The Clinical Utility of Microalbuminuria in Nephrotic Syndrome with Complete Remission, Isolated Microscopic Hematuria and Renal Transplantation Donors
Article information
Abstract
Using urinary microalbumin radioimmunoassay, we evaluated the clinical utility of microalbumin excretion in nephrotic syndrome with complete remission, isolated microscopic hematuria and kidney donors in reanl transplantation. The highest value in normal controls was 10.86 μg/min, and the upper normal level was set to 15 μg/min.
The range of microalbuminuria in patients with nephrotic syndrome with complete remission was 1.67 μg/min to 32.5 μg/min. There was no significant correlation between the recurrence rate and microlbuminuria level in nephrotic syndrome with complete remission. The range of microalbuminuria levels in isolated microscopic hematuric patients was between 2.37μg/min and 103.2 μg/min.
There was no singificant correlation between the amount of the red blood cells in urine and the level of microalbuminuria in the isolated microscopic hematuric patients. Most renal transplantation donors showed a normal range of microalbuminuria after nephrectomy. The aim of this study was to evaluate the clinical utility of urinary microalbuminuria in diseases other than diabetes. We concluded that further extensive and specific study will be required to determine the clinical utility of microalbuminuria.
INTRODUCTON
Since the development of radioimmunoassay for the specific and sensitive measurement of low concentrations of urinary albumin1) it is possible to predict the development of diabetic nephropathy in diabetes.2) It is observed in Type I and Type II diabetes that a slight to moderate increase in urinary albumin concentration, to a level not generally measurable by standard clinical tests, is associated with a considerable increase in mortality as well clinical renal disease4–5). Vigstrup and Mogensen6–7) documented that even a slightly raised urinary albumin excretion (UAE) far below the level of clinical proteinuria, is a strong predictor with respect to development of proliferative diabetic retinopathy, as well as nephropathy. To study the effects of improved control of blood glucose on markers of renal glomerular and tubular function, Urinary excretion rates of albumin were used in clinically nonproteinuric diabetic patients.8)
Irgens-Möller9) documented that the measurement of microalbumin can be used as a more discriminatory diagnostic test, a monitoring therapy or for control of pre-eclampsia. Recently, microalbuminuria has also been considered as a early diagnostic predictor of lupus nephritis in SLE.10)
In spite of the increased tendency to use microalbuminuria in the diagnosis of diabetes, in a number of other potential causes of microalbuminuria-e.g. exercise, non-diabetic renal or systemic disease-it has not been used actively.
The purpose of this study is to clarify whether microalbuminuria will be clinically useful in predicting relapse in nephrotic syndrome with complete remission, IgA nephropathy and the kidney donor in renal transplant.
PATIENTS AND METHODS
Patients: Fourty-six patients were studied. Of these, 18 had nephrotic syndrome in the complete remission state (ages 18 to 58 years, mean: 33.1 years), 7 of the 18 patients had minimal change, 5 had membranous glomerulopathy, 2 had the proliferative type and 4 were not determined by renal biopsy. Another 18 patients were isolated microspcopic hematuria (ages 17 to 69 years, mean: 39.7 years), 10 of these were determined as IgA nephropathy by renal biopsy and 8 were only clinically diagnosed as IgA nephropathy. Ten patients were kidney donors in kidney trasplantations (age 24 to 59 years, mean: 39.4 years) who had been observed for 6 months or longer. There were 20 apparently healthy controls (ages 23 to 35 years, mean 26.8 years).
In all groups, clinical albuminuria (Albustix) was not observed and the plasma creatinin level was below 1.3 mg/dl. Patients with diabetes mellitus, urinary tract infection and renal failure were exluded in this study. In all patients with isolated microscopic hematuria, the intravenous pyelogram was normal.
METHODS
All subjects collected urine for 24 hours in a relatively stable state. They were permitted to perform ordinary activities. The urine volume was recorded and aliquots were stored at −20°C until analysis of the albumin concentration by radioimmunoassay (Diagnostic products Co. LA, USA) with a double antibody.
RESULTS
The Results are all Summarized in Table 1.
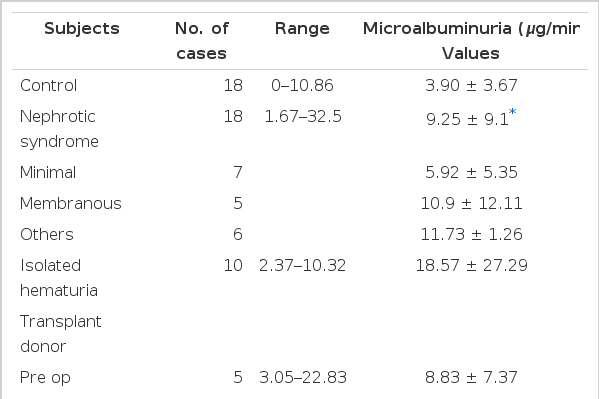
Urinary Microalbuminuria in Controls, Nephrotic Syndrome with Complete Remission, Isolated Microscopic Hematuria and Renal Transplantation Donors
1) Microalbuminuria in Normal Healthy Controls and Nephrotic Syndrome with Complete Remission State.
Fig. 1 shows the microalbuminuria levels in the controls and nephrotic syndrome patients. The highest value in normal controls was 10.86 μg/min. The upper normal level was set to 15 μg/min. The range of microalbuminuria levels in nephrotic syndrome with complete remission was between 1.67 μg/min and 32.5 μg/min. Of these 18 nephrotic syndrome patients, 13 had microalbuminuria levels below 15 μg/min (72.2%) and 5 had microalbuminuria levels above 15 μg/min (27.8%). There was no significant correlation between microalbuminuria levels and the type of nephrotic syndrome. There was also no significant correlation between the rate of recurrence and microalbuminuria levels in nephrotic syndrome patients with complete remission (Table 2).
Microalbuminuria in control and nephrotic syndrome.

Relationship Between Recurrence rate and Microalbuminuria in Nephrotic Syndrome
2) Isolated Microscopic Hematuria
Figure 2 shows microalbuminuria levels in the controls and isolated microscopic hematuria patients. The range of microalbuminuria levels in isolated hematuria patients was between 2.37 μg/min and 103.2 μg/min. Of these 18 patients, 14 had microalbuminuria levels below 15 μg/min (77.8%) and 4 had microalbuminuria levels above 15 μg/min (22.2%). Figure 3 shows the relationship between microalbuminuria levels and the number of red blood cells in urine. There was no significant correlation between these results.

Microalbuminuria in isolated hematuria.
Microalbuminuria in isolated hematuria as related to the number of red blood cells (RBC) in Urine.
3) Kidney Donor in Renal Transplantation
The range of preoperative microalbuminuria in kidney donors was between 3.05 μg/min and 22.8 μg/min. The patient with the highest level was checked just after renal arteriography. The postoperative 1 week range of microalbuminuria was between 6.27 μg/min and 32.5 μg/min. Figure 4 shows the change of microalbuminuria levels after nephrectomy. Of these 5 patients, 4 had microalbuminuria levels below 15 μg/min and one still showed a level as high as 30.68 μg/min.
Microalbuminuria in renal transplant donors.
DISCUSSION
Many investigators documented that even a slightly elevated rate of urinary albumin excretion in diabetes- far below the level found in clinical proteinuria-is a strong predictor of the development of overt diabetic nephropathy. The albumin excretion rate in patients with clinical proteinuria is generally above 200 to 300 μg/min. Recently, Mogensen and Christensen5) demonstrated evidence that patients with initial albumin excretion rates below 15 μg/min generally did not later have clinical proteinuria but patients with rates at or above 15 μg/min generally did have clinical proteinuria. Thus, they set the normal value of the albumin excretion rate below 15 μg/min.
The present study observed that the range of albumin excretion rates in normal healthy persons is below 11 μg/min, and this very similar to the normal value level set by Mogensen and Christensen.
In our country, Cha et al.,11) first studied the prevalence of microalbuminuria and its associated factors in Type II diabetes and demonstrated that microalbuminuria was positively correlated with fasting blood glucose leves and the incidence of hypertension and diabetic retinopathy.
The clinical utility of microalbuminuria in nephrotic syndrome has not yet been demonstsated. In this study, most of the nephrotic syndrome patients with complete remission showed normal ranges of microalbuminuria. But in a few patients, high values of microalbuminuria were observed. There was no significant correlation between microalbuminuria levels and the type of nephrotic syndrome. It will be observed prospectively whether there will be a significant correlation between relapsing tendency and microalbuminuria levels in nephrotic syndrome patients with complete remission.
Most isolated microscopic hematuric patients had microalbuminuria levels in the normal range. A few patients had microalbuminuria levels high above the normal range. The difference of prognosis between these two groups will be studied prospectively. There was no significant correlation between microalbuminuria levels and the number of red blood cells in urine.
This study also observed microalbuminuria in kidney donors of renal transplantation. Seven days after nephrectomy, 4 of 5 patients had microalbuminuria levels higher than the preoperative level. This observation is considered as an initial postoperative complication. After 6 months, 4 of 5 patients had microalbuminuria levels in the normal range. In one patient, microalbuminuria still showed a much higher level and this patient’s progress will be observed continuously.
Although radioimmunoassay is a sensitive technique, it is technically complex and requires expensive equipment. Thus, simple and more inexpensive techniques employing fluoresceinated or enzyme-linked immunosorbant assays (ELISA) have been developed.12)
Thus, the present study is a trial to establish the clinical utility of microalbuminuria in diseases other than diabetes such as nephrotic syndrome, IgA nephropathy, kidney donors and so on. Further extensive and specific study will be required to establish the clinical utility of microalbuminuria.