Causes and Treatment Outcomes of Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in 82 Adult Patients
Article information
Abstract
Background/Aims
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are predominantly known as medication-induced diseases. However, at our institution, we have experienced more cases of non-drug-related SJS and TEN than expected. Therefore, we studied the difference between non-drug-related and drug-related SJS and TEN in terms of clinical characteristics and prognoses.
Methods
The etiologies, clinical characteristics, and treatment outcomes for 82 adult patients with SJS and TEN were retrospectively reviewed.
Results
A total of 71 patients (86.6%) were classified as having SJS, and the other 11 patients (13.4%) were classified as having TEN. Drug-related cases were more common (43, 52.4%) than non-drug-related cases (39, 47.6%). Anticonvulsants (12/82, 14.6%) and antibiotics (9/82, 11%) were the most common causative medications. Anemia (p = 0.017) and C-reactive protein of ≥ 5 mg/dL (p = 0.026) were more common in the drug-related cases than in the non-drug-related cases. Intravenous steroid therapy was used as the main treatment regimen (70/82, 85.4%). Of the 82 patients, 8 (9.8%) died during the clinical course. A univariate analysis for mortality showed statistical significance for the following: kidney function abnormality, pneumonia, hemoglobin of < 10 g/dL, and combined underlying diseases. In a multivariate analysis, only pneumonia was statistically significant (odds ratio, 25.79; p = 0.009).
Conclusions
Drugs were the most frequent cause of these diseases. However, non-drug-related causes also contributed to a significant proportion of cases. Physicians should keep this in mind when documenting patient history. In addition, early recognition and treatment may be important for better outcomes.
INTRODUCTION
Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are rare but severe and potentially fatal mucocutaneous diseases characterized by widespread epidermal necrosis and mucosal involvement [1,2]. At least 80% of TEN cases are believed to be drug-induced, whereas the proportion of SJS cases attributable to drugs is somewhat lower, with the estimates ranging between 50% and 80% [2,3]. We recently encountered more non-drug-related SJS and TEN cases than expected in our clinical practice. Several infectious etiologies have also been implicated in SJS and TEN. Mycoplasma pneumoniae and herpes simplex virus are the most commonly reported [4-7]. A severity-of-illness score for TEN, abbreviated as SCORTEN, was developed by Bastuji-Garin et al. [8]. In another study conducted in 2008, the risk of death was strongly correlated to the patient's age and to the severity of the disease [9]. However, few reports on the prognostic factors of SJS and TEN have also included their etiologies. Therefore, in the present study, the etiologies, clinical characteristics, and treatment outcomes for a number of adult patients with SJS or TEN were evaluated.
METHODS
Subjects
All patients who had been consecutively admitted to Kyungpook National University Hospital with a diagnosis of SJS or TEN within the period from June 3, 2001 to June 12, 2011, were included. The patients were classified as having SJS or TEN based on the diagnostic criteria reported by Power et al. [10]. This study was approved by the institutional review board of the authors' hospital (No. KNUH-07-019).
Clinical data
Data were collected by reviewing the electronic medical database and patient charts. The medical records of the patients were examined to obtain the following data: patient demographics, presenting symptoms, causative drugs or events, extent of mucocutaneous involvement, laboratory tests, medical comorbidities, ocular complications, interval between symptom development and treatment, and treatment outcome. SJS was characterized by an epidermal detachment of < 30% of the body surface area, and TEN was characterized by an epidermal detachment of > 30% of the body surface area [11]. Table 1 summarizes the definitions of the clinical characteristics that were investigated.
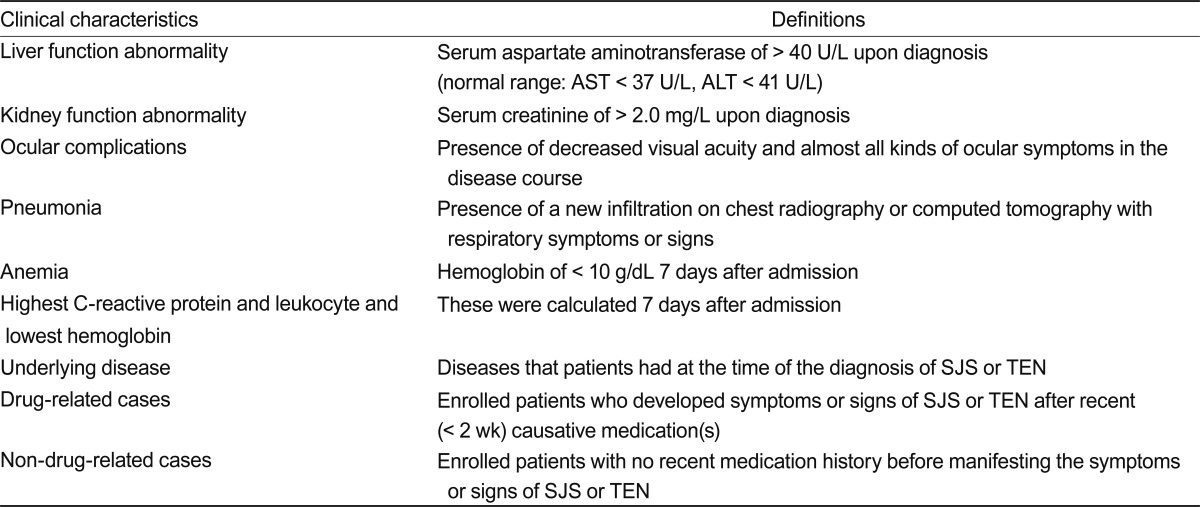
Definitions of clinical characteristics that were investigated
Statistics
The variables that were expected to be related to the prognosis were tested via a chi-square test between the non-drug-related and drug-related SJS/TEN patients. The data were analyzed using the SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). A value of p < 0.05 was considered statistically significant. The prognostic factors for survival were analyzed via Fisher's exact test and multivariate logistic-regression analysis with odds ratios (ORs) and 95% confidence intervals (CIs).
RESULTS
Demographic factors and clinical characteristics
A total of 82 consecutive patients were hospitalized for SJS or TEN. The demographics, presenting symptoms, and extent of mucocutaneous involvement during the study period were reviewed. Women were more frequently affected than men (45, 54.9% vs. 37, 45.1%, respectively). The mean age at initial presentation was 53.8 years (range, 18 to 94). The admission duration was 2-109 days (average, 20.2). A total of 71 patients (86.6%) were classified as having SJS, and the other 11 patients (13.4%) were classified as having TEN. Mucous membrane involvement was seen in the mouth (70, 85.4%), eye (49, 59.8%), genital area (27, 32.9%), nasal cavity (3, 3.6%), pharynx or tonsil (2, 2.4%), and larynx (1, 1.2%). A total of 49 patients (59.8%) had a fever of > 38℃ as an initial presenting symptom, and 34 patients (41.5%) complained of pain in the affected areas. Internal organ involvement comprised liver function abnormality (40, 48.8%) and kidney function abnormality (14, 17.1%).
Laboratory tests and medical comorbidities
A total of 45 (54.9%) patients had leukocytosis (> 10,000/mL), 49 patients (59.8%) had anemia, and 21 patients (25.6%) had neutropenia (absolute neutrophil count of < 4,000/mL). The C-reactive protein (CRP) level was 0.2 to 42.1 mg/dL (average, 8.75), the white blood cell count was 3,000 to 46,460/mL (average, 11,212), and the hemoglobin level was 3.8 to 15.1 g/dL (average, 11.2). Thirty-nine patients (47.6%) had underlying disease, including diabetes mellitus. Twelve patients (14.6%) had diabetes mellitus only, and three patients (3.6%) had other underlying disease with diabetes mellitus. Other underlying diseases included chronic renal failure, malignancy, liver cirrhosis, gout, human immunodeficiency virus infection, iatrogenic Cushing's syndrome, and miliary tuberculosis. One patient had multiple underlying diseases. Twelve patients had a medication history of anticonvulsants, and three patients (3.7%) had epilepsy. Cerebral hemorrhage, cerebral infarction, metastatic brain tumor, cerebral palsy, trigeminal neuralgia, hand tremor, anxiety disorder, headache, and back pain were each present in one patient, respectively.
Causative drugs
In 43 (52.4%) of the patients with SJS or TEN, the disease was related to drug administration. The most common drugs that triggered SJS or TEN were anticonvulsants (12/82, 14.6%), antibiotics (9/82, 11%), nonsteroidal anti-inflammatory drugs (NSAIDs) (5/82, 6.1%), herbal remedies (5/82, 6.1%), allopurinol (2/82, 2.4%), and antipsychotic drugs (1/82, 1.2%). Proton pump inhibitors, famciclovir, L-cysteine, and hair dye were among the etiologies in the patients. The most important causative drug was carbamazepine (7/82, 8.5%). In all patients, the administration of the causative or suspicious drug was discontinued after the diagnosis of SJS or TEN. Table 2 shows the causative drugs for the 82 patients.

Causes of Stevens-Johnson syndrome and toxic epidermal necrolysis
Difference between non-drug-related and drug-induced SJS or TEN
Anemia (p = 0.017), Crp level of ≥ 5 mg/dL (p = 0.026), and underlying disease (p = 0.001) were more common in the drug-related cases. Intravenous (IV) steroid use (p = 0.02) was more common in non-drug-related cases. Age of > 60 years, TEN, liver function abnormality, kidney function abnormality, and diabetes mellitus were much more frequently associated with the drug-related cases, but this was not statistically significant. Table 3 shows the results of the univariate analysis that was conducted for the clinical characteristics between the drug-related and non-drug-related SJS and TEN cases.
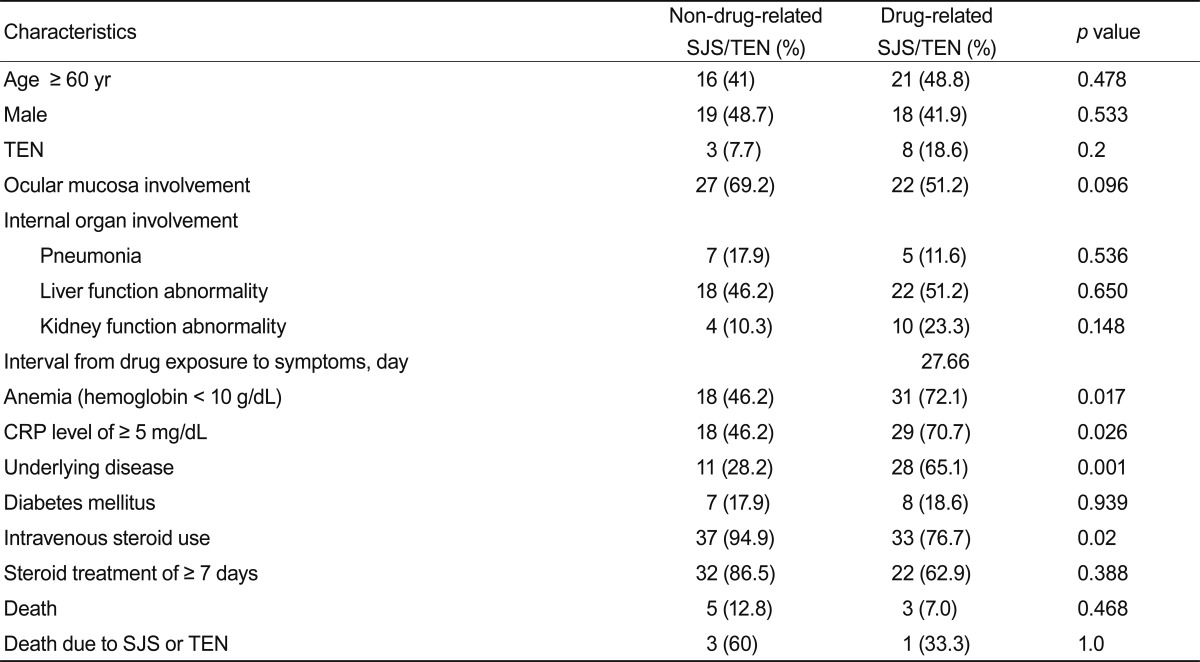
Results of univariate analysis of the clinical characteristics of drug-related (n = 43) and non-drug-related (n = 39) SJS and TEN cases
Differences between patients with SJS and TEN
Skin pain (p = 0.045), underlying disease (p = 0.002), and diabetes mellitus (p = 0.025) were more common in patients with TEN. Age of > 60 years, fever of > 38℃, pneumonia, kidney function abnormality, septic shock, leukocytosis of > 15,000/mm3, anemia, CRP of > 5 mg/dL, drug-related cases, and death were frequent in patients with TEN, but did not reach statistical significance. Table 4 shows the results of the univariate analysis that was conducted to compare the clinical characteristics between the SJS and TEN cases.
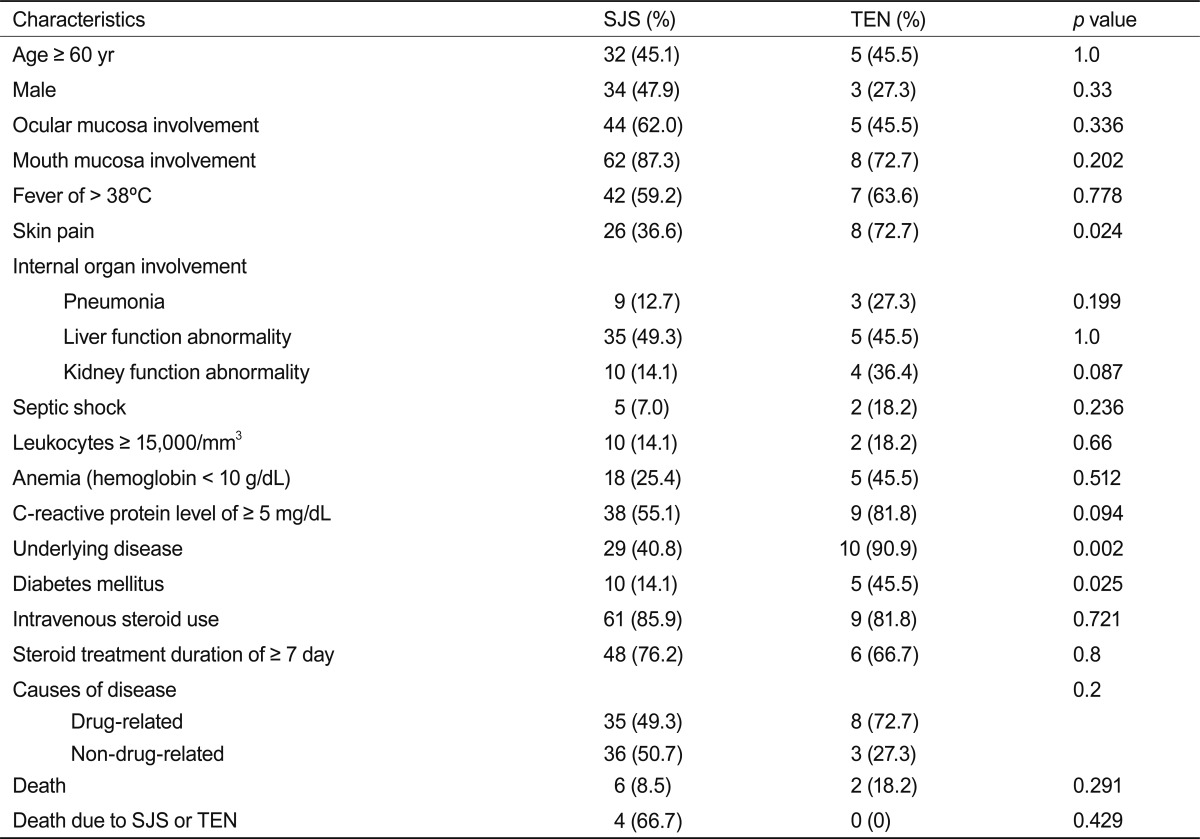
Comparison of univariate analysis of the clinical characteristics of SJS (n = 71) and TEN (n = 11) cases
Treatment regimens and outcomes
Seventy patients (85.4%) were treated with IV steroids, and the most common agent was dexamethasone (52, 63.4%). The initial steroid dose was 10 mg once daily. Peroral (PO) steroids in 42 patients (51.1%), along with prednisolone, was the most common treatment regimen (24, 29.3%), and the dose was 15 mg once daily. The interval from symptom onset to treatment with IV steroids was 2.21 days (range, 1 to 15), and the total period for IV and PO steroid use was 12.68 days (range, 1 to 68). Topical steroid ointments or lotions were used in 67 patients (81.7%). There were no complications from the steroid treatment. Intravenous immunoglobulin (IVIG) treatment was applied in only one patient. Eight patients (9.8%) died, and the cause of death in four was SJS or TEN itself. The follow-up duration was 2-2,193 days (average, 209.3). The results of the univariate analysis that was conducted to predict mortality showed statistical significance for the following: kidney function abnormality (OR, 24.75; p < 0.001), pneumonia (OR, 34.00; p < 0.001), hemoglobin of < 10 g/dL (OR, 25.38; p < 0.001), and combined underlying diseases (OR, 9.19; p = 0.017). In the multivariate logistic regression analysis, only pneumonia was found to be statistically significant as the cause of death (OR, 25.79; p = 0.009). The etiologies and clinical characteristics, such as age or sex, did not show a correlation with the prognosis. These results are summarized in Tables 5 and 6.
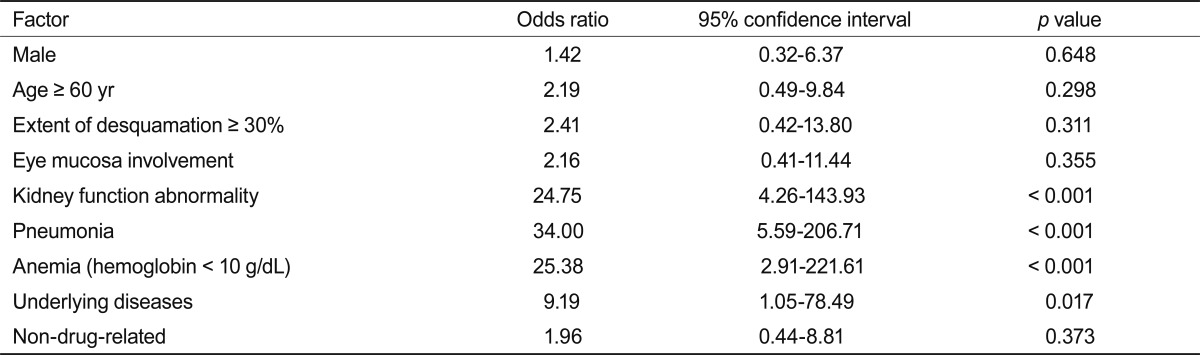
Results of univariate analysis for the prediction of death for 82 patients with Stevens-Johnson syndrome and toxic epidermal necrolysis

Multivariate logistic regression analysis for the prediction of death for 82 patients with Stevens-Johnson syndrome or toxic epidermal necrolysis
Ocular complications
Ten patients (12.2%) had ocular complications. The initial symptoms included ocular discharge (35, 42.7%), decreased vision (17, 20.7%), xerophthalmia (20, 24.4%), ocular pain (23, 28%), and photophobia (2, 2.4%). An ocular pseudomembrane was found in four patients, and corneal injury was found in two patients. Ocular edema and epithelial defects, superficial keratitis, symblepharon, and corneal infiltration were also found. Late ocular complications were seen in 8 patients (9.8%), but were not seen in 71 patients (80.7%). In nine patients, whether ocular complications occurred was unknown.
DISCUSSION
SJS and TEN are rare diseases (two cases/million population/year), but have significant impacts on public health because of their high mortality rates (20-25%) and complications, such as persistent corneal opacity, skin pigmentation, and skin scarring [2,12].
In a previous study that evaluated 207 patients with erythema multiforme (EM), SJS, or TEN, the most frequent cause of these ailments was found to be drugs [13]. Another study found that only 1 (3.1%) of 32 patients with SJS or TEN was a non-drug-related case [14]. In the present study, drug-related cases were common (43, 52.4%) but so were non-drug-related cases (39, 47.6%). All non-drug-related patients complained of various constitutional symptoms, such as fever, chills, myalgia, or sore throat, and the important and inevitable inclusion criteria were the symptoms preceding the drug that was prescribed to reduce such symptoms or not having a drug history. Non-drug-related or post-upper respiratory tract infection-related SJS or TEN may be more common clinically, but patients or doctors usually ignore its constitutional symptoms and do not pay attention to the drugs that may have caused it. To clarify the precise etiologies of SJS or TEN, and to prevent mistakes related to such, careful attention must be paid to patient history and medical history.
The most common triggering drugs in this study were anticonvulsants (carbamazepine) and antibiotics (cephalosporins). NSAIDs showed a lower risk in this study than in a previous study [2]. The so-called EuroSCAR study reported similar results, where the high-risk drugs included carbamazepine, cotrimoxazole, nevirapine, phenobarbital, phenytoin, and lamotrigine, whereas NSAIDs showed a lower risk [15]. Jeung et al. [16] studied 11 patients with drug rash with eosinophilia and systemic symptoms syndrome and 20 patients with SJS. The most common causative agents in both diseases were antibiotics, followed by anticonvulsants. Anticonvulsants and antibiotics are traditionally the drugs that are highly suspected of causing SJS or TEN, along with NSAIDs and allopurinol. The use of such drugs as first-line therapies should be carefully considered, especially when a safer alternative treatment modality exists.
In the present study, drug-related cases showed a frequently severe clinical course in contrast to the non-drug-related cases, consistent with previous findings [17]. The non-drug-related patients represented a large part of the etiologies, and patient hesitation to accept hospital visits or to acknowledge vague symptoms may have contributed to the delay in early diagnosis. Physicians should suspect early-phase SJS or TEN in patients with a short febrile history as well as sore throat and chills, although without a drug history.
SJS-related mortalities in previous studies have amounted to 0-10% of all mortalities, and TEN-related mortalities have amounted to 25-27% of all mortalities [10,18-22]. Optimal medical treatment for SJS and TEN requires early diagnosis, immediate discontinuation of the administration of the causative drug(s), provision of supportive care, and specific therapy [23]. The role of corticosteroids in the treatment of SJS is controversial. Some investigators have reported that corticosteroids may promote infectious complications and may lead to a poorer prognosis [24]. However, in recent years, steroid pulse therapy (e.g., with dexamethasone) in the acute stage of SJS/TEN has been proposed [25]. In that study, mortality of such patients was not higher and the time to re-epithelialization was not longer than expected, although small numbers of patients did not reach statistical significance. A small series of five patients from Japan suggested that early steroid pulse therapy may help to prevent ocular complications [26]. In the EuroSCAR-study, which evaluated 281 patients with SJS/TEN from France and Germany, mortality was chosen as the end point and linked to treatment with corticosteroids, IVIG, the combination of both, and supportive care only. ORs were calculated, and they suggested a benefit for treatment with corticosteroids but not for treatment with IVIG. Although such a retrospective analysis has some pitfalls, two major conclusions could be drawn: first, IVIG is not the best treatment for SJS/TEN and cannot generally be recommended; second, a controlled therapeutic trial using corticosteroids should be undertaken [9]. IVIG, which had been reported as an effective treatment for TEN based on the hypothesis that antibodies in pooled human IVIG block the Fas-mediated necrosis of keratinocytes in vitro, is still controversial. Other studies have shown that IVIG does not have an overall positive effect [27]. Two further studies undertaken in North American burn units suggested that IVIG does not improve the outcome of patients with TEN [28,29]. In the present study, IV steroids were used in most of the patients, and the mortality rate (9.8%) was lower compared to that of previous studies. Further well-designed studies are required to compare the effects and hazards of treatment modalities for SJS or TEN.
The SCORTEN was developed by Bastuji-Garin et al. [8] and can be used to predict the mortality risk based on seven independent risk factors (age of ≥ 40 years, heart rate of ≥ 120/min, history of malignancy, total body surface area detached > 10%, serum urea nitrogen of > 10 mmol/L, serum bicarbonate of < 20 mmol/L, and serum glucose of > 14 mmol/L). In the present study, kidney function abnormality, pneumonia, low hemoglobin (< 10 g/dL), and underlying diseases showed a significant negative correlation with survival in the univariate analysis. Only pneumonia, however, was shown to be a negative prognostic factor in the multivariate logistic regression analysis.
Ocular involvement is common in SJS and TEN [17]. In a previous study, 70% of the patients manifested ocular involvement and the common signs and symptoms were conjunctivitis, exudates, photophobia, and cicatrizing changes [17]. In contrast, less ocular involvement was found in the present study.
The limitations of this study include the fact that the causative agents were determined by history and did not depend on immunologic tests, and the treatment patterns differed among patients.
SJS and TEN have traditionally been known as drug-related systemic immune reactions. However, a definitive treatment regimen among the various supportive therapies that have been tried has not been established. In this study, the etiologies and clinical characteristics of non-drug-related and drug-related groups were reviewed. Only pneumonia was found to be a statistically significant negative prognostic factor. The overall mortality of the present study was lower than in previous studies, which may stem from the fact that steroid treatment was a major regimen in the present study. Hence, our results suggest that early steroid therapy should be performed along with other supportive management measures as well as careful documentation of patient history for vague constitutional symptoms and upper respiratory tract infection.
Notes
No potential conflict of interest relevant to this article was reported.