Long-term real-world entecavir therapy in treatment-naïve hepatitis B patients: base-line hepatitis B virus DNA and hepatitis B surface antigen levels predict virologic response
Article information
Abstract
Background/Aims
Entecavir is a potent nucleoside analogue with high efficacy and barrier for resistance. We aimed to investigate the long-term efficacy and viral resistance rate of entecavir and explore the factors associated with virologic response, including quantitative hepatitis B surface antigen (qHBsAg) levels.
Methods
One thousand and nine treatment-naïve chronic hepatitis B (CHB) patients were evaluated for cumulative rates of virologic response, biochemical response, and entecavir mutations. The role of baseline qHBsAg for virologic response was assessed in 271 patients with qHBsAg prior to entecavir treatment.
Results
The median duration of entecavir treatment was 26.5 months. The cumulative rate of virologic response at years 1, 3, and 5 were 79.0%, 95.6%, and 99.4%, respectively. The cumulative rate of entecavir resistance was 1.0% and 2.1% in years 3 and 5. Multivariate analysis identified baseline hepatitis B e antigen (HBeAg) negative status (p < 0.001) and lower hepatitis B virus (HBV) DNA (p < 0.001) as predictors of virologic response. Lower qHBsAg was an independent predictor of virologic response in patients with baseline qHBsAg. There were no serious adverse events during treatment.
Conclusions
Long-term entecavir treatment of nucleos(t)ide-naïve CHB patients was associated with an excellent virologic response and a low rate of entecavir-resistant mutations at 5 years. Baseline HBV DNA load, qHBsAg levels, and HBeAg status were predictors of virologic response during entecavir treatment.
INTRODUCTION
Hepatitis B virus (HBV) is estimated to have infected more than 2 billion people worldwide, of whom 350 to 400 million people are chronically infected [1]. Chronic hepatitis B (CHB) patients are at an increased risk for liver-related complications, including cirrhosis, liver failure, hepatocellular carcinoma, and death [2]. The Risk Evaluation of Viral Load Elevation and Associated Liver Disease/Cancer (REVEAL) study demonstrated that progression to liver cirrhosis and hepatocellular carcinoma are strongly correlated with HBV DNA loads [3,4]. Therefore, the goals of treatment for CHB patients are to suppress HBV viral replication to undetectable levels and achieve prevention of cirrhosis and hepatocellular carcinoma [5,6].
Entecavir is a high efficacy guanosine nucleoside analogue (NUC) with a selective polymerase inhibitor of HBV replication. Among hepatitis B e antigen (HBeAg)-positive and HBeAg-negative patients at 48 weeks into their treatment, the rates of virologic response, biochemical response, and improvement of histological findings were significantly greater among patients receiving entecavir than those receiving lamivudine [7,8]. Extension of these studies demonstrated that, with prolonged treatment, higher rates of virologic response are achieved [9]. Moreover, the development of drug resistance is reported to occur at a rate of only 1.2% after 5 years of entecavir treatment in treatment-naïve CHB patients [10].
Compared to registration studies, real-world populations are more heterogeneous in terms of age and types of comorbidities; therefore, real-world data are required to confirm drug efficacies and monitor drug safety. Empirical data about entecavir use have been found to be similar to data from registration trials, with high efficacy and a good safety profile. However, these empirical studies are limited by their small enrollment numbers, short follow-up periods, and focus on Western populations [11].
In patients treated with antiviral agents, outcomes that include worse clinical prognosis in CHB patients with inadequate virologic response emphasize the need for biomarkers that can predict treatment outcomes [12,13]. These markers could identify patients with poor clinical outcomes and aid in individualizing therapy for them. Baseline and on-treatment response of HBV DNA loads are well known predictors of treatment outcomes for patients on antiviral therapy. Recently, quantitative hepatitis B surface antigen (qHBsAg) has been developed as a marker for evaluating viral replication and a predictor of treatment response in patients treated with interferon. However, currently there is limited data on the role of qHBsAg levels in CHB patients treated with oral antiviral therapy.
The aims of this study were to investigate the long-term efficacy and viral resistance of entecavir therapy in a real world setting and to explore the factors associated with virologic response, including qHBsAg levels.
METHODS
Patients and treatment
One thousand and nine consecutive treatment-naïve HBV-infected patients, whose treatment was initiated with 0.5 mg of daily entecavir at Samsung Medical Center from 2007 through 2012, were enrolled. All patients were chronically infected with HBV and were confirmed as HBsAg-positive for at least 6 months. Exclusion criteria consisted of coinfection with hepatitis C virus or human immunodeficiency virus, prior treatment history with NUCs or interferon, entecavir treatment less than 24 weeks, prior diagnosis of hepatocellular carcinoma, being younger than 18 years old, and insufficient clinical data (Fig. 1). The indication for antiviral therapy followed those of the Korean Association for the Study of the Liver guidelines [14] and included: HBeAg-positive CHB patients with HBV DNA loads of ≥ 20,000 IU/mL and alanine transaminase (ALT) levels of ≥ 2 × the upper normal limit (UNL), HBeAg-negative CHB patients with HBV DNA loads ≥ 2,000 IU/mL and an ALT level of ≥ 2 × the UNL, compensated cirrhotics with HBV DNA loads ≥ 2,000 IU/mL regardless of the ALT level, and decompensated cirrhotics with any detectable HBV DNA loads.

Flow chart of patients included in the study.
This study was approved by the Institutional Review Board of Samsung Medical Center (IRB 2014-03-158).
Assessment
All patients underwent complete blood counts, liver function tests, HBV virologic markers, HBV DNA load counts, and imaging studies (abdominal sonography, computed tomography, or magnetic resonance imaging); these assessments were completed at baseline and were repeated at 3- to 6-month intervals. HBsAg, anti-HBs antibody, HBeAg, and anti-HBe antibody levels were examined by enzyme immunoassay. HBsAg levels were quantified by automated chemiluminescent microparticle immunoassay (Architect HBsAg, Abbott, IL, USA). HBV DNA loads were measured using the COBAS TaqMan HBV quantitative test (Roche Molecular Systems Inc., Branchburg, NJ, USA), with a lower detection limit of < 9 IU/mL. Viral mutational analysis was performed by direct sequencing of the reverse transcriptase (RT) domain of the HBV polymerase gene. Virologic responses were defined as a reduction in HBV DNA loads to < 60 IU/mL. Biochemical response was defined as ALT < 40 U/L. Virologic breakthroughs were defined as an increase in serum HBV DNA loads by > 1 log10 above the nadir after achieving a virologic response during continued treatment. Liver cirrhosis was determined by liver biopsy or an imaging modality combined with two positive laboratory findings (e.g., platelet levels < 100,000/µL, albumin levels < 3.5 g/dL, or prothrombin time [PT, international normalized ratio] > 1.3).
Statistical analyses
Baseline characteristics were summarized with descriptive statistics and are presented as a mean ± standard deviation or as percentages. In all study subjects, continuous variables were compared parametrically using the Student t test or non-parametrically using the Mann-Whitney U test. Categorical variables were compared using the chi-square test or the Fisher exact test as appropriate. Cumulative rates of virologic and biochemical responses were analyzed using the Kaplan-Meier method. Independent risk factors predicting achievement of virologic response and viral resistance were analyzed with the stepwise Cox regression analysis. A two-sided p < 0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 19.0 (IBM Co., Armonk, NY, USA).
RESULTS
Patient demographics
Baseline patient characteristics are listed in Table 1. The majority of patients were male (64.5%) and the median patient age was 48 years old (range, 18 to 80). The patients were followed up for a median of 28.0 months (range, 6.0 to 77.4). Five hundred and seventy-one (56.6%) patients were HBeAg-positive and 438 patients (43.4%) were HBeAg-negative. The mean baseline HBV DNA load was 6.47 ± 1.40 log10 IU/mL and 36.2% of the patients had liver cirrhosis at initiation of entecavir treatment. Stored baseline serum samples were available for qHBsAg analysis in 271 patients and retrospective measurement of qHBsAg in these patients revealed a median of 3,668.5 IU/mL (range, 1.15 to 124,925.0).

Baseline characteristics of treatment-naïve patients (n = 1,009)
Entecavir efficacy
Among 1,009 patients, the cumulative biochemical response rates were 81.0%, 95.0%, and 99.5% at years 1, 3, and 5, respectively. The cumulative virologic response rates in the entecavir-treated patients were 80.0%, 95.6%, and 99.4% at years 1, 3, and 5, respectively (Fig. 2A). Sixty-four patients (6.3%) failed to achieve a virologic response during follow-up. The cumulative virologic response rate in HBeAg-negative patients, which was 94.5% after the first year and 99.5% after the third year, was significantly higher than that of HBeAg-positive patients, which was 67.1% after the first year and 92.5% after the third year (p < 0.001) (Fig. 2B). Compared to patients with HBV DNA loads < 4 log10 IU/mL, patients with higher HBV DNA loads had a significantly lower virologic response (p ≤ 0.001) (Fig. 2C).
Virologic response of patients on continuous entecavir treatment. (A) The cumulative virologic response rate increased with time, reaching 99.4% at year 5. (B) Hepatitis B e antigen (HBeAg)-negative patients had a statistically higher rate of virologic response at year 1, 3, and 5. (C) The cumulative virologic response rate in patients with high hepatitis B virus (HBV) DNA loads, compared to patients with HBV DNA loads < 4 log10 IU/mL resulted in a significantly lower virologic response. (D) The log-rank test was used to compare the differences in the viral responses between each group. The cumulative entecavir resistance rates were 0% after 1 year, 1.0% after 3 years, and 2.1% after 5 years.
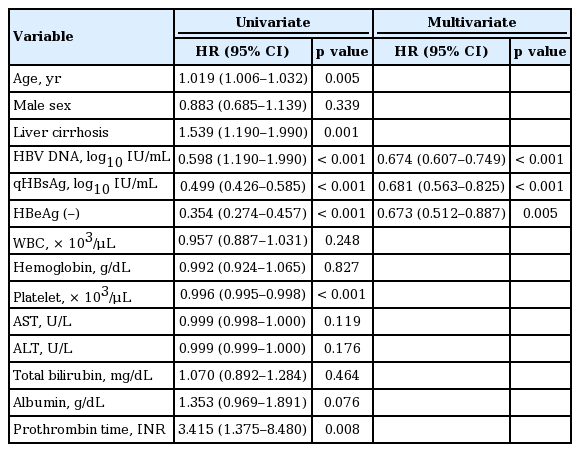
Univariate analysis revealed that older age, presence of liver cirrhosis, lower HBV DNA load, HBeAg negativity, lower platelet count, and prolonged PT were statistically significant factors associated with virologic response. In multivariate analysis, only HBeAg-negativity and lower HBV DNA load were independently associated with virologic response (Table 2).

Univariate and multivariate analysis of factors associated with virologic response in entecavir-treated chronic hepatitis B patients (n = 1,009)
The cumulative HBsAg seroclearance rates were 0.4%, 0.7%, and 1.6% in years 1, 3, and 5, respectively. Among the 571 HBeAg-positive patients, the cumulative HBeAg seroclearance rates at years 1, 3, and 5 were 4.1%, 19.2%, and 40.2%, respectively.
Virologic breakthroughs
Fifty-six patients (5.9%) experienced virologic breakthroughs during the follow-up period. Noncompliance was confirmed in 42 patients (75.0%) and of the remaining 14 patients, virologic resistance was confirmed in 12.
Virologic resistance
Only 12 patients (1.2%) out of the 1,009 treatment-naïve patients developed confirmable entecavir resistance. The cumulative entecavir resistance rates were 0% after 1 year, 1.0% after 3 years, and 2.1% after 5 years, respectively (Fig. 2D). The characteristics of patients who developed entecavir resistance are summarized in Table 3. The median time to resistance was 34 months (range, 21 to 66). All patients were HBeAg-positive, with a median HBV DNA load of 7.95 log10 IU/mL (range, 5.30 to 8.04). Baseline serum samples were available in six patients with documented entecavir resistance during follow-up and an rtV214A mutation was identified in two patients.
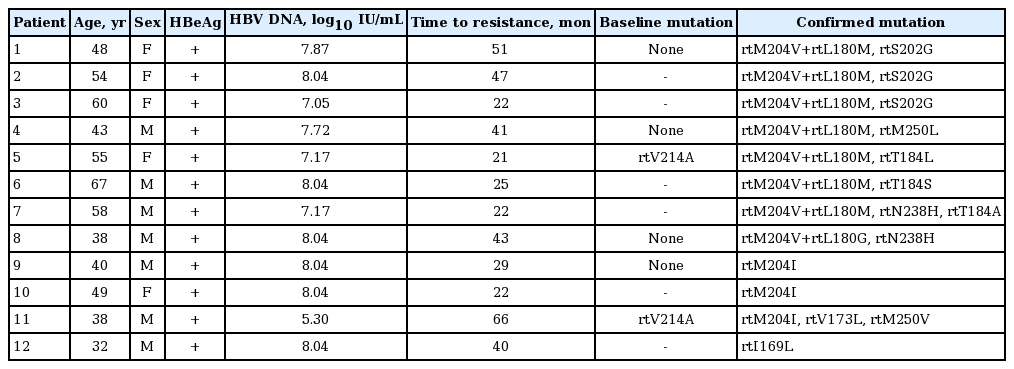
Characteristics and mutation sites of entecavir-resistance confirmed patients
The role of qHBsAg levels in predicting virologic response
Stored baseline serum samples were available in 271 patients (126 HBeAg-negative and 145 HBeAg-positive patients) and qHBsAg levels prior to entecavir treatment were measured. Multivariate analysis of the predictive factors of virologic response was performed in this 271-patient set, which revealed that lower qHBsAg levels (p < 0.001), lower HBV DNA loads (p < 0.001), and HBeAg-negative status (p = 0.005) were independently associated with virologic response (Table 4). Compared to patients with qHBsAg levels < 5,000 IU/mL, patients with greater qHBsAg levels had a significantly lower cumulative virologic response (p ≤ 0.001) (Fig. 3A). In HBeAg-positive patients, significantly greater HBeAg seroclearance was achieved in patients with qHBsAg levels < 5,000 IU/mL (p = 0.002) (Fig. 3B). Because low viral load is a significant factor in predicting virologic response, patients were grouped into low-viral load (HBV DNA load ≤ 6 log10 IU/mL) and high-viral load (HBV DNA load > 6 × log10 IU/mL) groups. In the low-viral load group, there was no significant difference in virologic response based on qHBsAg levels (p = 0.378) (Fig. 3C). However, there was a significant difference between the virologic response rate in the high viral load group based on low (≤ 5,000 IU/mL) and high (> 5,000 IU/mL) qHBsAg levels (p < 0.001) (Fig. 3D). The virologic response of the high viral load group at 6, 12, and 24 months was 46.7%, 89.3%, and 98.7%, respectively, in patients with qHBsAg levels ≤ 5,000 IU/mL; and 20.7%, 62.2%, and 84.6%, respectively, in patients with qHBsAg levels > 5,000 IU/mL.
Univariate and multivariate analysis of factors associated with virologic response in entecavir-treated chronic hepatitis B patients with baseline qHBsAg (n = 271)
Virologic response and hepatitis B e antigen (HBeAg) seroclearance based on quantitative hepatitis B surface antigen (qHBsAg) level. (A) The cumulative virologic response rate was significantly greater in patients with baseline qHBsAg < 5,000 IU/mL. (B) In HBeAg-positive patients, baseline qHBsAg < 5,000 IU/mL was associated with a significantly greater cumulative rate of HBeAg seroclearance. (C) The cumulative virologic response rate was not statistically different among patients with low viral loads (≤ 6 log10 IU/mL), regardless of qHBsAg levels. (D) In the high viral load group (high hepatitis B virus [HBV] DNA > 6 log10 IU/mL), patients with low qHBsAg (≤ 5,000 IU/mL) had a significantly greater virologic response compared to patients with high qHBsAg levels (qHBsAg > 5,000 IU/mL, p < 0.001).
Clinical safety
There were no serious adverse events reported during treatment. The reasons for patient noncompliance included economical difficulties and treatment fatigue after a prolonged adherence period. None of the patients stopped treatment due to problems with side effects.
DISCUSSION
CHB patients with high levels of HBV DNA have an increased risk for developing liver cirrhosis and hepatocellular carcinoma [3,4]. Therefore, suppression of HBV DNA is a critical goal in treating CHB patients [5,6]. Herein we present results from a long-term empirical study and report predictors of virologic response in treatment-naïve CHB patients treated with entecavir.
Genotype C is associated with a high likelihood of a longer period of persistent hepatitis, which increases the risk of liver cirrhosis and hepatocellular carcinoma [15,16]. In genotype C patients, the antiviral efficacy of lamivudine compared to other genotypes had conflicting outcomes [17-20]. Although direct comparison with other genotypes is not feasible because 95.6% to 100.0% of HBV patients in Korea are infected with genotype C [16,21,22], it is possible to provide an indirect comparison with entecavir efficacy among the genotypes. The cumulative virologic response rates to entecavir were 80.0%, 95.6%, and 99.4% after years 1, 3, and 5, respectively, which are comparable to previous long-term studies across multiple populations with various genotypes [23,24].
During the treatment period, 56 patients (5.9%) exhibited an increase in serum HBV DNA loads by > 1 log10 above the nadir, even after achieving a virologic response to treatment. Among these patients, 42 (42/56, 75.0%) were noncompliant and resistance mutations were identified in 2.1% of patients after 5 years of treatment. These results are comparable to those from a previously study by Yuen et al. [25] in which they reported three cases of viral breakthroughs among 222 patients over a 3-year treatment period, and Ono et al. [24] reported a 1.1% chance of viral breakthrough over a 4-year treatment period.
It is known that entecavir resistance requires three HBV RT substitutions: rtM204V and rtL180M, plus an additional mutation at rtT184, rtS202, or rtM250 [26]. Among patients with confirmed virologic resistance, seven patients fit this pattern. Interestingly, one of our patients (no. 8) had a different substituting amino acid at rtL180G that accompanied rtM204V and rtN238H. rtN238H has been reported to be associated with known adefovir dipivoxil resistance mutations, such as rtN236T and rtA181T/V [27]. Two patients (no. 9, 10) presenting with rtM204I mutations without additional mutations at rtT184, rtS202, or rtM250 experienced a virologic breakthrough. Another patient (no. 11) with rtM204I, rtV173L, and rtM250V mutations also experienced a virologic breakthrough. The rtV173L gene has been reported to enhance in vitro viral replication in lamivudine-treated patients [28]. One patient (no. 12) with an rtI169L mutation presented with primary non-response and eventually experienced a virologic breakthrough. Tenney et al. [29] reported that rtI169T substitutions increase the level of entecavir resistance 2- to 3-fold in select cases and rtI169T mutation was thought to be an ancillary or adaptive change to entecavir. To understand these patterns better, future in vitro analyses of rtI169L are needed.
Yang et al. [13] found a reduced risk of liver related events and HCC in entecavir-treated patients who experienced virologic response. A previous study done at our center also found increased HCC risk in patients with incomplete virologic response to treatment [12]. The patients with lower HBV DNA loads and baseline HBeAg-negativity had a significantly greater probability of achieving virologic response (p < 0.001). Thus, the two independent factors found to be predictive of virologic response in our study, baseline HBV DNA loads and HBeAg status, are comparable to previous viral efficacy studies of both lamivudine-treated and entecavir-treated patients [24,30-32].
Studies of qHBsAg have shown that titers correlate with serum HBV DNA load and intrahepatic covalently closed circular DNA level, which is the transcriptional template of HBV [33,34]. Low pretreatment serum qHBsAg level has been found to be a predictor of response to pegylated interferon therapy [35]. However, although NUCs are effective in suppressing HBV DNA load, limited data regarding the role of qHBsAg titers are available in patients treated with NUCs. The results of our study revealed that HBV DNA load (p < 0.001), HBeAg status (p = 0.005), and qHBsAg levels (p < 0.001) are independent predictors of virologic response. These data suggest that qHBsAg level may complement HBV DNA load in predicting virologic response in patients treated with NUCs. In patients with high HBV DNA loads, low qHBsAg titer (≤ 5,000 IU/mL) was associated with a significantly greater virologic response. In low HBV DNA loads, the qHBsAg titer may have less power in differentiating the predictability for virologic response. Thus, qHBsAg titer may be used as an independent predictor of virologic response in patients with high viral loads. Patients with a combination of HBV DNA loads > 6 log10 IU/mL and qHBsAg levels > 5,000 IU/mL can be considered to have the greatest risk of a poor virologic response. In HBeAg-positive patients, low qHBsAg titers were also predictors of HBeAg seroclearance. These results are comparable to those from a study by Lee et al. [36] in which lower levels of qHBsAg predicted HBeAg seroclearance/seroconversion.
Although our retrospective design has limitations, we present a large empirical study of treatment-naïve patients receiving entecavir. There is still limited data on the role of qHBsAg levels and our relatively large sample size and analyses using baseline qHBsAg levels offers new insights into the role of qHBsAg in predicting viral response.
In conclusion, continuous treatment with entecavir for treatment-naïve, genotype-C, CHB patients over 5 years shows an excellent virologic response rate and a low rate of resistance, which is comparable to results from registration trials. Baseline HBV DNA loads, qHBsAg levels, and HBeAg status were predictors of virologic response during entecavir treatment.
KEY MESSAGE
1. Long-term entecavir treatment is associated with an excellent virologic response and a low rate of entecavir-resistant mutation.
2. Baseline hepatitis B virus DNA load, quantitative hepatitis B surface antigen levels, and hepatitis B e antigen status are predictors of virologic response of entecavir treatment.
Notes
No potential conflict of interest relevant to this article was reported.