Ischemic monomelic neuropathy: a rare complication after vascular access formation
Article information
To the Editor,
Patients with end-stage renal disease require an arteriovenous fistula (AVF). Although an AVF has numerous advantages, it can result in neurological or ischemic problems with hemodynamic disturbance. In 1983, Wilbourn et al. [1] described ischemic monomelic neuropathy (IMN), defined as a type of multiple axonal-loss mononeuropathy distally in a limb, resulting from an impaired blood supply after graft insertion. IMN is a very rare complication, but requires an early diagnosis and treatment.
We report a case of IMN after an AVF operation and the results of a literature review.
A 44-year-old woman visited a vascular surgeon for hemodialysis access. She had been diagnosed with type 2 diabetes 15 years previously. She had a 3-year history of hypertension and chronic kidney disease and was a hepatitis B virus carrier. Laboratory studies showed a white blood cell count of 5,600/mL, hemoglobin of 9.1 g/dL, blood urea nitrogen (BUN) of 49.3 mg/dL, and serum creatinine of 7.6 mg/dL. The patient had outpatient surgery with a brachiocephalic graft on the left elbow.
The patient was admitted 7 days af ter the operation for weight gain, dyspnea, and general weakness. At that time, the hemoglobin was 8.2 g/dL, BUN 93.3 mg/dL, and serum creatinine 17.6 mg/dL. Metabolic acidosis was noted and a chest X-ray showed mild pulmonary congestion. The patient underwent emergency hemodialysis via a jugular vein catheter. After her uremia improved, she complained of swelling and numbness of the left hand and reduced grip strength. On examination, the fistula was patent and her radial pulse was palpable. The movement of the thumb was weak and she could not move her other fingers. She had no sensation in any modality.
Nerve conduction studies performed 3 weeks postoperatively showed a decreased nerve conduction velocity and amplitude for the motor and sensory parts of the left hand (Table 1). Both lower legs had markedly decreased motor and sensory function, compatible with a diabetic patient. We diagnosed IMN of the left hand and peripheral polyneuropathy of both legs.
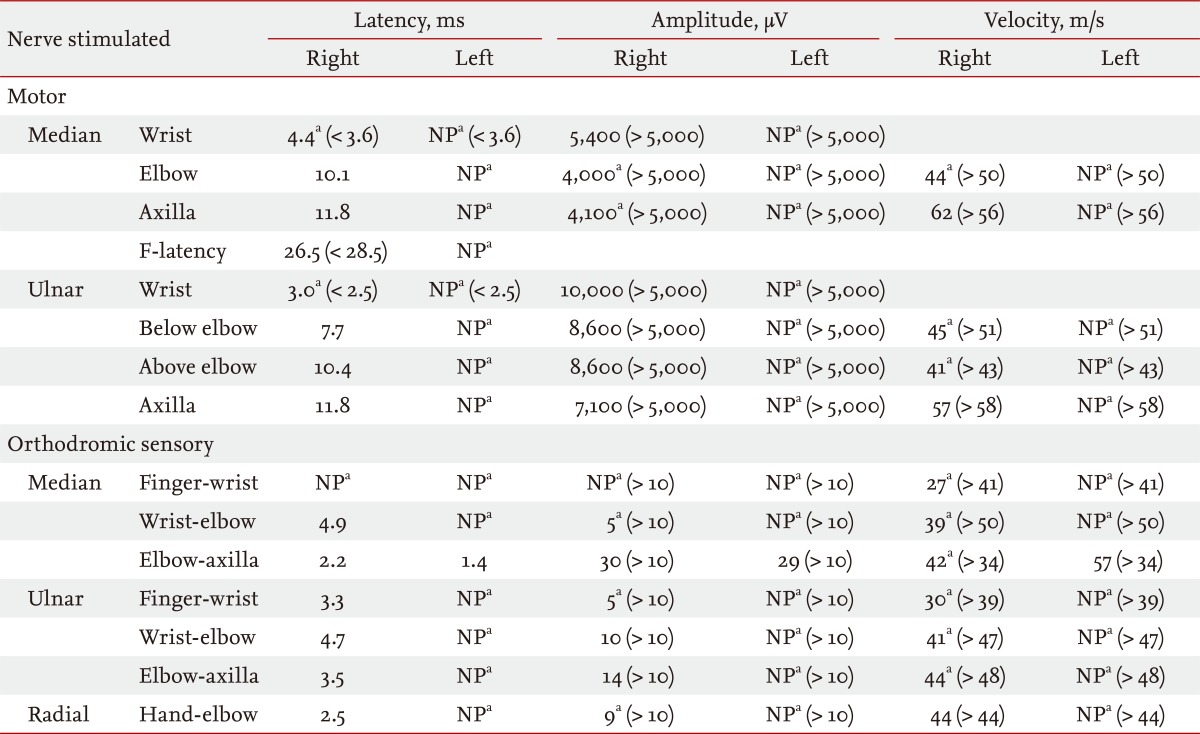
Nerve conduction study of upper extremities: initially
Although she required fistula ligation, we and the surgeon decided to observe her because 1 month had already passed since the first operation and an extra ligation would require another operation for access. Her diabetic polyneuropathy was treated with pregabalin.
After 2 months, she could grip a pencil. A follow-up nerve conduction test revealed improvement in the ulnar nerve, although defects remained in the median nerve (Table 2). She did not want to undergo more surgery. So we continued to observe her as an outpatient.

Nerve conduction study of upper extremities: after 2 months
IMN is a sensory/motor impairment without tissue necrosis, but with a transient reduction in blood flow. IMN is a form of steal phenomenon as the access surgery steals blood flow from distal nerve tissue [2], causing multiple axonal-loss mononeuropathy distally in the limb. IMN is often under-recognized and misdiagnosed, but its known incidence is 0.5% to 3.0% [3].
If a patient on hemodialysis complains of hand pain, physicians need to consider many diseases, including soft tissue swelling, wound hematoma, carpal tunnel syndrome, vascular steal syndrome, and IMN [4]. The most important factor in diagnosing IMN is that of the clinical manifestations. Acute pain, weakness, and muscle paralysis immediately after an operation are common symptoms. Since these symptoms are nonspecific, after AVF formation, the motor or sensory function of the operated hand should be checked and nerve conduction studies should be done. Low amplitudes and reduced or even undetectable motor or sensory nerve conduction velocities are compatible with IMN. Axonal loss of the median, radial, and ulnar nerves can also be observed [3]. Electromyograms show denervation, including fibrillation potentials and motor unit loss.
Since past neuropathy can be assumed to lower the ischemic injury threshold, diabetes, atherosclerotic disease, and women have an increased risk of IMN [2,4,5]. Nevertheless, IMN has been reported for a patient with no risk factors. In addition, a brachiocephalic fistula is commonly associated with this complication because the brachial artery is the only blood supply to the distal arm.
The most important treatment for IMN is immediate closure of the access; this increases the probability of recovery [3,4]. Early closure of the fistula leads to partial or full restoration of the sensory and motor function [5]. Some clinicians reported treatment using a banding operation [3]. Redfern and Zimmerman [5] reported an improvement in two patients under observation, like our case. However, it is not clear whether those patients had IMN [5]. Anticonvulsants, antidepressants, and narcotics have been used for pain control [2].
Better education and awareness on the part of the surgeon and nephrologist should lead to an early diagnosis and the proper management of IMN [4]. Therefore, we report this case of IMN after an AVF operation with a literature review.
Notes
No potential conflict of interest relevant to this article is reported.