Preoperative Evaluation of the Curative Resectability of Gastric Cancer by Abdominal Computed Tomography and Ultrasonography: A Prospective Comparison Study*
Article information
Abstract
Objectives
We compared the ability of preoperative abdominal computed tomography (CT) with that of preoperative abdominal ultrasonography (US) in predicting the extent of tumor growth and the curative resectability of gastric cancer.
Methods
Abdominal CT and US were done in 95 patients with gastric adenocarcinoma. The radiologic findings were prospectively compared with surgical and pathologic findings.
Results
The sensitivities of abdominal CT and US in detecting the perigastric lymph node involvement were 26.6% and 20%, respectively. The sensitivity of abdominal CT in predicting the pancreatic invasion (60%) was better than that of abdominal US (20%). However, there were 6 false positive diagnosis of pancreatic invasion by abdominal CT; in contrast, there was no false positive diagnosis of pancreatic invasion by abdominal US. Of 95 patients who underwent surgical exploration, 14 were found to have unresectable tumors because of extragastric organ involvement and distant metastases. Abdominal CT falsely predicted 8 of 74 cases in which curative gastric resection was impossible as resectable. Moreover, abdominal CT falsely predicted 5 of 81 cases in which curative gastric resection was possible as unresectable. Abdominal US falsely predicted 12 of 14 cases in which curative surgery was impossible as resectable.
Conclusion
Preoperative abdominal CT and US did not accurately predict the tumor extent and the curative resectability of the gastric cancer. Especially, abdominal CT finding of pancreatic invasion by gastric cancer should not be a contraindication for surgical exploration.
INTRODUCTION
The prognosis of a patient with gastric adenocarcinoma depends on his or her clinical stage at presentation. Therefore, accurate determination of the extent of tumor growth is essential for the proper management of patients with gastric cancer1). Abdominal computed tomography (CT)2–10) and ultrasonography (US)11–14) have been used to preoperatively predict the stage of the gastric cancer.
Abdominal CT or US can demonstrate not only the gastric wall and the perigastric tissue, but also the direct extension of tumor into the contiguous organs and the presence of distant metastases15). Some investigators have reported that abdominal CT or US provided equally accurate preoperative staging information of gastric cancer2–6,12–14) and have claimed that it could replace the operative exploration in patients with unresectable tumor.
Although there have been many reports on preoperative evaluation using either abdominal CT or US, reports comparing preoperative abdominal CT or US results with surgical results are variable2–14) and only few have tried to compare the predictive roles of CT and US. Moreover, many of these reports were retrospective studies and used a small number of patients. Therefore, in this study, we prospectively compare the ability of preoperative abdominal CT with that of preoperative abdominal US to predict the extent of tumor growth and the curative resectability of gastric cancer in 95 patients.
PATIENTS AND METHODS
1. Patients
Between August 1990 and July 1991, 295 patients with gastric adenocarcinoma diagnosed using endoscopic biopsy underwent preoperative abdominal CT and/or US. For ethical reasons, patients in this group with definite evidence of distant metastases, such as space occupying lesions in the liver detected by abdominal CT or US, malignant ascites, metastatic cervical lymph nodes confirmed by histology or palpable rectal shelves, were not operated and were excluded from the study. Ninety-five patients were enrolled in the series. Sixty-seven patients were men and twenty-eight were women. The mean age was 52.9 years with a range of 26–78 years.
2. Radiologic study
Both abdominal CT and US were performed on each patient before laparotomy. CT was done with a GE 9800 scanner (General Electric, Milwaukee, IL) using a 1-cm slice thickness and 1-cm interval. Scan was done from the top of the liver to the iliac crest with the patient in supine position to evaluate the gastric mass and the extent of the tumor. Then the scan was repeated from the fundus of the stomach to the lowest level of the pancreas in right lateral decubitus position to evaluate the pancreatic invasion.
US was done with 3.5- or 5-MHz sector scanner (Acuson 128, Mountain view, CA). Transverse and longitudinal scans of epigastric and right upper quadrant area were done with the patient in supine position to evaluate the gastric mass and the extent of the tumor. In case of gaseous distention of the stomach, 500–1000ml of water was given to the patient and scan was done in a sitting position to improve the visualization of the pancreas and retroperitoneal organs.
The results from each procedure were interpreted by the consensus of two radiologists (B.I.C. and J.K.H.) before laparotomy, without knowledge of each other’s results. If there was a disagreement in the interpretation of radiologic findings, the final decision was made after the discussion. The accordance rate was more than 80%. Lymph node enlargement was evaluated, particularly in the perigastric, celiac and para-aortic areas. A lymph node was regarded as being enlarged if the longest diameter of an Individual node exceeded 1 cm. Pancreatic invasion was considered to be present if the fat plane between the stomach and the pancreas was obliterated or if there was a lack of change in relative position of the gastric mass and the pancreas. The mesocolon was considered to be invaded if there is a soft tissue mass or streaky lesions that were connected to the gastric mass. Patients with radiologic findings of para-aortic lymph node enlargement, pancreas and liver invasion, and mesocolon involvement were preoperatively judged to have a disease in which the curative resection was impossible.1,16) However, according to the protocol, all of these patients underwent exploratory laparotomy within 14 days from radiological studies for either palliation or attempt at cure.
The abdominal CT and US results were compared with surgical and pathologic findings. The sensitivities and specificities of abdominal CT and US in detecting lymph node and extragastric organ involvement were evaluated. The positive and negative predictive value of abdominal CT and US in predicting the curative resectability were also calculated.
RESULTS
1. Assessment of Tumor Extent
1) Lymph node involvement (Table 1, 2)

Assessment of Tumor Extent of Gastric Adenocarcinoma by Abdominal CT (n=95)
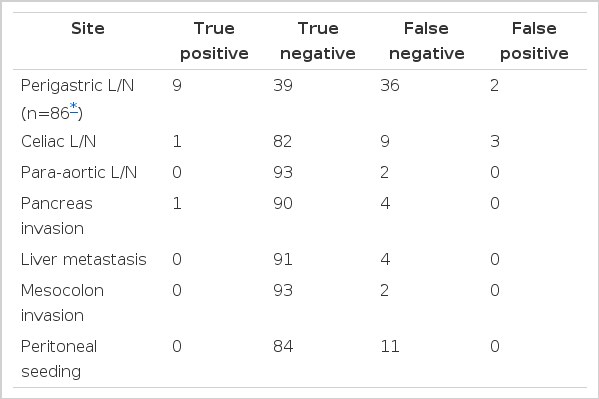
Assessment of Tumor Extent of Gastric Adenocarcinoma by Abdominal US (n=95)
Overall, neither abdominal CT nor US were effective in detecting the lymph node involvement in 86 of 95 cases. In 9 of 95 cases, histological confirmation of perigastric lymph nodes and palliative gastrojejunostomies without lymph node dissection was done. Perigastric lymph node involvement was found in 45 of 86 cases. Abdominal CT and US correctly predicted perigastric lymph node involvement only in 12 and 9 cases, respectively. There were 5 and 2 false positive diagnoses by abdominal CT and US, respectively.
Histological examination of all the celiac and para-aortic lymph nodes was impossible because of difficulties in obtaining specimens during surgery. Therefore, we compared radiologic findings with operative findings in the evaluation of celiac and para-aortic lymph node involvement. There were 10 patients with celiac lymph node enlargement and 2 patients with para-aortic lymph node enlargement at laparotomy. Abdominal CT and US identified celiac lymph node enlargement in only 2 and 1 cases, respectively. There were 3 false positive diagnoses by abdominal US. Abdominal CT correctly identified para-aortic lymph node enlargement in 1 of 2 cases, but abdominal US did not identify para-aortic lymph node enlargement. There was no false positive diagnosis by abdominal CT or US in detecting para-aortic lymph node enlargement.
Sensitivities and specificities of abdominal CT and US in detecting the lymph node involvement are shown in Table 3.
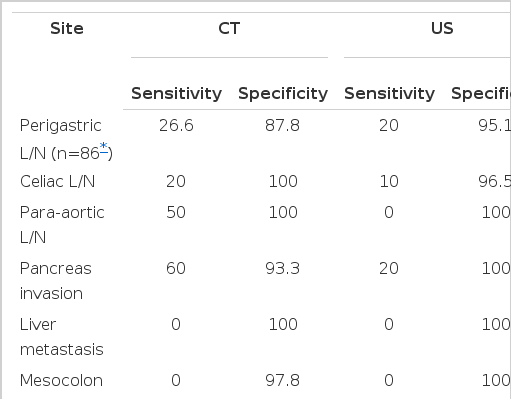
Sensitivities and Specificities of Abdominal CT and US in the Assessment of Tumor Extent (n=95)
2) Extragastric organ involvement and metastases
Five patients were determined to have pancreatic invasion at laparotomy. Three of these were identified using abdominal CT. However, there were 6 false positive diagnoses of pancreatic invasion using abdominal CT. Abdominal US could identify pancreatic invasion in only one of 5 cases, but there were no false positive diagnoses of pancreatic invasion using this method.
There were 4 patients with liver metastases. Several small metastatic nodules were found on the surface of the liver at laparotomy and the size of the nodules was not larger than 1cm in longest diameter. Neither abdominal CT nor US identified the small metastatic nodules.
Mesocolon involvement was found in 2 patients at laparotomy. Neither abdominal CT nor US identified mesocolon involvement, and there were 2 false positive diagnoses of mesocolon involvement by abdominal CT.
Eleven cases of peritoneal tumor seeding were identified at laparotomy. The size of peritoneal tumor seeding was smaller than 1 cm in longest diameter. Neither abdominal CT nor US identified peritoneal tumor seeding.
Specificities and sensitivities of abdominal CT and US in detecting extragastric organ involvement are shown in Table 3.
2. Assessment of Curative Resectability
Of 95 patients who underwent surgical exploration, 14 were found to have unresectable tumors because of extragastric organ involvement and distant metastases. Abdominal CT correctly predicted as resectable 76 of 81 cases in which curative gastric resection was possible. However, abdominal CT falsely predicted as resectable 8 of 14 cases in which curative gastric resection was impossible. Moreover, abdominal CT falsely predicted as unresectable 5 of 81 cases in which curative gastric resection was possible. Abdominal US correctly predicted as resectable 81 cases in which curative surgery was possible. However, abdominal US falsely predicted as resectable 12 of 14 cases in which curative surgery was impossible.
The positive and negative predictive value of abdominal CT and US for curative resectability was shown in Table 4.
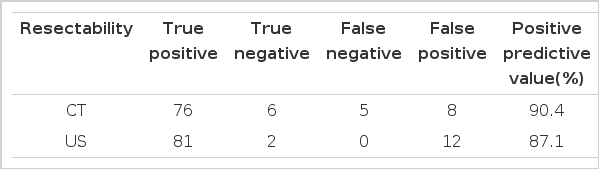
Assessment of Resectabilily of Gastric Adenocarcinoma by Abdominal CT and US (n=95)
DISCUSSION
To our knowledge, this is the largest study of patients with gastric cancer in which results from preoperative abdominal CT and US were prospectively compared with surgical and pathologic findings. In our study, the sensitivities of abdominal CT (26.6%) and US (20%) in detecting the perigastric lymph node involvement were very low. Some investigators have had better results in detecting the lymph node involvement with sensitivity of up to 97%5,12), but others reported poor results8,10). Our poor results of abdominal CT and US in detecting the lymph node involvement may arise from the difficulty in detecting the lymph nodes with metastases that were not enlarged and in distinguishing the enlarged lymph nodes adjacent to primary tumor from adipose tissue2,8,10).
The sensitivity of abdominal CT in predicting the pancreatic invasion (60%) was higher than the sensitivity of abdominal US (20%). However, there were 6 false positive diagnosis of pancreatic invasion by abdominal CT. Sussman et al.10) reported a 27% sensitivity for detection of pancreatic invasion by abdominal CT and found 5 cases of false positive results, for pancreatic invasion. Fraser et al.18) found that invasion of the pancreas was not diagnosed by abdominal CT in 9 of 11 patients studied. CT results, indicating the absence of a fat plane between tumor and the pancreas or a lack of change in relative position of the gastric mass and the pancreas, as described by others9,10), may not be a reliable indicator of invasion and may produce a false positive diagnosis.
Many investigators have had poor results in detecting the liver metastasis. Cook et al.8) and Sussman et al.10) reported sensitivities of abdominal CT detection of liver metastasis of 28% and 29%, respectively. Fraiser et al.18) reported seven false negative results when diagnosing liver metastases by abdominal CT. However, in this study, patients with definite space occupying lesions in the liver detected by abdominal CT or US were excluded from the patients studied, so it was not possible to evaluate the role of abdominal CT and US in detecting the liver metastasis in our selected patients. Nevertheless, abdominal CT and US failed to detect the small sized liver metastatic nodules in all four patients with this diagnosis in our study. Thus, the sensitivity of abdominal CT and US for small metastatic nodules may be very low.
Neither abdominal CT nor US identified mesocolon involvement and peritoneal tumor seeding. All the patients with peritoneal tumor seeding had metastatic nodules smaller than 1cm. Both abdominal CT and US could not identify the smallsized metastatic nodules on the liver surface or on the peritoneum. This is one of the limitations of abdominal CT and US in preoperatively predicting the stage of gastric cancer.
Our results clearly show that abdominal CT and US routinely underestimate the extent of disease. Of even greater significance is that when positive results were obtained with abdominal CT, it tended to overestimate the extent of disease. In five patients, whose tumors had been judged by preoperative abdominal CT to be unresectable, curative gastric resection was possible during exploratory laparotomy. Although abdominal US was less sensitive than abdominal CT in detecting lymph node and extragastric organ involvement, abdominal US did not overestimate the extent of disease once a positive result was obtained. Therefore, although the positive predictive value of curative resection was slightly better for abdominal CT than for abdominal US, the negative predictive value of curative resection was very poor for abdominal CT.
Surgical resection is the treatment of choice for gastric cancer. Carcinoma of the stomach is primarily a regional disease, so aggressive resection is highly justified when the operating surgeon determines that there were no distant metastases19). Therefore, even advanced disease shown using abdominal CT should not deter the use of surgical procedures, as we have shown that abdominal CT often tends to overestimate the extent of disease. Especially, abdominal CT finding of pancreatic invasion by gastric cancer should not be a contraindication for surgical exploration.
In conclusion, in this study, preoperative abdominal CT and US did not accurately predict the extent of tumor growth or curative resectability of the gastric cancer. Therefore, neither abdominal CT nor US studies are alternatives to operative staging. Metastases to the liver are imaged by US with an accuracy equal to or exceeding the13) accuracy of CT13). Therefore, for the preoperative staging of gastric cancer, either abdominal CT or US can be used just for the detection of liver metastases, and every patient without definite evidence of liver metastases should receive surgical exploration.
Notes
This study was supported by a grant, number 02-92-007, from Seoul National University Hospital, Seoul, Korea.