Metastatic sarcomatoid carcinoma presenting as a pedunculated mass on the floor of the mouth
Article information
To the Editor,
Sarcomatoid carcinoma is a biphasic malignant neoplasm demonstrating both carcinomatous and spindle cell components, the latter of which may exhibit epithelial features on immunohistochemical or ultrastructural analysis [1]. These uncommon neoplasms have been described using a variety of different names, including carcinosarcoma, mixed tumor, or carcinoma with sarcomatoid stroma, causing great uncertainty about their classification and histogenesis. They have been found to occur in many different anatomical locations, with head and neck, kidney, and lung being the most common sites [2]. While microscopic findings are often quite variable for this kind of carcinoma, evidence of a morphological transition zone between the carcinomatous and sarcomatous tissue, as well as distinct epithelial characteristics in the sarcomatous component as determined by electron microscopy or immunohistochemistry are considered distinctive features of these neoplasms; this has provided both helpful clues for pathological diagnosis and important insights into histogenesis [3]. Here, we describe a case of metastatic sarcomatoid carcinoma of the lung presenting as a pedunculated mass on the floor of the mouth.
A 62-year-old man presented to our clinic complaining of a sublingual mass and left shoulder pain for 3 months. Analysis of his medical history was noncontributory. On physical examination, a soft 3 × 4-cm pedunculated mass with a necrotic and ulcerated surface was identified on the floor of the mouth (Fig. 1A). The remainder of the clinical examination, including examinations of the patient's respiratory system, revealed no abnormalities. A chest radiograph revealed a 5-cm lobulated mass in the right upper lobe of the lung. A subsequent chest computed tomography scan revealed a 5 × 5-cm mass on the apical segment of the right lower lobe and hilar lymphadenopathy (Fig. 1B). Following diagnosis, the patient underwent a bronchoscopic biopsy to remove the mass, along with an incisional biopsy of the mass in the oral cavity. Morphologically, the excised masses were composed of pleomorphic spindled tumor cells resembling a malignant fibrous histiocytoma (Fig. 1C and 1D). By immunohistochemical staining, the malignant cells were diffusely strongly positive for vimentin and focally positive for cytokeratin (Fig 2). However, the malignant cells were negative for S-100 protein and HMB45. Following surgery, the patient received radiation therapy on the oral cavity, in addition to palliative chemotherapy; however, the response to these therapies was poor, and he died 4 months after diagnosis.
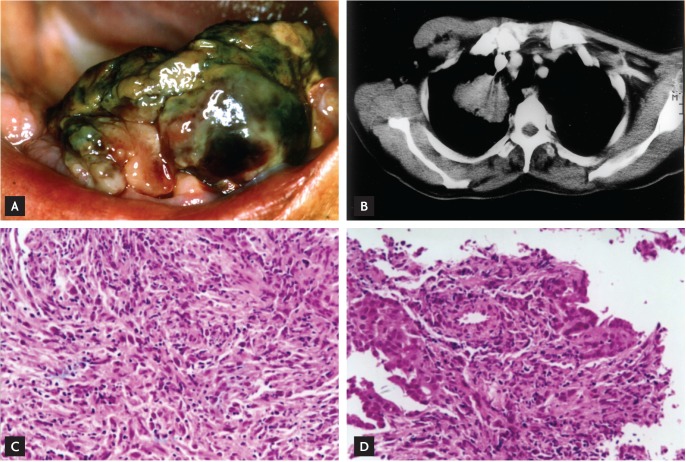
Clinical, imaging, and microscopic findings. (A) A soft 3 × 4-cm pedunculated mass with a necrotic and ulcerated surface on the floor of the mouth. (B) A 5 × 5-cm mass on the apical segment of the right lower lobe and hilar lymphadenopathy on chest computed tomography. (C, D) A storiform pattern of plump spindled cells characterized by cellular pleomorphisms with numerous mitotic figures (H&E, ×100) in masses excised from the floor of the mouth and lung.
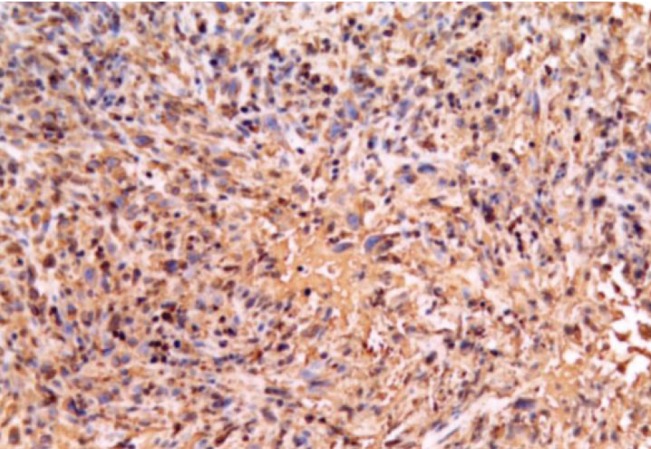
Vimentin immunostaining findings. Diffuse strong reaction in the sarcomatoid component and focal immunoreactivity for cytokeratin in spindled cells (×100).
Lung tumors in which a malignant mesenchymal component exists concurrently with a malignant epithelial component are uncommon. In this case, the sarcomatoid component presented with three major patterns: a malignant fibrous histiocytoma-like pattern, a fibrosarcomatous pattern, and an unclassified sarcomatous pattern [1]. In general, there was a mixture of spindle cell proliferation patterns, whereas our categorization was based on the predominant pattern. In cases with poor carcinomatous differentiation by light microscopy, such as this one, immunohistochemical staining is often used to establishing a diagnosis of sarcomatoid carcinoma [4]. The majority of sarcomatoid cells expressed abundant vimentin-positive intermediate filaments, compared with focal staining for cytokeratin. Analysis of mesenchymal differentiation using antibodies other than vimentin, such as actin, desmin, myosin, and S-100 protein, revealed no staining in the sarcomatous areas in any case [5].
Cases of pulmonary sarcomatoid carcinoma such as this one should be regarded as poorly differentiated carcinomas, as they tend to be more aggressive at the time of diagnosis and are also associated with a high metastatic rate. Accordingly, the prognosis of these patients is often poor, even after surgery, irradiation, and chemotherapy. Aggressive treatments, including preoperative chemoradiotherapy, combined with extensive resection and postoperative adjuvant therapy, may therefore be reasonable to prolong the life of pulmonary sarcomatoid carcinoma patients. This case was unique in that the first presentation of the disease was a pedunculated mass on the floor of the mouth in combination with a lung mass detected during work-up. As the histologic and immunohistochemical findings between the two masses were identical, it is reasonable to consider this a case of sarcomatoid carcinoma of the lung with metastasis.
Notes
Conflict of interest: No potential conflict of interest relevant to this article was reported.