibilities of systemic combination chemotherapy to improve the outcomes. A similar consequence in inoperable hepatocellular cancer patients was observed in a combination of topotecan and oxaliplatin, which is a diamino-cyclo-hexane-platin compound proven effective against several cisplatin-resistant tumor cell lines. Causing only one subjective response among 13 patients in this trial, topotecan and oxaliplatin is unlikely to be active, too10).
Treatment of unresectable hepatocellular carcinoma is extremely disappointing because neither locoregional (chemo-embolization or percutaneous alcohol injection) nor systemic therapies have demonstrated any survival benefit11). Only adriamycin and cisplatin have exhibited response rates up to 15% to 20% after systemic administration. Lee et al., using adriamycin and cisplatin, achieved a 36% response rate in 14 evaluable patients with advanced hepatocellular carcinoma. However, in this phase II study, the median survival time of all patients was 17 weeks, although the median time to progression was statistically significantly better in the responders than in the nonresponders12).
In unresectable hepatocellular carcinoma without severe underlying cirrhosis, concomitant intraarterial chemotherapy and embolization are usually considered the treatment of choice. Reported response rates with intraarterial doxorubicin and cisplatin combination are better than using the intravenous route13). However there is no clear evidence that this strategy could improve survival over best supportive care or intravenous chemotherapy14). The systemic chemotherapy in hepatocellular carcinoma published during the past 20 years are clearly dismal, so the activity of new cytotoxic agents and promising combinations probably have been underexplored. And there is a need for more intensive clinical research in this area. Some studies have recently evaluated the efficacy of new cytotoxic agents in unresectable hepatocellular carcinoma. Interesting results have been observed in chemotherapy-naive patients with paclitaxel15) and gemcitabine16) that need larger studies.
In this study, patients with advanced hepatocellular carcinoma can be treated with topotecan, topoisomerase I inhibitor and cisplatin. While administration of topotecan and cisplatin at this dose and schedule was relatively well tolerated in terms of non-hematologic toxicities, the hematologic toxicity was significant. Six patients experienced grade IV neutropenia or thrombocytopenia, although there were no toxicity related death or life-threatening bleeding. These results are similar with those of the Southwest Oncology Group study using a higher dose of single topotecan7). Nevertheless, although patients with advanced hepatocellular carcinoma can be treated with topotecan and cisplatin, we do not recommend the regimen of this dose and schedule.
CONCLUSION
We hope this study may contribute to the interest in the development of cytotoxic agents and combination regimens in hepatocellular carcinoma. When used in this dose and schedule, a combination chemotherapy of topotecan and cisplatin does not appear to be effective for patients with advanced hepatocellular carcinoma.