Clinical and Coronary Angiographic Findings of 400 Korean Adults with Coronary Artery Disease
Article information
Abstract
The clinical and angiographic findings of Korean adults with coronary artery disease (obstructions exceeding 50% of the internal diameter of the lumen of one or more major coronary arteries) were studied in 400 of 670 patients on whom selective cinecoronary arteriograms were performed at the Department of Internal Medicine, Yonsei University, College of Medicine between January 1981 and August 1986.
Among the 400 cases with significant coronary atherosclerosis, a clinical diagnosis of unstable angina (including new-onset angina in which angina developed within 3 months) was made in 45.8%, stable angina in 16.0%, variant angina, 3.7%, acute myocardial infarction, 17.3%, and old myocardial infarction, 17.3%.
Single vessel disease was more prevalent in the group with unstable angina (53%) than with stable angina (47%). The incidence of multi-vessel involvement was low in patients with acute myocardial infarction (46%), in contrast to a much higher incidence in the group with old myocardial infarction with angina (76%).
An average of 2.2 lesions resulting in at least 50% luminal narrowing of the major arteries was found per patient. The anterior descending coronary artery was involved more frequently than other vessels.
INTRODUCTION
Symptoms of coronary artery disease generally occur in association with the obstruction of coronary arteries. The development of selective coronary cinearteriography has made possible the correlation of clinical syndromes and evidence of arterial obstruction during life.
The distribution and extent of atherosclerosis within the coronary arterial circulation is well known as an important determinant of treatment and prognosis, but reports of coronary artery disease confirmed by coronary arteriography are almost nonexistent in Korea.
We report, herein, clinical and coronary angiographic findings of 400 Korean adults with coronary artery disease which were confirmed by coronary angiography at the Department of Internal Medicine, Yonsei University College of Medicine.
MATERIALS AND METHODS
1. Patient Group
The clinical records of 670 patients who had selective cinecoronary arteriography between January 1, 1981, and August 31, 1986, were reviewed. Of thease patients, the cases in whom the origin of their cardiac disease was considered to be primarily valvular or myocardial and not atherosclerotic were excluded from this study, and the cases whose findings of angiography revealed narrowing of less than 50 percent in luminal diameter were also excluded. The remaining 400 cases who had significant coronary artery disease (narrowed by 50 percent or more in luminal diameter) were analyzed with clinical and coronary angiographic findings (Fig. 1).
Annual number of coronary angiogram (total 670 cases) performed at severance hospital in the period Jan. 1980–Aug. 1986.
2. Catheterization and Angiographic Procedures
Left-heart catheterization and selective coronary arteriography by the percutaneous femoral approach were performed. Pressures were recorded on a Electronics for Medicine VR-12 oscillographic recorder using Statham P23D transducers and fluid-filled catheters. Single-plane left ventriculography was performed in the 30° right anterior oblique position. Coronary arteriograms were obtained in multiple projections, including angulated views in the sagittal plane. All angiographic images were recorded on 35-mm film at 30 frames per sec and reviewed on a Tagarno projector.
Angiograms were assessed by three independent observers, who independently measured the percent reduction in luminal diameter in the various projections, and discrepancies were resolved by averaging the observed values.
RESULTS
1. Age and Sex Distribution
Of the 400 cases of significant coronary atherosclerosis, 320 were male and 80 female with the male preponderance at a ratio of 4 to 1. The ages ranged from 27 to 79 years. Preponderant age group of coronary artery disease were the sixth decade (37.8%) (Table 1).
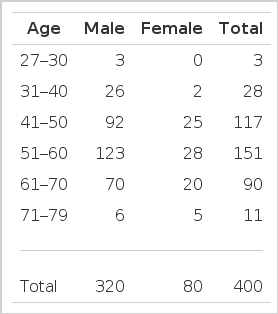
Age and Sex Distribution
2. Major Risk Factors
Of the 400 cases of significant coronary atherosclerosis, the common risk factors were smoking (60.5%), hypertension (38%), hypercholesterolemia (22.0%) and diabetes mellitus (13.8%) (Table 2).
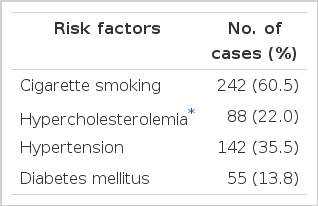
Major Risk Factors in 400 Patients with Coronary Artery Disease
3. Clinical Manifestation and Extent of Coronary Atherosclerosis
Among 400 cases of significant coronary atherosclerosis, clinical diagnosis of unstable angina (45.8%), stable angina (16.0%), variant angina (3.7%), acute myocardial infarction (17.3%) and old myocardial infarction (17.3%) were made. In the groups with unstable angina, variant angina and acute mycoardial infarcation, there was preponderance of single vessel disease. In old myocardial infarction group, multi-vessel disease was more prevalent than single vessel disease (Table 3). Of the 400 cases of coronary artery disease, single vessel involvement was observed in 188 cases (47%), two vessel disease, 100 cases (25%), triple vessel disease, 87 cases (22%), and left main disease, 25 cases (6%) (Table 3).
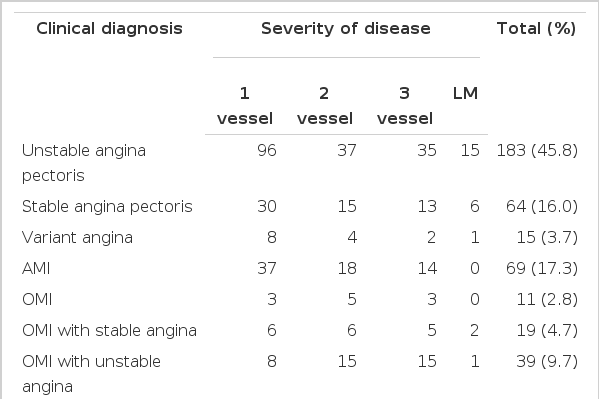
Clinical Manifestations and Severity of Angiographic Findings
4. Distribution of Atherosclerotic Lesions
Fig. 2 and 3 show the distribution of lesions in each of the four arteries. The total number of obstructed arteries in 400 patients was 895, an average of 2.2 per patient. The distribution for the four arteries was left anterior descending artery 46%, left circumflex artery 26%, right coronary artery 25% and left main artery 3%.

Distribution of diseased vessels in left coronary artery.
* LAD : Left anterior descending artery
DB : Diagonal branch
SB : Septal branch
LT.A CX : Left atrial circumflex branch.

Distribution of disease vessels in right coronary artery.
* RCA : Right coronary artery
AM : Acute marginal branch
PD : Posterior descending branch
PL : Posterolateral branch.
DISCUSSION
Since selective coronary arteriography was first performed by Sones1) in 1958, there has been a remarkable development in the methodology of coronary arteriography2–5). Nowadays, selective coronary arteriography is essential for the diagnosis of coronary artery obstructive disease (CAOD), determining treatment modality and prognosis.
In the developed countries, the literature is replete with reports of the clinical and angiographic findings of coronary artery disease6–9). In Korea, however, reports coronary artery disease confirmed by coronary arteriography are still rare.
Herein, we report the clinical and coronary angiographic findings of 400 Korean adults with coronary artery disease confirmed by coronary arteriography.
In our study the sex ratio was 4 to 1. This result is similar to those of Kim et al10) and Proudfit6). Age distribution of our cases was 38% in the 6th, 29% in the 5th and 23% in the 7th decades.
Major risk factors for coronary atherosclerosis in male patients were smoking, hypertension, hypercholesterolemia (≥220 mg%) and diabetes mellitus in the order mentioned, but in female patients they were hypertension, hypercholesterolemia, diabetes mellitus and smoking. Kannel et al11) reported that although the serum total cholesterol is still quite useful for ascertaining risk at ages younger than 50, and probably improved at any age, by an HD lipoprotein cholesterol measurement. Anderson et al12) reported that the degree of coronary artery occlusion was positively related to elevated cholesterol, elevated triglyceride, diabetes, age and history of smoking for both male and female patients and hypertension was related to the degree of occlusion only for female patients.
In this study, single vessel disease was more prevalent in the group with ustable angina including new-onset angina (53%) than in the stable angina group (47%). Victor et al13), Roberts et al14) and Lawson et al15) also reported that new-onset angina group had a higher incidence of single vessel disease than those with chronic angina. The incidence of multi-vessel involvement was low in patients who had acute myocardial infarction (46%), in contrast to a much higher incidence in old myocardial infarction group, especially, with angina (76%). These finding were similar to that of Proudfit16).
Among the 400 patients who had more than a 50% narrowing in luminal diameter in at least one vessel, 188 (47%) and single vessel involvement, 100 (25%), two vessel disease, 87 (22%), triple vessel disease and 25 (6%), left main disease. These findings were similar to those of Ljungberg et al17), but Proundfit et al16) and Bruschke et al8) reported that two vessel disease was most prevalent. The incidence of the left main disease was 6% in our cases, 12% in the study of Ljungberg et al17) and 10.1% in that of Proudfit et al16).
The total number of coronary atherosclerotic lesions among the 400 patients was 895. The average number of arteries affected by the lesions exceeding 50% of the luminal diameter was 2.2 in our study, 1.8 in that of Ljungberg17) and 2.0 in that of Proundfit et al16). The distribution for the four arteries was left anterior descending artery 46%, left circumflex artery 26%, right coronary artery 25%, left main 3%. These findings were similar to those of Proudfit et al16).
Although in our study lesions were more common in the left anterior descending branch of the left coronary artery than at other sites, the difference in incidence in comparison with involvement of the right coronary artery and the circumflex branch of the left coronary artery was not striking. Among 895 lesion sites, proximal (158) and mid (136) portions of left anterior descending coronary artery were the most prevalent sites.
Study of the distribution of severe arterial obstructions did not reveal a pattern characteristic of a clinical syndrome. Only limited conclusions can be reached. Lesions in the left main coronary artery were less common in patients who had myocardial infarction without angina pectoris than in the various groups of patients who had angina pectoris with or without myocardial infarction.
In the absence of anatomic patterns characteristic of a clinical syndrome, symptoms must depend on other variables such collateral circulation, the presence of functional arterial constriction, the cardiac output, the viability of the myocardium distal to the obstruction, the arterial blood pressure, and the regional coronary blood flow. In this study the presence or absence of evidence of collateral circulation was not noted, because this information was difficult to tabulate.
In this study we suggest that in Korea the prevalent age of CAOD is older and the incidence of multivessel disease is lower than that in the developed countries.