Epidemiology of chronic thromboembolic pulmonary hypertension in Korea: results from the Korean registry
Article information
Abstract
Background/Aims:
The diagnosis of chronic thromboembolic pulmonary hypertension (CTEPH) is difficult for numerous reasons and is related with a poor prognosis. In Korea, the incidence of CTEPH and its clinical features are unknown. Thus, in this study, we evaluated the clinical characteristics and outcomes of CTEPH in a Korean cohort.
Methods:
This study included South Korean patients diagnosed with CTEPH between September 2008 and October 2011. Baseline characteristics, treatments and outcomes were analyzed.
Results:
A total of 134 patients were included in this study with 76 females (56.7%). Their median age was 58.3 ± 15.9 years and dyspnea (112 patients, 83.5%) was the most common presenting symptom. Sixty-three patients (47%) had a history of acute pulmonary embolism or deep vein thrombosis, and six (4.5%) had pulmonary tuberculosis. In total, 28 patients (21%) underwent pulmonary thromboendarterectomy (PTE), and 99 patients had medical therapy. During the study period, 18 patients (13.4%) died. In a multivariate analysis, higher hemoglobin (relative risk [RR], 1.516; 95% confidence interval [CI], 1.053 to 2.184; p = 0.025) and lower total cholesterol levels (RR, 0.982; 95% CI, 0.965 to 0.999; p = 0.037) were associated with increased mortality.
Conclusions:
This was the first national cohort study of Korean patients with CTEPH. Accurate diagnosis, characterization and distributions of CTEPH are imperative for prompt treatment in patients, particularly those undergoing PTE.
INTRODUCTION
Chronic thromboembolic pulmonary hypertension (CTEPH) is one of the leading causes of severe pulmonary hypertension (PH) and is associated with considerable mortality [1]. CTEPH results in overt thromboembolic PH and right heart failure; however, progress in surgical treatments over the past decade has considerably improved the prognosis for this condition [2,3].
Current data suggest the incidence of CTEPH is 3 to 30 per million [4]. The development of CTEPH is associated with pulmonary embolism (PE), certain chronic medical conditions, thrombophilia, and a genetic predisposition [5-8]. Nonspecific symptoms, an unremarkable physical examination, and a lack of physician awareness about the condition often complicates accurate diagnosis [2,9]. A recent study in the UK showed that CTEPH was diagnosed in 14% of cases referred to designated national PH centers [10]. These data suggest that CTEPH may be a more common condition than is currently recognized.
The incidence and clinical characteristics of CTEPH in Korea are unknown. The Korean Registry for Pulmonary Hypertension was initiated in 2008 with the aim of gaining more insight into the prevalence, therapy, and outcome of patients with PH in Korea. In this study, we evaluated the baseline characteristics and outcomes of CTEPH patients in the Korean Registry.
METHODS
The Korean Registry for Pulmonary Hypertension is a voluntary registry that was launched in 2007. Patients who were diagnosed with CTEPH between September 2008 and October 2011 were entered retrospectively in this study, and prospectively thereafter. All patients were evaluated at five University Hospitals (Asan Medical Center, University of Ulsan College of Medicine; College of Medicine, The Catholic University of Korea; Chung-Ang University College of Medicine; Seoul National University College of Medicine; Samsung Medical Center, Sungkyunkwan University School of Medicine) and data were collected by means of electronic data capture, starting with the initial baseline assessment reported in the medical records. One investigator visited each site to review the patient records and confirm the diagnoses. During this visit, data were also obtained on baseline assessments, treatments, and follow-up data including survival. The date of the diagnosis was considered as the date of the initial right heart catheterization or pulmonary angiography, ventilation-perfusion scan of the lungs, and chest multi-detector computed tomographic angiography. The patients were followed up with until death or the censoring date of December 31, 2011. Institutional ethics approval was sought for this study; however, no formal ethical approval was deemed necessary.
Study population
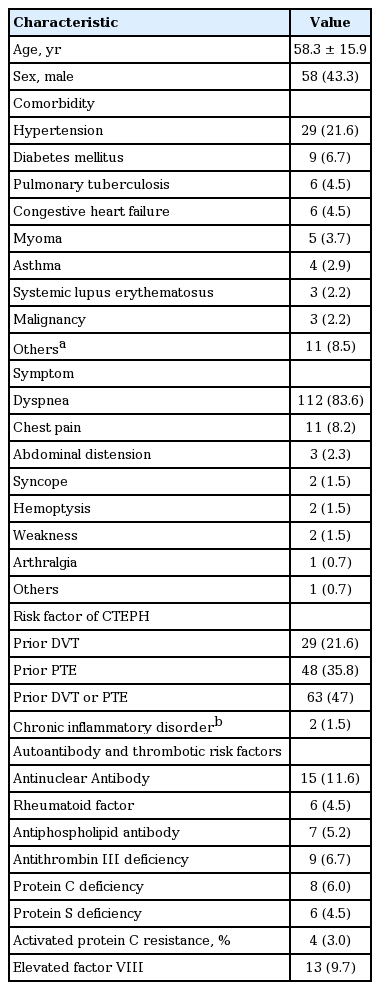
A total of 134 patients were assessed in this study; their baseline characteristics are shown in Table 1. Female patients (56.7%) outnumbered male patients. The overall median age of patients was 58.3 ± 15.9 years and 97 (72.4%) were more than 50 years. The median time between the onset of symptoms and diagnosis was 29.9 months and the presenting symptoms were dyspnea (83.6%), chest pain (8.2%), and hemoptysis (1.5%). At the time of diagnosis, four patients were in New York Heart Association (NYHA) class I, 36 were in class II, 37 were in class III, and 13 were in class IV. Forty-eight patients (35.8%) had PEs, while 29 patients (21.6%) had deep vein thrombosis. Two patients (1.5%) had chronic inflammation (inflammatory bowel disease or osteomyelitis), while malignant disease was observed in three patients and pulmonary tuberculosis was observed in six patients. Among the 134 total patients, 78 (58.2%) had at least one established thrombotic risk factor, including antiphospholipid antibodies, antithrombin III deficiency, protein C and S deficiencies, activated protein C resistance, and elevated factor VIII.
Baseline characteristics
Definitions
CTEPH was defined by the following observations after at least 3 months of effective anticoagulation therapy: (1) a mean pulmonary arterial pressure (PAP) > 25 mmHg with a pulmonary capillary pressure ≤ 15 mmHg, measured by right heart catheterization, or a right ventricular systolic pressure > 40 mmHg estimated by echocardiography; (2) at least one (segmental) perfusion defect detected by either lung scanning, multi-detector computed tomographic angiography, or pulmonary angiography.
The diagnosis of CTEPH was also established by transthoracic and transesophageal echocardiography using Doppler, pulmonary function tests including diffusion capacity for carbon monoxide (DLCO), right heart catheterization, pulmonary angiography, and a ventilation-perfusion lung scan. The CTEPH type was classified as either proximal or distal. For proximal type, a thrombus was present from the main pulmonary artery to the segmental artery. For distal type, occlusions were below the level of the segmental artery.
Statistical analysis
Data are presented as the median (interquartile range, 25% to 75%) for continuous variables, and as percentages (%) for categorical variables. For continuous variables, data were compared using the Mann-Whitney U test, while the chi-square test or Fisher exact test was used to assess categorical variables. To examine the association between mortality and CTEPH, a multiple logistic regression analysis was performed using covariates associated with mortality. Variables with p values ≤ 0.2 in univariate regression analyses were considered for multiple regression analysis. A p < 0.05 was considered statistically significant throughout the study. Data were analyzed using the PASW version 18.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
Diagnostic testing
Sixteen patients (11.9%) had right heart catheterization data recorded in the registry. Their median PAP was 39.6 ± 18.6 mmHg and their median right ventricle systolic pressure (RVSP) was 70.2 ± 25.4 mmHg. A complete two-dimensional echo examination was performed in all 128 patients. The median tricuspid regurgitation velocity was 4.0 ± 0.8 m/sec and systolic PAP was 74.7 ± 25.0 mmHg. A total of 98 patients (73.1%) exhibited abnormal perfusion scans, whereas ventilation scans were abnormal in 17 patients (12.7%). On average, the pulmonary function tests showed normal values. Forced vital capacity (FVC) was reduced in nine patients (< 2 L) and forced expiratory volume in 1 second (FEV1) was reduced in 21 patients (< 2 L) (Table 2).

Diagnostic evaluation
CTEPH types were also classified as proximal and distal: 105 patients (78.4%) belonged to the proximal CTEPH group, while 29 (21.6%) belonged to the distal CTEPH group. The proximal CTEPH group had a significantly lower median time between the onset of symptoms and diagnosis compared to the distal CTEPH group (p < 0.05). Additionally, the DLCO in the proximal CTEPH group was significantly lower than that of the distal CTEPH group (p = 0.007) (Table 3).

Differences between the distal and proximal chronic thromboembolic pulmonary hypertension groups
Treatment
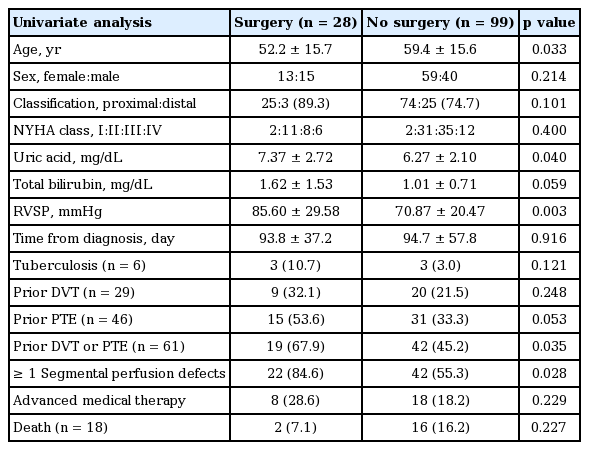
During CTEPH diagnosis, 28 patients (21%) had a pulmonary thromboendarterectomy (PTE), 99 (74%) had medical therapy, and seven (5%) had no data. Nineteen patients were treated with a prostacyclin PGI2 analog (beraprost sodium), while four patients were treated with an endothelin receptor antagonist (bosentan) or a phosphodiesterase type V inhibitor (sildenafil). Only three patients received combination therapies. The surgical group was younger (median age, 52.2 ± 15.7) than the non-surgical group; however, the two groups had similar gender distributions, median times between the onset of symptoms and diagnosis, and NYHA class. The non-surgical group had a lower RVSP (70.9 ± 20.5 vs. 85.6 ± 29.6, p = 0.003), less history of PE or deep vein thrombosis (42 [45.2%] vs. 19 [67.9%], p = 0.035), and less ≥ 1 segmental perfusion defects (42 [55.3%] vs. 22 [84.6%], p = 0.028), compared to the surgical group (Table 4). In the surgical group, 25 patients (89.2%) had proximal type CTEPH. For the proximal type of CTEPH, the overall survival rate of surgical group patients versus non-surgical group patients was 96% (24/25) and 82.4% (61/74; p = 0.03), respectively.
Differences between the surgical and non-surgical groups
Prognosis
During the study period, 18 patients (13.4%) died: two of these belonged to the surgical group, and 16 patients belonged to the non-surgical group (p = 0.227). The causes of death were cardiac events (n = 7, 38.9%), lung cancer (n = 4, 22.2%), disease progression (n = 4, 22.2%), and respiratory events (n = 3, 16.7%). In a univariate analysis, total cholesterol and median arterial pressure were associated with increased mortality. In a multivariate analysis, higher hemoglobin levels (relative risk [RR], 1.516; 95% confidence interval [CI], 1.053 to 2.184; p = 0.025) and lower total cholesterol levels (RR, 0.982; 95% CI, 0.965 to 0.999; p = 0.037) were associated with increased mortality (Table 5).

Multivariate analysis of the prognostic factor for mortality
DISCUSSION
This was the first national study of Korean patients with CTEPH. Based on 134 patients from the Korean Registry for Pulmonary Hypertension, baseline characteristics and outcomes were evaluated. CTEPH was equally common among men and women in their fifth decade of life and most patients were in NYHA dyspnea class II or III at the time of their diagnosis, consistent with the findings of previous studies [11-13]. CTEPH patients had numerous severe comorbidities in our study and, in general, the clinical presentation of an acute PE episode, and possibly venous thromboembolism (VTE) recurrences, increased the risk of developing CTEPH. Consistent with previous studies [1,14,15], 47% of patients had a prior episode of acute PE or DVT. The European CTEPH Registry recently revealed that previous PE episodes were detected in 74.8% of CTEPH patients, while previous DVT was documented in 56.1% of patients [11].
Acute episodes of VTE may be associated with the risk of developing CTEPH. In a prospective study, symptomatic CTEPH developed in 18 patients of the 305 patietnts with an acute episode of pulmonary embolism. In the multivariated analysis, a previous pulmonary embolism remained significantly associated with increased risk of CTEPH [14]. In a large retrospective study, a logistic regression analysis performed on 585 patients showed that both previous and recurrent VTEs were significantly associated with an increased risk of CTEPH (odds ratio [OR], 4.52; 95% CI, 2.35 to 9.12; and OR, 14.49; 95% CI, 5.40 to 43.08, respectively) [16].
CTEPH complicates a small but significant proportion of patients with acute PE. Thus, when treating patients with acute PE, physicians should be aware of the risks for progression to CTEPH. With this knowledge, the times to diagnosis may be reduced and adequately treat CTEPH after a PE episode.
Another remarkable comorbid condition in this study was pulmonary tuberculosis. Six patients had pulmonary tuberculosis and the association between this condition and pulmonary thromboembolism is concordant with previous studies [17-19]. Multiple studies have concluded that the high level of plasma fibrinogen, platelet aggregation, and impaired fibrinolysis associated with a decrease in antithrombin III and protein C levels appears to induce a hypercoagulable state promoting the development of venous thrombosis [20-22]. Some studies have reported that prothrombin deficiency occurs in one third of tuberculosis patients [21,23]; thus, the high proportion of patients with tuberculosis in CTEPH is most likely related to the relatively higher prevalence of pulmonary tuberculosis in Korea than in Europe or the United States.
On average, pulmonary function (FEV1, FVC, and FEV1/ FVC) was preserved in both the proximal and distal CTEPH groups in this study. The DLCO was significantly lower in the proximal CTEPH group than in the distal group, although some studies have reported a lower DLCO in the CTEPH group. The decrease of DLCO may include an increase in the thickness of the alveolar capillary membrane caused by a fibrotic or proliferative process and interstitial edema [24]. However, pulmonary function was measured in only 50% of patients in our cohort. Therefore, large studies are still required to evaluate pulmonary function in CTEPH.
In this study, 25 patients with proximal type CTEPH underwent PTE. For the proximal CTEPH group patients, the numbers of survivors in the surgical and non-surgical groups were 24 (96%) and 61 (82.4%), respectively (p = 0.03). The PTE procedure increases survival among patients in the proximal CTEPH group, compared to those who received medical therapy. PTE remains the preferred treatment option for CTEPH [2], and the current PTE procedure provides excellent results with a worldwide in-hospital mortality rate of 4.4% to 10% [25]. The low mortality rate (4.7%) reported in the present study is in agreement with that previous finding and reflects a combination of increased surgeon experience and adequate selection of eligible patients [2,11]. Thus, PTE should be considered as the first treatment option for patients with proximal CTEPH. Due to nonspecific symptoms and an often unremarkable physical examination during the early course of CTEPH, diagnostic misclassifications or other delays in diagnosis are common. A lack of disease awareness by physicians also plays a role in this delay [11]. Accurate CTEPH diagnosis and characterization of its progression and distribution are imperative for prompt treatment, particularly in patients suitable for PTE.
In our study, higher hemoglobin and lower cholesterol levels were associated with mortality. Prolonged exposure to hypoxia is also associated with an increase in red blood cell mass, which aggravates PH by increasing blood viscosity. Uncorrected chronic hypoxemia is associated with the development of polycythemia and untreated sustained PH showed poor prognosis. The presence of hypoxemia is strongly associated with increased morbidity and reduced survival; thus, higher hemoglobin is related with higher mortality in CTEPH [26,27].
Data regarding lower cholesterol levels as a risk factor for CTEPH are conflicting. Some studies have shown an association between elevated low density lipoprotein (LDL) and low high density lipoprotein levels and the risk of VTE [28,29]. Other studies, however, did not find an association between LDL-cholesterol levels and the risk of CTEPH [30,31].
There were several limitations to this study. The main limitation was the retrospective nature of the data collection. Thus, retrieval bias may have been introduced because information was gathered from notes with differing levels of completeness. The effects of missing hemodynamic and functional data were accounted for in the regression models by including missing category variables. Given that most of the participating centers were referral centers for CTEPH and PTE, the proportion of surgical patients may have been overestimated due to referral bias.
In conclusion, this was the first national study of Korean patients with CTEPH. The baseline characteristics and symptoms of CTEPH patients were similar to previous studies. The prognosis of patients with CTEPH was poor unless an early diagnosis was made and treatment was initiated. Thus, accurate CTEPH diagnosis and characterization of its extent and distribution are imperative for prompt initiation of treatment, especially in patients eligible for PTE.
KEY MESSAGE
1. This study was the first national cohort study of Korean patients with chronic thromboembolic pulmonary hypertension (CTEPH).
2. In a multivariate analysis, higher hemoglobin and lower total cholesterol levels were associated with increased mortality.
3. The pulmonary thromboendarterectomy (PTE) procedure significantly increased survival in patients with proximal CTEPH compared to medical therapy. However, a larger, prospective study remains necessary to establish the effects of PTE in Korea.
Notes
No potential conflict of interest relevant to this article was reported.