Correlation of Esophageal Lengths with Measurable External Parameters
Article information
Abstract
Previous data for esophageal lengths are based on age related groups or cadaveric examination, both of which are improper for application to various individualized procedures. Because of the variability in height for any given age and longer length in vivo, lindividualized approximation is needed. Thus, we measured various anatomical levels of the esophagus using a flexible endoscope and correlated these data with measurable external body intervals.
The mean esophageal length was 40.92±2.79, which is longer than the length derived from cadaveric examinations. Also, esophageal lengths which correlated better with height than any other body intervals, could be calculated from the following equation. Esophageal length from the upper incisors to the esophagogastric junction (L) can be expressed: L = 0.242 × height (Ht) + 2.078cm (P = 0.000, R2 = 0525).
The data from our study indicate that esophageal length can be reliably predicted using external body parameters before employing various procedures.
INTRODUCTION
Anatomists have observed that the length of the esophagus, i.e. the distance from the incisors to the esophagogastric junction1–4), varies in different individuals from 32 to 50cm.
By endoscopy, the usual length of on adult essphagus is measured as 40 cm from the incisor to the point where mucosal change occurs5–6), but the esophageal length varies from one person to another according to physical status. This variability is often experienced when trying to insert a pH meter, manometer or even nasogastric tube, or when placing the prosthesis for benign or malignant stenosis.
We measured various lengths of esophagi in korean adults using a flexible fibercope and measured the external body intervals. Then, we analyzed these data and extrapolated the various esophageal lengths with measurable external body intervals to obtain the correlations. The regressive equation was derived from these trials to approximate the true esophageal lengths.
MATERIALS AND METHODS
The study was conducted for the measurement of esophageal length in 196 persons, 97 males and 99 females, with normal esophagogastric endoscopic findings. The distribution of age was from 16 to 77.
The distances from the upper incisors to 5 anatomical levels of esophagus (cricopharyngeus narrowing, aortic narrowing, left main bronchus narrowing, hiatus and gastroesophageal junction) were measured by an endoscope with 1cm markings (Olympus Co. Q20 foreward view) (Fig. 1). Each length was the mean value of double measurements during full inspiration and expiration respectively.
An endoscope with 1cm markings (Olympus Co., Q20 foreward view)
The external body interval lengths studied were standing height, sitting height, the distance from the 7th vertebra to the coccyx and the distance from the upper incisors to the external occipital protuberance. The standing height and sitting height were measured with standard physical examination devices. The distance from the 7th cervical vertebra to the coccyx was measured with a tape measure. A specially designed measure was used for the distance from the incisors to the external occipital protuberance (Fig. 2).

The specially designed device used to measure the distance from the incisors to the occiput
Data analysis and correlation of esophageal lengths to external body intervals were done using SPSS/pc+ (Statistical Package for Social Science/pc+).
RESULTS
The mean age of the group studied was 45.5±14.54 years. Their heights ranged from 133 to 182 cm.
Observations have shown great variation in the length of the esophagus in adults but good correlation between esophageal lengths and external parameters. The measured lengths of external body intervals and various anatomical esophageal levels are depicted in Table 1.
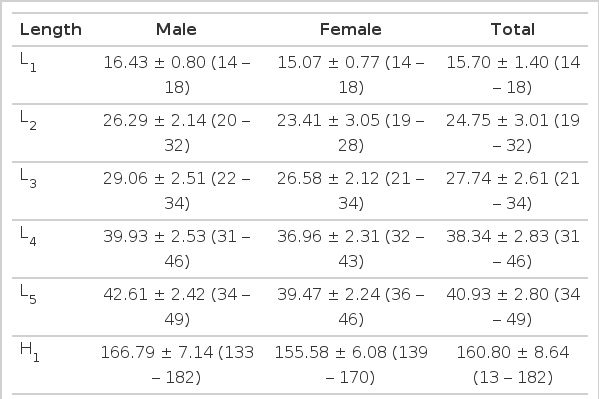
Mean Esophageal Length and Anatomical Variables
Abbreviations used:
The mean standing-height and sitting-height of 196 persons studied were 160.80±8.64 cm and 86.60±5.91 cm, respectively.
The interval from the upper incisors to each anatomical landmark of the esophagus (cricopharyngeal narrowing, aortic arch compression, left main bronchus compression, hiatus, and esophagogastric junction) were 15.70 cm, respectively. The true esophageal length, which is the distance from the cricopharyngeal narrowing to the esophagogastric junction, was 24.93±2.76cm.
The correlation of each esophageal anatomical level with external body intervals using the multiple stepwise reggression method is shown in Table 2.
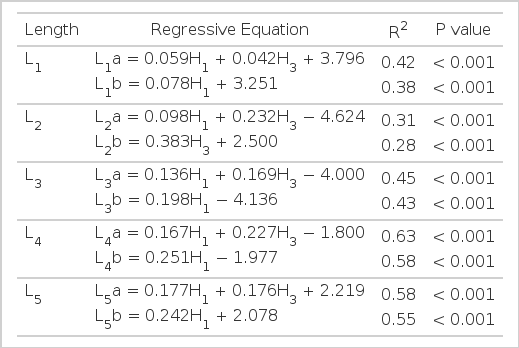
Estimation of Distances of Various Esophageal Levels from Incisors Using Anatomic Variables
Each of these 4 external variables was statistically significant, but better correlations were demonstrated by the H1 and H3. Although we employed the measurable distance (H4) instead of the unmeasurable distance (L1), the equations using H4 and H2 did not express the esophageal lengths more accurately than the equation using H1 and H3 only.
For example, the distance from the incisors to the esophagogastric junction (L5) could be neatly expressed in simple equations as the following:
Likewise, all other esophageal lengths could be approximated with the equations using H1 and H3 or with the equation using H1 only.
DISCUSSION
The development of improved capability in medical and surgical managment of esophageal disease processes has been significant. To understand and appropriately use current technologic advancements, the anatomic properties of the esophagus must be appreciated3). Available information about esophageal length, however, has been based on cadaveric measurements, because it is not feasible to measure esophageal length in vivo.
In adults, the distances from the incisor teeth to the esophagogastric junction have been described to be in the range of 32–50 cm by various studies1–4), and the described distance from the cricopharyngeus narrowing to the esophagogastric junction usually varies from 20 to 30cm1–2).
On the other hand, Jackson7) described esophageal lengths according to various age groups.
But such wide ranges of esophageal values and different physical status even in the same age group hamper the application of these data to individual patients in esophageal procedures.
The best approximation of esophageal length would be useful for various clinical procedures, such as placement of a pH meter, manometer and nasogastric tubes, insertion of an endoprosthesis and colonic interpostition for both benign and malignant stenotic segments. There have been several studies8–10) in order to approximate the true esophageal lengths. We conducted this study to determine the mean esophageal length of various anatomical levels and to derive a method approximating true esophageal lengths.
Data were analyzed from 196 persons who completed the study. The mean esophageal lengths from the upper incisors to the esophagogastric junction were 42.61±2.42cm in men and 39.47±2.24cm in women.
These values are not smaller than Western data despite the fact that Koreans are shorter. This is possible because previous data were based on cadaveric examination and Koreans have a different racial stature.
We correlated several external body intervals with esophageal lengths by the multiple stepwise regression method: standing height, sitting height, the distance from the 7th cervical vertebra to the coccyx and the distance from the upper incisors to the occiput. All external parameters significantly correlated with the true esophageal lengths.
Based on our results, the distance from the upper incisors to the esophagogastric junction (L5) can be best approximated by employing following equations:
But accuracy determined by the other equations using more variables other than height did not increase remarkably despite their complexities. Likewise, other anatomical levels of the esophagus can be predicted accurately as shown in the previous results.
In conclusion, we consider that an accurate appraisal of the true length of an adult esophagus can be made by measuring the height and the other external measurable parameters. This finding will be extremely useful in various esophageal procedures.