Hepatitis C Infection in Hemodialysis Units
Article information
Abstract
We performed an epidemiological study of the hepatitis C infection on 112 patients of 3 urban hemodialysis units using a recently developed anti-HCV recombinant based assay. Eleven patients (9.8%) were positive for anti-HCV. Among them, 8 (72.7%) were positive for anti-HBc, one of whom was HBsAg positive and 6 of whom were also anti-HBs positive. Surprisingly, all of the anti-HCV (+) patients were normal alanine aminotransferase. The mean age of the anti-HCV (+) patients was 50.7 ± 3.3 (mean ± SE) and that of the anti-HCV (–) was 47.6 ± 1.3. The mean duration (month) of hemodialysis of the anti-HCV (+) and anti-HCV (–) groups were 52.7 ± 7.2 (mean ± SE) and 60.9 ± 9.7, respectively. The prevalence of anti-HCV among anti-HBc positive subjects was 9.5% and that among anti-HBc negative subjects was 17.6%. This didn’t have any statistical significance according to the criteria of the study (p = 0.308). The prevalence of anti-HCV among the transfusion positive group was 11.0% and that of the transfusion negative group was 7.7%. This data showed the tendency for a higher prevalence of anti-HCV among the trasnfusion positive group, but this also didn’t reach statistical significance (p = 0.424). Of the 40 normal controls, none were anti-HCV positive. The prevalence of HBsAg in our hemodialysis units was 12.5%. This rate was not so much higher than the average population in Korea. The prevalence of anti-HCV and previous hepatitis B virus infection also had no significant relationship.
This data suggests that the prevalence of HCV in hemodialysis units is higher than the normal population. The prevalence of HCV is not definitely associated with age, duration of dialysis, previous HBV infection status, or history of transfusion.
INTRODUCTION
Infectious hepatitis is a major problem for patients undergoing maintenance hemodialysis and for staff caring for these patients1). Before 1970, hepatitis B was the major cause of hepatitis in dialysis units. In 1967, Blumberg et al. discovered the “Australia antigen” which was found to be related to viral hepatitis2). Later this was confirmed to HBsAg identified as the surface antigen of the hepatitis B virus (HVB). With the advent of universal blood screening for HBsAg in 1972, the single-most control measure for hepatitis B was instituted. This measure prevented the development of hepatitis B infection in transfused patients3,4). With the development of sensitive serologic tests for hepatitis A and B virus, non-A, non-B (NANB) hepatitis has emerged as a newly recognized type of hepatitis among dialysis patients5). The diagnosis of NANB hepatitis is at the present time one of exclusion of other viruses for which serologic markers are abailable. In 1989, Kuo et al.6) introduced a new assay for hepatitis C antibodies, and this new method prompted us to investigate the prevalence of hepatitis C infection in our hemodialysis units.
PATIENTS AND METHODS
During February 1990, 112 hemodialysis patients at the dialysis centers of Severance Hospital, Yongdong Severance Hospital, and Dr. Chung’s Dialysis Clinic were Studied. Routine hemodialysis techiques were used with 4-or 6-hour treatments performed twice or thrice weekly. Sera from the study subjects were obtained during February of 1990. All patients had routine periodic liver function tests including serum alanine aminotransferase (ALT), alkaline phosphatase, lactic dehydrogenase (LDH), and bilirubin, Hepatitis B suface antigen (HBsAg) and antibody (Anti-HBs) and hepatitis B core antibody (Anti-HBc) were checked by commercial kits (Genedia, Green Cross Corp., Seoul, Korea, and Corzyme, Abbott Lab., North Chicago, IL, USA). Anti-HCV was measured by the method of Kuo et al.6) In this assay, a polypeptide synthesized in recombinant yeast cloned of HCV was used to capture circulating viral antibodies. Statistical analyses for two-way tables were tested using the Fisher’s Exact probability test. Other variables were analyzed using the Student t-test.
RESULTS
Eleven patients (9.8%) were positive for anti-HCV. Among them, 8 (72.7%) were positive for anti-HBc, One of whom were also anti-HBs positive. Surprisingly, all of the anti-HCV (+) patients were normal alanine amonotransferase (Table 1). The mean age of the anti-HCV (+) patients was 50. 7 ± 3.3 (mean ± SE) and that of the anti-HCV (–) was 47.6 ± 1.3. Themeanduration(month)ofhemodialysis of the anti-HCV (+) and anti-HCV (–) groups were 52.7 ± 7.2 (mean ± SE) and 60.9 ± 9.7, respectively. The age and mean duration of hemodialysis of the two groups were not statistically different (p>0.05). We did an analysis to determine whether the presence of anti-HCV and anti-HBc were related to each other (Table 2). The prevalence of anti-HCV among anti-HBc positive subjects was 9.5% and that among anit-HBc negative subjects was 17.6%. This didn’t have any statistical significance according to the criteria of the study (p = 0.308). We compared the prevalence of anti-HCV and the history of transfusion. Table 3 shows that the prevalence of aniti-HCV among the transfusion positive group was 11.0% and that of the transfusion negative group was 7.7%. This data showed a tendency for a higher prevalence of anit-HCV among the transfusion positive group, but this also, didn’t reach statistical significance (p = 0.424). The prevalence of HBsAg in our hemodialysis units was 12.5% (Table 4). This rate was not so much higher than the average population in Korea. The prevalence of anti-HCV and previous hepatitis B virus infection also had no significant relationship.
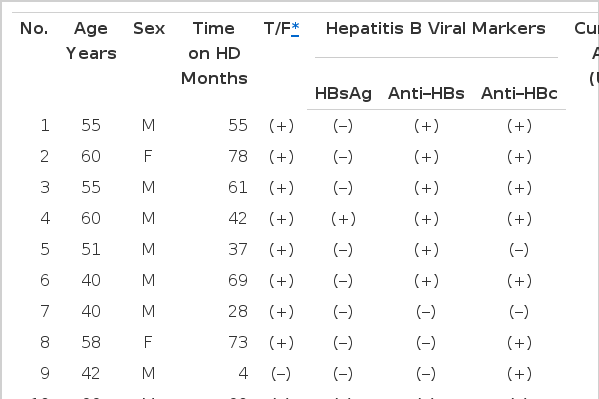
Clinical and Laboratory Characteristics of Anti–HCV (+) Patients

Prevalence and Association of Antibodies to HCV and HBc

Prevalence and Association of Transfusion History and Anti–HCV

Prevalence of Hepatitis B Viral Markers and Anti–HCV in Hemodialysis Patients
DISCUSSION
Infectious hepatitis is a major problem for patients undergoing hemodialysis because these patients had frequent transfusions and depressed immunity1,7,8). Implementation of sensitive testing for hepatitis B virus in the early 1970’s reduced the incidence of post-transfusion hepatitis9). However, post-transfusion hepatitis is still a problem for hemodialysis units, and this hepatitis is caused by an as yet unidentified virus. The term non-A, non-B hepatitis has been used to describe hepatitis in patients who do not develop antibodies to hepatitis A virus, hepatitis B virus, cytomegalovirus or Epstein-Barr virus nor have a clinical history of other potential causes of hepatitis10). Recombinant DNA technology opened a new era in research on and control of non-A, non-B hepatitis. The cloning and sequencing of hepatitis C virus and the development of a new serologic assay to detect antibody to a part of this virus (anit-HCV) have been major break throughs in the search for a causative agent of non-A, non-B hepatitis. Kuo et al.6) cloned an agent, designated hepatitis C virus (HCV), from the plasma of a chronic non-A, non-B hepatitis chimpanzee that led to the development of a recombinant antigen (c100-3) which was used in an assay to identify antibodies to HCV (anti-HCV). A previous report suggests that hepatitis C virus is a major cause of non-A, non-B hepatitis throughout the world6). In our hemodialysis patients, the prevalence of HCV was 9.8%. Several recent surveys from USA10), Spain11) and Germany12) show the prevalence of HCV of 12%, 20%, and 5.5%, respectively. Our prevalence rate was slightly lower than the rates of USA and Spain. Surprisingly, all of our anti-HCV positive patients had normal liver function tests and no evidence of current hepatitis. The detection of anti-HCV indicates that the infection occurred at some time with hepatitis C virus or that the person has an ongoing infection. This antibody may not indicate recovery from a past infection. Whether or not all anti-HCV positive individuals are carriers of the hepatitis C virus is not yet known13). Clinical evaluation and follow-up of these individuals should answer this question. We compared the prevalence of anti-HCV and the history of transfusion. The prevalence of HCV among the positive transfusion history group was 11.0% and that of the negative transfusion history group was 7.7%. This data revealed a slightly higher prevalence rate of anti-HCV among the transfusion positive group, but this didn’t have statistical significance. Jeffers et al.10) also reported that there was no significant correlation between the prevalence of HCV and a history of blood transfusion. However, the number of transfusion units was significantly higher in the anti-HCV positive patients. The incidence of anti-HCV in patients at risk were variously reported. In the study from Spain11), the incidence of anti-HCV in patients at risk was intravenous drug abusers 70%, post-transfusion NANB hepatitis 80%, and hemodialysis patients 20%. In the study from the USA10), the rate was much lower than the study from Spain. Our hemodialysis patients also had a lower prevalence rate than the studies from the USA and Spain. Before the advent of anti-HCV test, anti-HBc and serum alanine aminotransferase (ALT) were used as surrogate markers for non-A, non-B hepatitis14). In some recently reported data, a surrogate assay for anti-HBc would have detected only half of the anti-HCV positive donors involved in the transmission of hepatitis15). The association of positive anti-HBc and the prevalence of HCV was suggested by the study of Jeffers er al.6), but the statistical significance was borderline. Our results also showed no significant association.
In conclusion, the prevalence of HCV in hemodialysis units is higher than in the normal population. The prevalence of HCV is not definitely associated with age, duration of dialysis, previous HBV infection status, or history of transfusion. However, the elimination of anti-HCV positive blood from the blood donor pool and scrupulous infection control measures in hemodialysis units such as the use of gloves, proper disposal of needles, cleaning of dialysis machines, and separation of anti-HCV positive patients may be beneficial in reducing hepatitis C infection in dialysis units.