A Case of Type B Dissecting Aneurysm Involving Right Sided Aorta with Kommerell's Diverticulum
Article information
Abstract
A right-sided aortic arch (RAA) is a rare congenital anomaly, and Stanford type B dissection aneurysms involving this anomaly is also uncommon. Surgical approaches to dealing with an RAA are complicated by the unusual anatomical features of the condition. Here we report the case of a 47-year-old male who had a type B dissecting aneurysm involving an RAA with Kommerell's diverticulum. Graft replacement was successfully performed with an uneventful postoperative course.
INTRODUCTION
Right sided aortic arch (RAA) is an uncommon congenital anomaly with an incidence of 0.1%, and aortic dissection involving RAA is rare [1]. The surgical approach for a RAA aneurysm remains a complicated problem entity because of its anatomical characteristics. We present a case of type B dissecting aneurysm involving a RAA with Kommerell's diverticulum, in which a successful graft replacement was performed via right posterolateral thoracotomy.
CASE REPORT
A 47-year-old male with a history of hypertension requiring medication was admitted to our hospital due to chest pain, which is a dull ache and is radiated to the back. The patient's vital signs were stable. Electrocardiography showed no evidence of myocardial ischemia, and transthoracic echocardiography showed a normal left ventricular ejection fraction and no regional wall motion abnormalities. However, a chest X-ray showed mediastinal widening with a right-sided convex-shaped shadow (Fig. 1). Subsequent chest computed tomography revealed a dissecting aneurysm involving a right-sided aorta with Kommerell's diverticulum. The dissection started just distal to the left subclavian artery and propagated to the level of the renal artery, forming an aneurysm with a maximal diameter of 10.5 cm (Fig. 2). An entry tear was detected at the lower thoracic aorta, with two reentry tears at the celiac and renal arterial levels (Fig. 3). The superior mesenteric artery and right renal artery originated from the true lumen, while the celiac trunk and left renal artery originated from the false lumen. The abdominal aorta was located on the left side.
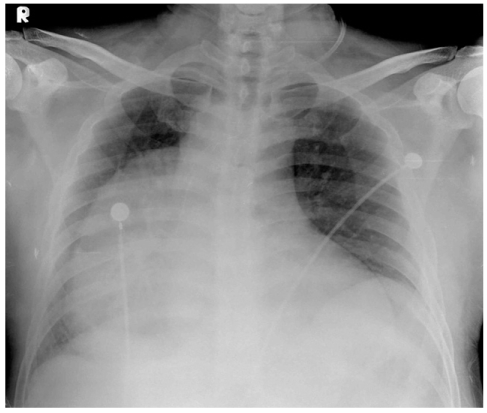
Chest X-ray showing mediastinal widening with a right-sided convex-shaped shadow.
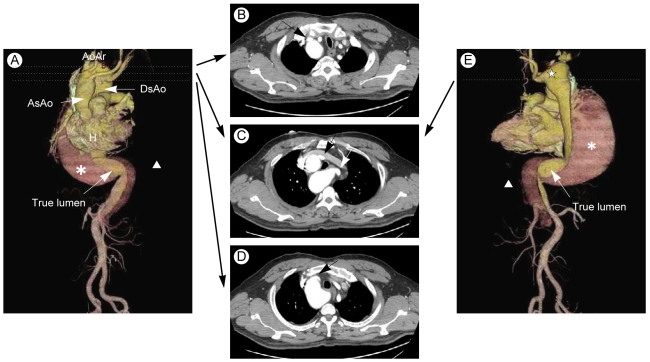
Three-dimensional multiplanar reformats post-processing and axial view of the thoracic computed tomography scan with contrast enhancement. (A) Anteroposterior view. The order of the great vessels from the right-sided aortic arch were as follows: left common carotid artery, right common carotid artery, right subclavian artery, and left subclavian artery. (B) Origin of the left common carotid artery (arrow). (C) Origin of the right common carotid artery (black arrow) and left subclavian artery (white arrow) from Kommerell's diverticulum. (D) Origin of the right subclavian artery (arrow). (E) Posteroanterior view. Kommerell's diverticulum (★) with an aberrant left subclavian artery. *, asterisk, dissecting aneurysm; arrowhead, false lumen; H, heart; As Ao, ascending aorta; Ao Ar, aortic arch; Ds Ao, descending aorta.

(A) Computed tomography scan showing a 10.5-cm type B thoracoabdominal aortic dissecting aneurysm (▲, true lumen; ★, false lumen) with an entry tear (white arrow). (B) Optimal exposure of the operative field via right posterolateral thoracotomy (▲, dissecting aneurysm; ←, cranial; →, caudal). (C) Entry tear in the descending aortic dissection (arrow).
Surgical intervention was indicated due to signs of impending rupture, periaortic fluid collection, and an increase in size. A right posterolateral thoracotomy was performed, which adequately exposed the right aortic arch and right descending aorta. A cardiopulmonary bypass was started after cannulation of the right common femoral artery and vein. The patient was cooled to 20℃. During circulatory arrest, a 28-mm tube graft with a 10-mm side arm was anastomosed proximally at the distal aberrant left subclavian artery. Next, the circulation was started with the graft-side arm cannulation. During the rewarming period, a distal anastomosis was performed after generous resection of the distal dissection flap. The postoperative course was uneventful, and the patient remained well during the 6-month follow-up period.
DISCUSSION
RAA is a rare congenital anomaly with a general incidence of approximately 0.1% [1]. Embryologically, the aortic arch is formed from the left aortic arch as the right aortic arch degenerates. However, if the left instead of the right aortic arch degenerates, the aortic arch will be formed from the right aortic arch [2,3]. The result can be classified into three types, depending on the pattern of degeneration of the left aortic arch and the branching pattern of the great vessels [2,3]. The so-called mirror image pattern is an uncommon type in which the great vessels originate from the arch in the following order: left innominate artery, right common carotid artery, and right subclavian artery. A mirror image-type right aortic arch was shown to be associated with major congenital heart disease in 98% of patients, including tetralogy of Fallot, truncus arteriosus, and tricuspid atresia [3,4]. The most common type occurs when the great vessels originate from the arch in the following order: left common carotid artery, right common carotid artery, right subclavian artery, and left subclavian artery originating from Kommerell's diverticulum. This type is less frequently associated with major cardiac anomalies (5 to 10%) [2,4-6]. The only cardiac anomaly in the present case was an aberrant left subclavian artery originating from Kommerell's diverticulum. The third and rarest type occurs when the left common carotid artery, right common carotid artery, and right subclavian artery originate in order from the right aorta, and the left subclavian artery is not connected [3,7]. Most patients with an RAA are asymptomatic; however, tracheoesophageal compression may occur due to a vascular ring that develops from the ductus arteriosus, which connects the left pulmonary artery to the left subclavian artery or Kommerell's diverticulum [5-7].
The true incidence of a right-sided aortic aneurysm or dissection is unknown, but aortic dissection does not appear to be increased in frequency in individuals with a right aortic arch [6]. However, Bodine et al. [8] suggested that a type B dissection developed more frequently than other types of dissection in patients with an RAA. Patients with an RAA have a shorter radius and more acute curvature of the arch compared with the usual gentle curve of the left aortic arch. This change in direction of blood flow from the cephalic to the caudal represents an additional stress to the tissues in the vessel wall, which could predispose affected individuals to a type B dissection in the RAA [7,8]. In our case, the dissection was of Stanford type B; thus, it did not involve the ascending aorta and it extended to the renal arterial level distally. For treatment, a surgical approach is the most important consideration because the anatomical features of a right-sided aorta present specific technical problems compared with a normal left-sided aorta. Commonly used surgical approaches in such cases include a midline sternotomy, right thoracotomy, left thoracotomy, and bilateral thoracotomy; however, these approaches may not be appropriate for a complete repair [9,10]. The surgical intervention in our case was performed successfully by right posterolateral thoracotomy, and the patient's postoperative course was uneventful.
In conclusion, aortic dissection involving a right-sided aorta is a rare condition, and right posterolateral thoracotomy may be a good method to adequately expose an RAA.
Notes
No potential conflict of interest relevant to this article was reported.