A duodenal lipoma with a long stalk
Article information
57-year-old female patient presented with intermittent, progressive upper abdominal pain of 6-month duration. The physical examination was unremarkable. A duodenal polypoid lesion with a long stalk was seen at esophagogastroduodenoscopy (Fig. 1A). Routine laboratory tests were normal. We performed endoscopic ultrasound (EUS) to characterize the lesion, which appeared as a heterogeneously hyperechoic lesion originating from the third layers (Fig. 1B). Using EUS, the patient was diagnosed as having a duodenal lipoma. Using an electrocautery snare, we transected the upper third of the polypoid lesion to unroof it. This showed fat, consistent with the EUS finding (Fig. 1C). The histopathology of the excised specimen confirmed the diagnosis of lipoma. Her abdominal pain eventually subsided after endoscopic treatment.
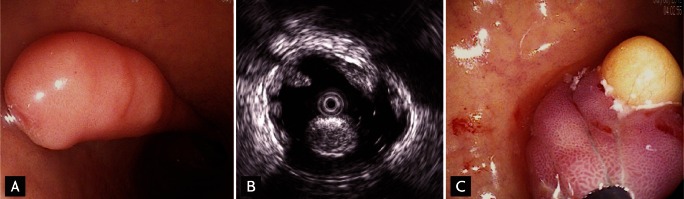
A duodenal lipoma with a long stalk confirmed using endoscopic ultrasound and an unroofing technique. (A) Duodenal polypoid lesion with a long pedicle is seen. (B) Hyperechoic lesion located on the third layer is found. (C) Fat is shown after unroofing technique.
Duodenal lipomas are rare, with fewer than 230 reported cases. Most are detected after bleeding or obstruction. EUS is an effective modality for diagnosing duodenal lipoma. On EUS, the typical duodenal lipoma is an intensive homogeneous hyperechoic lesion originating from the submucosa, with echo attenuation behind or inside the rear area. The unroofing technique cutoff only the upper half of the lipoma, and the remaining adipose tissue was rapidly and completely extruded from the open surface. This simple technique allows both histological confirmation and complete treatment with minimal risk of perforation.
Notes
No potential conflict of interest relevant to this article is reported.