Recent advances in treatment of aplastic anemia
Article information
Abstract
Recent advances in the treatment of aplastic anemia (AA) made most of patients to expect to achieve a long-term survival. Allogeneic stem cell transplantation (SCT) from HLA-matched sibling donor (MSD-SCT) is a preferred first-line treatment option for younger patients with severe or very severe AA, whereas immunosuppressive treatment (IST) is an alternative option for others. Horse anti-thymocyte globuline (ATG) with cyclosporin A (CsA) had been a standard IST regimen with acceptable response rate. Recently, horse ATG had been not available and replaced with rabbit ATG in most countries. Subsequently, recent comparative studies showed that the outcomes of patients who received rabbit ATG/CsA were similar or inferior compared to those who received horse ATG/CsA. Therefore, further studies to improve the outcomes of IST, including additional eltrombopag, are necessary. On the other hand, the upper age limit of patients who are able to receive MSD-SCT as first-line treatment is a current issue because of favorable outcomes of MSD-SCT of older patients using fludarabine-based conditioning. In addition, further studies to improve the outcomes of patients who receive allogeneic SCT from alternative donors are needed. In this review, current issues and the newly emerging trends that may improve their outcomes in near futures will be discussed focusing the management of patients with AA.
INTRODUCTION
Aplastic anemia (AA) is an clinical syndrome characterized by fatty replacement and decreased hematopoietic precursors of the bone marrow (BM), which results in peripheral blood (PB) pancytopenia [1]. It has been suggested that immune-mediated destruction of hematopoietic stem cells by activated cytotoxic T-cells expressing inhibitory cytokines such as interferon-γ and tumor necrosis factor-α contribute to its occurrence [2]. These cytokines induces death of hematopoietic stem cells, at least partially through the Fas-dependent pathway of apoptosis [3]. The mechanism of activation of cytotoxic T-cells is unclear, but several potential factors which are associated with antigen recognition, susceptibility of immune response, and secretion of cytokines are found [4]. The annual incidence of AA is estimated to be 2 per 1,000,000 persons per year in Western countries [5,6], but it is relatively higher in the Far East with 4 to 7 per 1,000,000 persons per year [7,8,9]. When patients are diagnosed with AA, careful investigations to exclude other possible cause of pancytopenia with hypocellular BM, including hypocellular myelodysplastic syndrome, paroxysmal nocturnal hemoglobinuria, and late onset inherited BM failure disorders, are needed [10]. For their therapeutic decision making, disease has been stratified to moderate, severe, and very severe AA based on the degree of pancytopenia and BM hypocellularity [11].
Four decades ago, when there were only a few effective treatment options, patients with severe or very severe aplastic anemia (SAA) died 1 to 2 years after diagnosis due to fatal infections and/or hemorrhagic complications. However, recent treatment options including allogeneic stem cell transplantation (SCT) and immunosuppressive treatment (IST), mainly anti-thymocyte globuline (ATG) with cyclosporin A (CsA), have helped them to expect a long-term survival [12]. Nevertheless, there are still many challenges in management of patients with AA; approximately half of patients fail to achieve hematologic response and experience relapse or clonal evolution associated with myelodysplasia and leukemia after IST. On the other hand, a substantial proportion of patients who need MSD-SCT, especially those who experienced failure to a first-line IST, are not able to receive transplantation due to donor unavailability or significant comorbidities. In addition, graft failure and serious complications including graft-vs-host disease (GVHD) and fatal infections after allogeneic SCT limit its more relevant applications [12]. In this review, current issues and the newly emerging trends that may improve their outcomes in near futures will be discussed focusing the management of patients with AA.
CURRENT TREATMENT SCHEME IN PATIENTS WITH SAA
Based on recent reports for the management of patients with SAA, a treatment algorithm is represented with Fig. 1. Allogeneic SCT from HLA-matched sibling donor (MSD-SCT) is the most preferred first-line treatment option for younger (≤ 50 years) SAA patients with a suitable donor and no significant comorbidities. Other patients can receive IST with ATG/CsA as their initial treatment. Allogeneic SCT from available HLA-matched donor should be considered as a salvage treatment in patients who fail to achieve response to first-line IST. If they cannot receive it, appropriate alternative treatment options, including novel IST regimen, allogeneic SCT from familial mismatched donor (FMD-SCT), androgen, and supportive care, should be offered according to their individual circumstances.
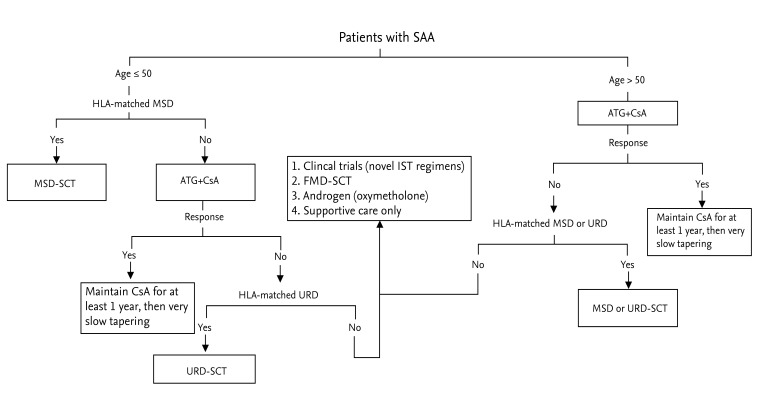
Treatment algorithm based on recent reports for the management of patients with severe aplastic anemia (SAA). MSD, matched sibling donor; URD, unrelated donor; ATG, anti-thymocyte globuline; CsA, cyclosporine A; FMD, familial mismatched donor; SCT, stem cell transplantation.
IMMUNOSUPPRESSIVE TREAMTENT
Historical aspect of IST for patients with AA: horse ATG/CsA as a standard IST regimen
Before allogeneic SCT and IST were relevantly used to the treatment of the patients with AA, high-dose androgen and/or supportive care including blood transfusion were the only available treatments, but their efficacy was observed in only a small proportion of patients [12]. Based on the recovery of autologous BM function after receiving horse ATG or allogeneic BM infusion with horse ATG conditioning [13,14], many investigators evaluated the efficacy of horse ATG alone for patients with AA and reported that a substantial proportion of patients could achieve hematologic response [15,16,17,18]. After Stryckmans et al. [19] reported the ability to induce hematological improvement of CsA, a phase III prospective study conducted by Frickhofen et al. [20] showed that patients who received IST using a combination of horse ATG and CsA achieved a higher overall response rate compared to those using horse ATG alone (70% vs. 46% at 6 months, p < 0.050). In addition, a subsequent report for long-term outcomes of this study showed a higher failure-free survival rate (39% vs. 24% at 11 years, p = 0.040) in the horse ATG/CsA group, but similar overall survival rate (58% vs. 54% at 11 years, p = 0.600) between the two groups because most nonresponders received salvage therapy [21]. Thereafter, other studies validated the efficacy horse ATG/CsA, which showed satisfactory results with overall response and overall survival rates of approximately 60% to 70% and 60 to 90%, respectively. Based on these reports, horse ATG/CsA has been accepted as a standard IST regimen for patients with AA [22,23,24].
Pretreatment factors predicting response and relapse rates of ATG/CsA for patients with AA
Although several studies showed acceptable outcomes of ATG/CsA, there were only limited reports for pretreatment factors predicting response and relapse rates of patients with AA who received it. A large retrospective study by the US National Institutes of Health (NIH) group to determine whether pretreatment blood counts can predict response rate for patients receiving horse ATG/CsA showed that younger age, higher absolute reticulocyte count (ARC) and absolute lymphocyte count (ALC) were associated with increased response rate. In this study, patients with higher ARC and ALC (≥ 25 × 109/L and ≥ 1 × 109/L, respectively) achieved a higher overall response rate compared to those with lower ARC and ALC (83% vs. 41%, p < 0.001) [25]. In other studies, patients with HLA-DR15, normal cytogenetics, and paroxysmal nocturnal hemoglobinuria clone had higher overall response rate and quality of response compared to those without [26,27,28].
On the other hand, Saracco et al. [29] compared the relapse rate between those who responded to horse ATG/CsA that received rapid (0.8 mg/kg/month) and slow CsA (≤ 0.7 mg/kg/month) tapering after maintaining stable blood counts lasting 3 or more months, and reported that was the relapse rate was higher in the rapid tapering group (60% vs. 8% at 10 years, p = 0.001). This study suggests that tapering CsA should be initiated after at least 1 year from treatment and taper carefully by 10% every month. Late relapse also can be observed in several long-term responders, which may have resulted from suboptimal therapeutic range of CsA by intolerability or poor compliance [30]. In addition, the NIH group reported that shorter telomere length of PB leukocytes at diagnosis was associated with higher relapse (odds ratio [OR] 0.16; 95% confidence interval [CI], 0.03 to 0.69; p = 0.010) and clonal evolution (OR, 0.29; 95% CI, 0.11 to 0.76; p = 0.010) rates with a lower overall survival (OR, 0.35; 95% CI, 0.17 to 0.73; p = 0.005) rate, but was not associated with overall response rate [31]. Conversely, Sakaguchi et al. [32] reported that pediatric patients with shorter telomere length of PB lymphocytes at diagnosis was associated with a lower overall response rate (OR, 22.0; 95% CI, 4.19 to 115; p < 0.001), but not relapse, clonal evolution, and overall survival rates. Considering these conflicting results, further large prospective studies to validate the relation between the outcomes of ATG/CsA and telomere length at diagnosis are needed.
The comparison of efficacy between patients with AA who received horse ATG/CsA and rabbit ATG/CsA as a first-line IST
Horse ATG/CsA had been used as a regimen of choice for first-line IST, whereas rabbit ATG/CsA has been used as a second-line regimen for patients with refractory or relapsed AA [30]. However, Lymphoglobulin (Sangstat, Lyon, France), which had once been the most widely used preparation of horse ATG, was withdrawn from the market in 2007 due to manufacturing difficulties. Thereafter, horse ATG has become unavailable and replaced with rabbit ATG in most countries.
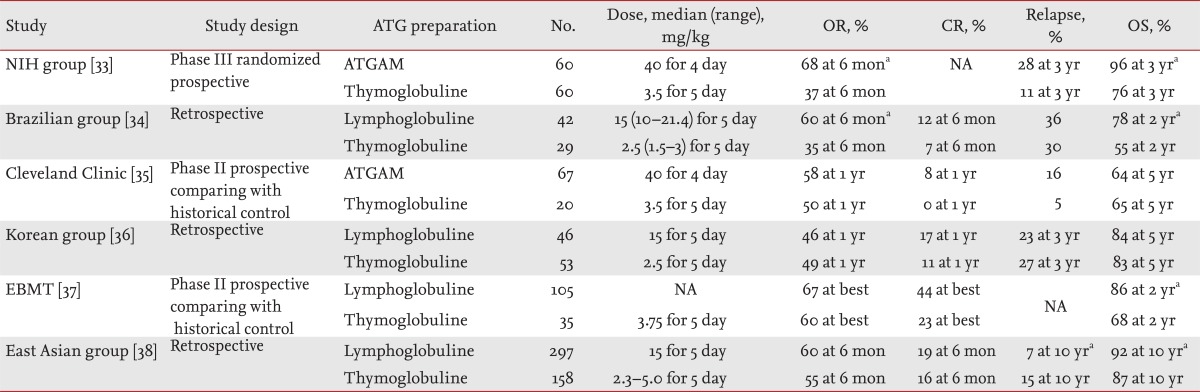
Until recently, there have been several studies comparing the outcomes of AA patients who received horse ATG/CsA and rabbit ATG/CsA as a first-line IST (Table 1). A phase III randomized prospective study conducted by the NIH group showed that the horse ATG/CsA group showed higher overall response (68% vs. 37% at 6 months, p < 0.010) and overall survival (96% vs. 76% at 3 years, p = 0.040) rates compared to the rabbit ATG/CsA group [33]. A retrospective study by Brazilian group also reported that horse ATG/CsA group showed higher overall response (60% vs. 35% at 6 months, p < 0.050) and overall survival (78% vs. 55% at 2 years, p = 0.030) rates [34]. However, a phase II prospective study comparing the historical horse ATG/CsA control group conducted by the Cleveland Clinic and a retrospective study by Korean group showed similar overall response (58% vs. 50% at 1 year, p = 0.610; and 46% vs. 49% at 1 year, p = 0.740, respectively) and overall survival (64% vs. 65% at 5 years, p = 0.540; and 84% vs. 83% at 5 year, p = 0.460, respectively) rates were observed between two groups [35,36]. On the other hand, another phase II prospective study comparing the historical horse ATG/CsA control group conducted by the European Group for Blood and Marrow Transplantation (EBMT) as well as a recent large pediatric retrospective study by East Asian Group, showed similar overall response (67% vs. 60%, p > 0.050; and 60% vs. 55% at 6 months, p = 1.000) rates, but the horse ATG/CsA group showed higher overall survival (86% vs. 68% at 2 years, p = 0.010; and 92% vs. 87%, p < 0.010, respectively) rates compared to the rabbit ATG/CsA group [37,38].
Comparative studies of horse ATG/CsA and rabbit ATG/CsA as a front-line IST in patients with AA
Compared to horse ATG, rabbit ATG evokes more prolonged and profound lymphocytopenia, which leads to a lower absolute number of CD4+ regulatory T-cells [33,36]. These findings can explain lower response and survival rates of the rabbit ATG/CsA group in several studies. However, it is suggested that discrepancies of other factors including the dose and duration of CsA administration and ethnic factors may result in conflicting results [1]. Notably, there has not been any study that showed superior outcomes of rabbit ATG/CsA over horse ATG/CsA. Therefore, horse ATG/CsA should be used preferentially as a first-line IST regimen and rabbit ATG/CsA should be considered only if horse ATG is unavailable.
Efforts to improve the outcomes of ATG/CsA by the addition of other agents
Because half of patients with AA experience failure to IST, there have been many efforts to improve its efficacy by adding other agents. However, prospective studies conducted by the NIH group failed to show that the addition of mycophenolate mofetil or silrolimus to horse ATG/CsA results in improved overall response rate and reduced relapse rate [39,40]. Meanwhile, a prospective study conducted by Teramura et al. [41] comparing the outcomes of patients who received horse ATG/CsA with or without granulocyte colony-stimulating factor (G-CSF) showed that patients who received G-CSF achieved higher overall response (77% vs. 57% at 4 years, p = 0.030) and lower relapse (15% vs. 42% at 4 years, p = 0.010) rates compared to those who did not, but there were no significant difference in overall survival rate (88% vs. 94% at 4 years, p = 0.440) and incidence of infectious complications (59% vs. 40%, p = 0.070). Conversely, similar overall response rate (73% vs. 66% at 6 years, p = 0.540) between the patients who received horse ATG/CsA with and without G-CSF was observed in another randomized study conducted by Tichelli et al. [42]. Because of conflicting results and insufficient data, many clinical centers have not included routine G-CSF administration with their IST protocol.
Eltrombopag, an oral form of nonpeptide thrombopoietin mimetic, was developed to induce platelet maturation and release by binding to thrombopoietin receptor (c-MPL) on megakaryocytes in patients with immune thrombocytopenic purpura [43]. However, a previous report, which showed that patients who lack c-MPL develop a form of congenital BM failure, suggested that thrombopoietin is critical to hematopoietic stem cell development and differentiation [44]. Based on this observation, a recent phase II prospective study was conducted to determine the eltrombopag can be effective for nonresponders to previous IST. In this study, 11 of 25 enrolled patients (44%) achieved hematological response in at least one-lineage and the normalization of BM tri-lineage hematopoiesis [45]. In its subsequent study, hematological response in at least one-lineage was observed in 17 of 43 enrolled patients (40%), including seven (16.3%) tri-lineage response. In addition, five patients (11.6%) who achieved sustained response maintained stable blood counts at a median 13 months (range, 1 to 15) after drug discontinuation [46]. These reports suggest that adding eltrombopag might improve the efficacy of horse ATG/CsA. A phase III randomized study to validate this hypothesis is currently ongoing (www.clinicaltrials.gov as #NCT01623167).
Salvage treatment for patients with AA refractory or relapsed to a first-line IST
Not only MSD-SCT but also allogeneic SCT from HLA-matched unrelated donor (URD-SCT) can be a considerable treatment option for SAA patients who failed to first-line IST. It is supported by a recent phase III prospective study conducted by Kosaka et al. [47], which showed a higher failure-free survival rate of pediatric patients who received URD-SCT compared to those who received horse ATG/CsA (84% vs. 10% at 5 years, p < 0.010) after experiencing failure to first-line IST. However, alternative treatment options, including an additional course of ATG/CsA or other IST regimens, also can be considered for patients who are ineligible for allogeneic SCT.
Studies for second course of ATG/CsA were not relatively abundant and reported a wide range of response rates. A phase II prospective multicenter study conducted by Di Bona et al. [48] reported that nonresponders to first-line horse ATG/CsA who received a second course rabbit ATG/CsA showed acceptable overall and complete response rates (70% and 30%, respectively). In addition, a retrospective study by the NIH group showed that overall response rates of a second course rabbit ATG/CsA at 6 months in patients who failed to achieve response or experienced relapse to first-line horse ATG/CsA were 30% and 65%, respectively [49]. However, a retrospective study by the NIH group showed that non-responders to first-line rabbit ATG/CsA who received a second course horse ATG/CsA achieved relatively poor overall response rate (21% at 3 months) [50]. Based on this result, It is not recommended second course of ATG/CSA in patients who failed achieve response to first-line rabbit ATG/CsA.
Alemtuzumab, which is a humanized anti-CD52 IgG1 monoclonal antibody with lymphocytopenic activity, or high-dose cyclophosphamide (CY) has been also used in patients with refractory or relapsed AA. A pilot study conducted by Risitano et al. [51] for 19 patients with AA (including 13 refractory) showed an overall response rate of 58% and complete response rate of 26% after receiving alemtuzumab (a total dose of 103 mg subcutaneously) and low-dose CsA. In addition, the NIH group investigated the role of alemtuzumab monotherapy (test dose of 1 mg followed by 10 mg/kg/day for 10 days) for patients with refractory or relapsed SAA, which showed overall response rates at 6 months of 37% and 56% with overall survival rates at 3 years of 83% and 86%, respectively [52]. In these studies, clinically significant infectious complications including cytomegalovirus reactivation and Epstein-Barr virus-related disease was not problematic. On the other hand, a recent report for long-term outcomes of CY (50 mg/kg for 4 days) in 23 patients with refractory AA showed feasible overall and complete response rates (47.8% and 21.7% at 10 years, respectively) with overall survival rate (61.8% at 10 years) [53]. However, CY for patients with AA should be used with caution because frequent fatal infectious complications followed by delayed neutrophil recovery in patients who received it as a first-line treatment were observed in a previous study [54].
ALLOGENEIC SCT FOR PATIENTS WITH SAA
Allogeneic MSD-SCT
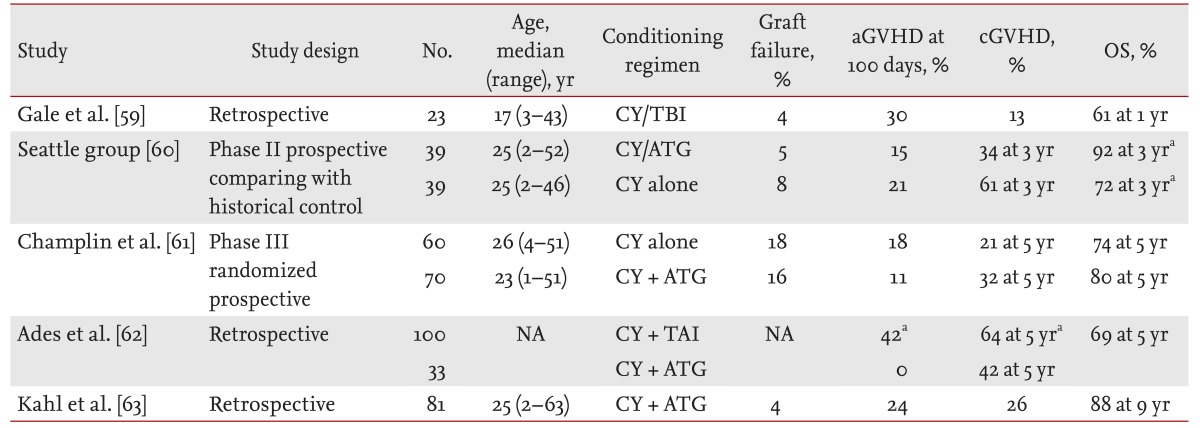
MSD-SCT is the most preferred treatment option for younger SAA patients with a suitable donor and no significant comorbidities. Until recently, many investigators have explored optimal conditioning regimen for SAA patients who receive MSD-SCT to achieve sustained engraftment with minimal fatal complications (Table 2). In the initial experiences of MSD-SCT using CY alone conditioning, high incidence of graft failure was a major challenge, particularly in previous heavily transfused patients [55]. Subsequently, MSD-SCT using radiation, including local-field and total-body irradiation (TBI), plus CY conditioning was attempted and resulted in a lower incidence of graft failure, but was associated with relatively higher incidences of long-term regimen-related morbidities and mortality [56,57,58,59]. Thereafter, several investigators attempted MSD-SCT using CY plus ATG conditioning, which might induce both effective immunoablation and lymphoablation [60,61,62,63]. In a phase II prospective study conducted by the Seattle group, the incidence of neutrophil engraftment, acute and chronic GVHD for patients who received MSD-SCT using CY (200 mg/kg) plus horse ATG (90 mg/kg) conditioning were 95%, 15%, and 34%, respectively. Their overall survival rate was significantly higher compared to that of historical control group who received CY alone conditioning (92% vs. 72% at 3 years, p = 0.043) [60]. In addition, a retrospective study by Ades et al. [62] comparing the outcomes of patients who received MSD-SCT using CY (200 mg/kg) plus rabbit ATG (10 mg/kg) conditioning and thoraco-abdominal irradiation (TAI, 600 cGy) plus CY (150 mg/kg) conditioning showed that the CY/ATG group was associated with a lower incidence of acute (0% vs. 42%, p < 0.001) and chronic GVHD (42% vs. 64%, p = 0.025) with higher overall survival rate (OR, 6.20; 95% CI, 1.50 to 25.90; p < 0.001) compared to the TAI/CY group.
Reports of outcomes in patients with SAA who received MSD-SCT
On the other hand, minimizing the incidence of GVHD is essential for SAA patients who receive allogeneic SCT, considering that they do not need its graft-versus-leukemia effect. A large registry-based study conducted by EBMT/Center for International Blood and Marrow Transplant Research (CIBMTR) comparing the outcomes of patients who received MSD-SCT using peripheral blood stem cells (PBSCs) and BM as a graft source showed that higher incidence of chronic GVHD (27% vs. 12%, p = 0.002) and lower overall survival rate (73% vs. 85% at 5 years, p = 0.024) were observed in the PBSC group compared to the BM group, especially in patients younger than 20 [64]. In addition, a phase III randomized study conducted by Gruppo Trapianto di Midollo Osseo/EBMT comparing the outcomes of patients who received MSD-SCT using CsA plus methotrexate (MTX) and CsA alone GVHD prophylaxis showed that the incidence of transplant-related mortality (3% vs. 15% at 1 year, p = 0.070) and overall survival rate (94% vs. 78% at 5 years, p = 0.050) were significantly superior in the CsA/MTX group compared to the CsA alone group [65]. Therefore, BM and CsA/MTX are widely used as the preferable stem cell source and GVHD prophylactic regimen for SAA patients who receive MSD-SCT.
On the other hand, the upper age limit of SAA patients who are able to receive MSD-SCT remains an unsolved challenge. In a large registry analysis conducted by CIBMTR, the impact of patients' age on transplant outcomes was analyzed. The incidence of neutrophil engraftment was not significantly different in all age groups, whereas patients older than 40 showed a significantly lower incidence of platelet engraftment compared to those younger than 20 (OR, 0.45; 95% CI, 0.25 to 0.83; p = 0.010), whereas not compared to those aged between 20 and 40 (OR, 0.60; 95% CI, 0.33 to 1.10; p = 0.098). The incidence of mortality for patients older than 40 was significantly higher compared to those of patients younger than 20 (OR, 2.70; 95% CI, 1.89 to 3.87; p < 0.001) and aged between 20 and 40 (OR, 1.60; 95% CI, 1.13 to 2.26; p = 0.008) [66]. This study showed that the incidence of mortality increased with age for patients who received MSD-SCT although it should be interpreted with caution because patients in this study cohort received heterogeneous conditioning regimens with mostly receiving CY (200 mg/kg) with or without ATG (71.4%). However, the difficulties of determining the most appropriate first-line treatment for older patients still remain because lower overall response and survival rates were also observed when they received IST [25].
On the other hand, a recent phase II prospective study conducted by EBMT which analyzed the outcomes of patients who received MSD-SCT using fludarabine (FLU, 120 mg/m2) plus CY (1,200 mg/m2) with rabbit ATG (15 mg/kg) showed that no significant difference in overall survival rate was observed between patients older than 40 and those aged between 30 and 40 [67]. We also reported the outcomes of 82 SAA patients who received MSD-SCT using FLU (180 mg/kg) plus CY (100 mg/kg) with rabbit ATG (10 mg/kg) conditioning. In this study, there was no significant difference in overall survival rate among patients with age lesser than 20, 20 to 39, 40 to 49 and 50 to 59 (88%, 97%, 92%, and 86% at 3 years, respectively, p = 0.426) [68]. Consequently, these reports suggest that FLU-based conditioning may be a promising option to overcome relatively poor outcomes of MSD-SCT in older patients. Therefore, MSD-SCT using FLU-based conditioning should be considered as a feasible first-line treatment for older patients.
Allogeneic URD-SCT
URD-SCT can be considered as a treatment option for SAA patients who failed first-line IST or require emergent allogeneic SCT if they have no suitable MSD. Two decades ago, only about one-third of patients who received URD-SCT experienced long-term survival [69]. Recently, however, relevant applications of high-resolution HLA typing for donor selection and more optimized conditioning regimen improved overall survival rate to approximately 70 to 80% [70,71,72,73,74].
The conditioning regimen for URD-SCT for SAA patients that could minimize the incidence of graft failure and regimen-related toxicities still remains uncertain. An initial phase II prospective study conducted by EBMT which analyzed the outcomes of patients who received URD-SCT using FLU (120 mg/m2) plus CY (1,200 mg/m2) with rabbit ATG (7.5 mg/kg) conditioning showed that the incidence of graft failure was 18% with an overall survival rate of 73% at 2 years. In this study, patients older than 14 showed a significantly higher incidence of graft failure (32% vs. 5%, p = 0.030) with a lower trend of overall survival rate (61% vs. 84% at 2 years, p = 0.200) [70], which suggested that the modification of conditioning was required. In addition, an EBMT registry-based analysis for the outcomes of patients who received URD-SCT using FLU (120 mg/m2) plus CY (1,200 mg/m2) with rabbit ATG (7.5 mg/kg) ± low-dose TBI (200 cGY) conditioning showed that there was no significant difference in overall survival rate between the patients older and younger than 27 when they received low-dose TBI containing regimen (78% vs. 79% at 5 years, p > 0.050). However, relatively high incidence of mortalities by graft failure (7%), posttransplant lymphoproliferative disease (4%) and GVHD (4%) of this study remained to be a challenge to overcome [71]. On the other hand, the Seattle group conducted a dose-escalating study to find the most appropriate TBI dose, when used with CY (200 mg/kg) plus horse ATG (120 mg/kg) conditioning. After escalating or de-escalating 200 cGy based on the development of graft failure or regimen-related toxicities from staring 600 cGy, they found that 200 cGy was the most effective dose in minimizing regimen-related toxicities without sacrificing sustained engraftment [72]. In addition, we conducted a prospective study of de-escalating TBI to find optimal dose, when used with CY (120 mg/kg), which showed higher overall survival rate in the 800 cGy group was observed compared to the 1,000 and 1,200 cGy groups (92% vs. 40% vs. 44% at 3 years, p < 0.001) [75]. In a subsequent report of the long-term results for patients who received URD-SCT using TBI (800 cGy) plus CY (120 mg/kg) conditioning, all enrolled patients achieved sustained myeloid engraftment after a median of 13 days (range, 8 to 30) with acceptable incidences of acute and chronic GVHD (46% and 50%, respectively) and overall survival rate (88% at 5 years) [76]. The current available reports of outcomes for SAA patients who received URD-SCT are summarized in Table 3.
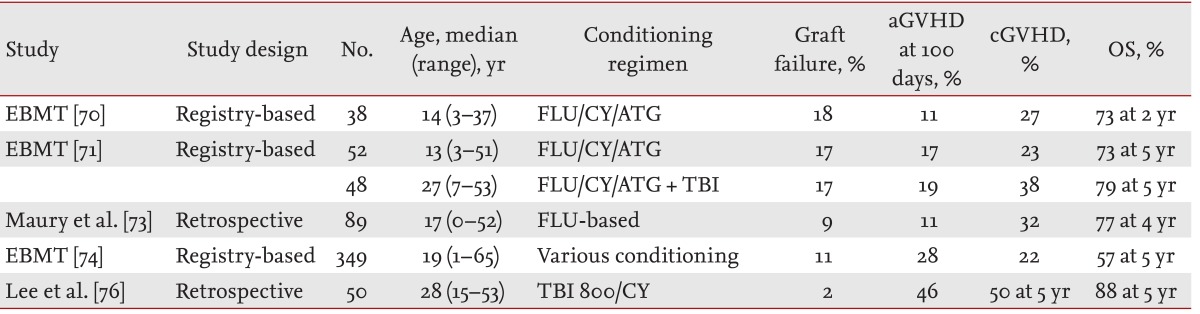
Large-study reports of outcomes in patients with SAA who received URD-SCT
Because patients who received URD-SCT experience more frequent and severe GVHD compared to those who received MSD-SCT [77], more effective GVHD prophylaxis, especially for SAA patients, is needed. A matched-pair analysis based on the Japan Marrow Donor Program registry comparing the outcomes of patients who received URD-SCT using GVHD prophylaxis with FK506 and CsA along with MTX showed that the FK506/MTX group showed a higher overall survival rate (83% vs. 50% at 5 years, p = 0.012) with a lower trend for incidence of chronic GVHD (13% vs. 36%, p = 0.104) [78]. On the other hand, several patients unavoidably receive URD-SCT using PBSC as stem cells source and/or from partially HLA-URD. Because they are associated with a higher incidence of GVHD or lower survival rate [76,79], we conducted a phase II prospective study of adding low-dose rabbit ATG (2.5 mg/kg) to TBI (800 cGy) plus CY (120 mg/kg) conditioning in patients who received URD-SCT from these donors and compared the historical control group who did not receive additional low-dose rabbit ATG. In this study, the incidence of acute GVHD was significantly decreased (21% vs. 64%, p = 0.028), but not chronic GVHD (31% vs. 57%, p = 0.247) in patients who received low-dose rabbit ATG compared to the historical control group [80]. However, further studies are needed to determine whether this strategy is effective for SAA patients.
Allogeneic FMD-SCT
FMD-SCT had been considered a treatment option for patients with aggressive hematologic malignancies and lacking HLA-matched donors. Although there are several advantages including universal donor availability without delay, high incidences of graft failure and GVHD due to bidirectional barrier of HLA incompatibilities have been considered as a great concern [81,82]. However, recent advances in controlling these challenges extended its application to patients with less aggressive diseases, including SAA.
Until recently, several investigators have attempted to search optimal conditioning regimen and strategy of graft manipulations for SAA patients who receive FMD-SCT. An initial retrospective study by the Seattle group showed that patients who received unmanipulated FMD-SCT using more intensified conditioning consisted of TBI (1,200 cGy) and CY (120 mg/kg) achieved a higher incidence of sustained engraftment (83% vs. 29%, p < 0.050) and overall survival rate (50% vs. 0%, p < 0.050) compared to those using CY alone (200 mg/kg) conditioning [83]. Another retrospective study by Tzeng et al. [84] showed that no graft failure was observed in six patients who received unmanipulated FMD-SCT using TBI (800 cGY) plus CY (200 mg/kg) conditioning. In a recent retrospective study by the Peking group for patients who received FMD-SCT, all patients achieved sustained engraftment by using intensified conditioning that consisted of CY (200 mg/kg) plus rabbit (2.5 mg/kg) or horse ATG (20 mg/kg) with intravenous busufulan (6.4 mg/kg) following G-CSF primed BM and mobilized PBSC infusion, with acceptable overall survival rate (65% at 2 years) and incidences of acute and chronic GVHD (42% and 56%, respectively) [85]. In addition, various novel strategies including using posttransplant CY and selective CD3+ T-cell depleted grafts have been also attempted to improve the outcomes of patients who receive FMD-SCT [86,87].
IRON CHELATION THEARPY FOR PATIENTS WITH AA
A substantial proportion of patients with AA unavoidably receive blood transfusions as supportive care after receiving available treatments. Long-term regular transfusion may lead to iron overload, which is associated with significant morbidities and mortality [88,89]. Deferasirox is an oral iron chelator, whose efficiency has been proven for patients with various transfusion-dependent hematological diseases [90,91]. A recent sub-group analysis for 116 patients with AA, conducted by Lee et al. [92], of a large phase II prospective study which evaluated its efficacy and safety showed that their serum ferritin level significantly decreased (3,254 to 1,854 ng/mL, p < 0.001) at 1 year after deferasirox without significant toxicities except mild renal toxicities. A subsequent post hoc analysis of this study showed hematologic improvement was observed in a subset of patients (46%) who received deferasirox without concomitant IST with a significant difference in serum ferritin level change from baseline between those who achieved response and those who did not (-46% vs. -28%, p = 0.017) [93]. Other investigators also reported that a substantial proportion of patients who received deferasirox achieved hematological improvement [94,95,96], but further investigations are required to determine which mechanism was involved.
CONCLUSIONS
Although recent advances have helped most AA patients to achieve long-term survival, there are many unsolved challenges in their appropriate management. About half of patients who received IST as a first-line treatment still experience failure. Therefore, further studies are needed to improve the response rate and reduce the incidence of relapse after IST, especially considering the unavailability of horse ATG in many countries. Eltrombopag may be a promising additional agent to improve the efficacy of IST, but further validations for its beneficial effects are needed. In addition, more effective treatment for patients who are ineligible for allogeneic SCT after experiencing failure to first-line IST should be explored.
On the other hand, the upper age limit of SAA patients who are able to receive MSD-SCT as a first-line treatment should be re-determined, considering the favorable outcomes of older patients who received MSD-SCT using FLU-based conditioning. It may contribute to determine the most appropriate treatment option for them along with further studies to investigate pretreatment factors predicting response and relapse after fist-line IST. In addition, more optimized conditioning and effective GVHD prophylaxis should be also developed to improve the outcomes of allogeneic SCT from alternative donors.
Notes
No potential conflict of interest relevant to this article was reported.