Effect of Helicobacter pylori eradication on the regression of gastric polyps in National Cancer Screening Program
Article information
Abstract
Background/Aims
Western guidelines recommend Helicobacter pylori eradication in H. pylori-associated gastric polyps; however, there is no standard guideline in Korea. The aim of this study is to assess the effect of H. pylori eradication on the regression of gastric hyperplastic polyps in National Cancer Screening Cohort, representative of general population.
Methods
Among participants in National Cancer Screening Program, subjects who had H. pylori positive gastric hyperplastic polyps less than 10 mm and underwent follow-up endoscopy and H. pylori testing were enrolled. The effect of H. pylori eradication on hyperplastic gastric polyps was estimated using odds ratios (ORs) and 95% confidence intervals (CIs).
Results
A total of 183 H. pylori infected subjects with hyperplastic polyp at baseline underwent follow-up endoscopy and H. pylori test after mean of 2.2 years. Successful H. pylori eradication markedly induced the disappearance of hyperplastic polyps comparing to non-eradication group (83.7% vs. 34.1%, p = 0.001). Successful eradication increased the possibility of disappearance of hyperplastic polyps (adjusted OR, 5.56; 95% CI, 2.63 to 11.11). Polyp size was inversely related with the disappearance of hyperplastic polyps (adjusted OR, 59; 95% CI, 0.48 to 0.71).
Conclusions
Eradication of H. pylori infection may induce disappearance of gastric hyperplastic polyps in National Cancer Screening Cohort.
INTRODUCTION
Gastric polyps are usually asymptomatic and are found incidentally. The most common types of gastric polyps are hyperplastic polyps, which are related with Helicobacter pylori infection, and fundic gland polyps, which are associated with the use of proton pump inhibitor (PPI). The incidence of gastric polyps has increased because the prevalence of H. pylori has decreased but the use of PPI markedly increased during the past few decades [1]. Therefore, hyperplastic polyps have decreased and fundic gland polyps have increased in Western country. However, in East Asian where H. pylori infection remains high, larger proportions of gastric polyps are still hyperplastic [2].
Even though hyperplastic polyps rarely progress to neoplastic lesion, they are associated with synchronous gastric neoplasm. The prevalence of dysplasia arising in hyperplastic polyps has been reported from 2% to 19% and synchronous gastric cancer varies from 0.6% to 2% [2-7]. Previous small studies suggest that H. pylori eradication induced regression of hyperplastic polyps [8-11]. The British Society of Gastroenterology strongly recommends H. pylori eradication in persons with hyperplastic polyps [2]. However, Korean national medical insurance doesn’t cover H. pylori eradication for H. pylori associated gastric polyps. Previously we reported the disappearance of hyperplastic polyps after H. pylori eradication in private screening cohorts [12]. Even if private screening cohort is close to general population, they are motivated persons for health care and private screening program is expensive. Therefore, private screening cohort may have a little selection bias. National Cancer Screening Program (NCSP) provides endoscopy without any payment or with a little payment according to their income. Now we assessed the effect of H. pylori eradication on gastric hyperplastic polyp in National Cancer Screening Cohorts.
METHODS
Study population at baseline
Participants were enrolled from a NCSP at the National Cancer Center from May 2007 to December 2013. Korean NCSP for gastric cancer screening recommends 2-year interval screening of endoscopy or upper gastrointestinal series from 40 years of age [13]. Endoscopic and pathologic records from electrical data base were reviewed and subjects with H. pylori positive hyperplastic polyp at baseline were included. We excluded absence of hyperplastic polyp (n = 11,098) and subjects with neoplastic lesion at baseline (n = 32). Among 32, dysplasia (n = 16) and cancer (n = 4) were synchronously observed in hyperplastic polyps. A total of 1,131 participants with hyperplastic polyps were initially screened. Additionally, 210 subjects with tiny polyps less than 3 mm and 584 subjects without follow-up endoscopy and 154 H. pylori negative subjects at baseline was excluded (Fig. 1).
Study flow. Of a total of 11,279 subjects from 2007 to 2013, 1,131 persons had hyperplastic polyps. Of a total of 1,131 subjects with hyperplastic polyps, 183 eligible persons were analysed in a cohort study. EGD, esophagogastroduodenoscopy; HP, Helicobacter pylori.
The study was approved by the Institutional Review Board of National Cancer Center (IRB No. NCCNCS-13835), and performed in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent.
Endoscopy and follow-up
Esophagogastroduodenoscopy was performed using a flexible endoscope (Q260, Olympus Optical, Tokyo, Japan) by mainly four gastroenterologists after the subject fasted overnight. Pharyngeal anesthesia with 4% xylocaine spray and almost all participants received non-conscious endoscopy. H. pylori test was performed using histologic test if any focal lesions were present in the stomach or duodenum. The size and site of polyp were described during endoscopy. Gastric polyps were histologically confirmed as hyperplastic polyp and fundic gland polyp (Fig. 1). Hyperplastic polyps are inflammatory proliferations of the gastric foveolar cells. We defined hyperplastic polyps using review article of Shabi et al.’s review article [14]. In summary, hyperplastic polyps include polypoid foveolar hyperplasia, which are elongated, distorted, branching, and dilated hyperplastic foveolae lying in an edematous stroma and hyper-vasculature, and inflammatory polyps, which are characterized as small haphazardly distributed smooth muscle bundles with chronic and active inflammation [14]. If a person has multiple polyps, it was considered as one person with polyps.
H. pylori eradication was provided to persons with clinical indications (duodenal or benign gastric ulcer) or with non-ulcer dyspepsia or asymptomatic subjects according to the participant’s request [15]. H. pylori eradication therapy consisted of omeprazole 20 mg, clarithromycin 500 mg, and amoxicillin 1,000 mg, twice daily for 7 days. Quadruple therapy was provided in the cases of triple therapy failure. H. pylori eradication was confirmed using the C13 urea breath test, rapid urease test, or histologic examination at 4 to 8 weeks after completion of the eradication treatment. Most participants underwent follow-up endoscopy after 2 years according to NCSP recommendation but a part of participants followed up earlier or later than 2 years. Follow-up endoscopy was performed 1 to 3 years (mean of 2.2 years) after initial endoscopy (Fig. 1). At follow-up, subjects were classified into two groups; successful eradication group and non-eradication group.
Statistical analyses
Data are presented as mean ± standard deviation (SD) or number (percent). The Pearson chi-square test, independent t test was performed to assess the difference in risk. Effects of H. pylori eradication and cofactors on the regression of gastric hyperplastic polyps were estimated with odds ratios (ORs) and 95% confidence intervals (CIs) using logistic regression analysis. Significant risk factors in t test or chi-square test were subjected to multivariate analysis. Adjusted analysis was performed to investigate the effect of H. pylori eradication on the disappearance of hyperplastic polyps at follow-up. All statistical analyses were performed using STATA version 12 (StataCorp LLC, College Station, TX, USA). All statistical tests were two-sided, and p < 0.05 was considered statistically significant.
RESULTS
Characteristics of participants at baseline
A total of 11,279 persons underwent endoscopy and H. pylori testing from 2007 to 2013 (Fig. 1). Among 1,131 hyperplastic polyp, 183 subjects met with our study aim. Mean age was 57.5 ± 9.8 years and male sex was 32.8% (n = 60) (Table 1). Hyperplastic polyps were measured with mean of 4.6 mm and were mainly distributed at the antrum and body (48.5% and 36.9%, respectively).
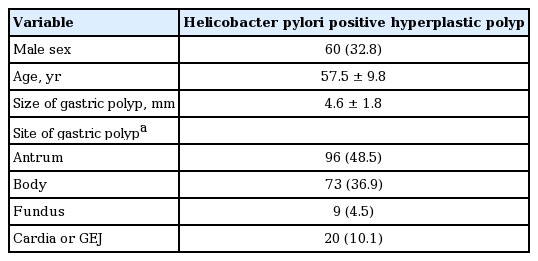
Baseline characteristics of eligible participants (n = 183)
Effect of H. pylori eradication on the regression of hyperplastic polyps
Participants with hyperplastic polyps were followed up and those who did not undergo endoscopy or H. pylori testing were excluded. We excluded removed polyps and small polyps less than 3 mm which they have a high possibility of regression or removal after biopsy (Fig. 1). A total of 183 persons were eligible to be analyzed with mean follow-up duration of 2.2 years (Fig. 1).
Eighty four percent of hyperplastic polyps disappeared after successful H. pylori eradication, whereas only 34% of them disappeared in H. pylori non-eradication group (Table 2). Location of polyps had no difference between persistent hyperplastic polyps (40 antrum, 27 body, three fundus, and 11 cardia or gastroesophageal junction [GEJ]) and disappearance of hyperplastic polyps (56 antrum, 46 body, six fundus, nine cardia or GEJ). Gastric polyp size in persistent hyperplastic polyp group was larger than that in disappearance group (5.3 mm vs. 4.1 mm). In adjusted analysis, H. pylori eradication significantly induced the disappearance of hyperplastic polyps (adjusted OR, 5.56; 95% CI, 2.63 to 11.11), whereas polyp size was inversely associated with the disappearance of hyperplastic polyps (adjusted OR, 0.59; 95% CI, 0.48 to 0.71). In adjusted analysis, diagnostic age, sex, and follow-up duration had no association with disappearance of hyperplastic polyps (Table 2).
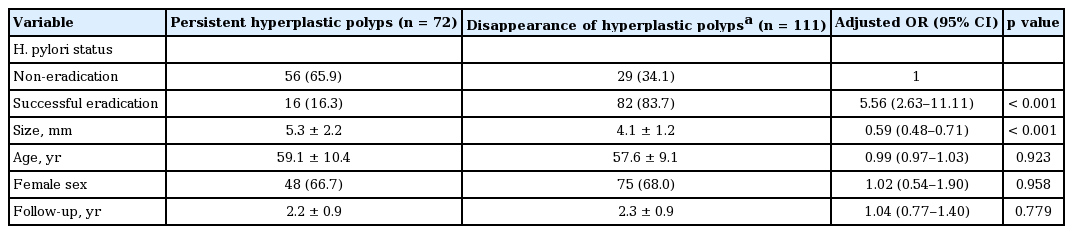
Effect of Helicobacter pylori eradication on the course of hyperplastic polyps
DISCUSSION
In this study, H. pylori eradication induced the disappearance of hyperplastic polyps and larger polyps were less likely disappeared, whereas age, sex and follow-up year had no effect on the regression of hyperplastic polyps.
H. pylori eradication induced a significant disappearance of hyperplastic polyps (84%) in National Cancer Screening Cohort. This result is very similar with the results from a previous private screening cohort (85% disappearance of hyperplastic polyps after H. pylori eradication) [12]. Previous small studies from Japan and China also showed 68% to 85% regression of hyperplastic polyps in H. pylori eradication group [8-11]. H. pylori eradication markedly induced the disappearance of hyperplastic polyps (adjusted OR, 5.5) comparing to non-eradication group in this National Cancer Screening Cohort. This result is similar to that of previous private screening cohort (adjusted OR, 11.7) [12]. These results provide the evidence of H. pylori eradication in H. pylori-related gastric polyp. Hyperplastic polyp is well known to be associated with H. pylori infection [1,2]. The disappearance of hyperplastic polyp after H. pylori eradication looks to be related to reduction or disappearance of H. pylori-induced inflammation.
British Society of Gastroenterology strongly recommends H. pylori eradication and an endoscopic follow-up in patients with hyperplastic polyps [2]. Small hyperplastic polyps may spontaneously regress or disappear [11]. In this study, 34% of hyperplastic polyps disappeared without any treatment in H. pylori positive group. Previous private screened cohort study also showed 29% of hyperplastic polyps disappeared without eradication in H. pylori positive group [12]. However, 66% to 70% of hyperplastic polyps still remains during mean follow-up of 2 years in both studies. A previous Chinese study showed that polyps disappeared in H. pylori eradication group (68.2%) and H. pylori eradication rate was 86.4% (19/22); however, change in polyps was not noted in non-eradication group [16]. Korean national medical insurance doesn’t approve H. pylori eradication in patients with hyperplastic polyps and there is no standard guideline for the follow-up interval for gastric polyps. Korean NCSP provide esophagogastroduodenoscopy every 2 years for gastric cancer screening with age older than 40 years [13]. Therefore, gastric polyps less than 1cm are usually followed up every 2 years and gastric polyps lager than 1 cm are usually resected. However, American Society for Gastrointestinal Endoscopy guideline recommends polypectomy for gastric polyp larger than 5 mm (if H. pylori positive, H. pylori eradication has been associated with regression of hyperplastic polyp) [17].
Increased gastric polyp size was inversely associated with disappearance of hyperplastic polyps in this study. We excluded tiny polyps less than 3 mm and removed polyps at baseline. Small polyps after biopsy may be spontaneously disappeared and it might be ignored or missed at the follow-up endoscopy because this study is retrospective study. Location of gastric polyp had no association with disappearance of hyperplastic polyps.
Male portion was 33% in gastric hyperplastic polyps. Mean age in this study was older than in private screening cohort (57 years vs. 53 years). Mean polyp size was slightly larger than previous private screening cohort (4.6 mm vs. 4.2 mm) [12]. Hyperplastic polyps were mainly distributed at antrum and body (85%). Age, sex, and follow-up duration had no association with the regression of gastric hyperplastic polyps. These results were similar to previous private screening cohort [12].
This study has several strengths. First, this study evaluated the effect of H. pylori eradication on the regression of gastric polyps in a NCSP that government provides 2 years interval endoscopic screening to all persons who was older than 40 years regardless of their income. Therefore, the study population can be representative as general population. Second, the effect of H. pylori eradication on gastric hyperplastic polyps in this study are very similar with the results from private screening cohort despite of different mean age between two cohorts. This suggests that the effect of H. pylori eradication on gastric hyperplastic polyps is constant regardless of age or population. This study also has several limitations. Even if a large baseline cohort, the numbers of follow-up hyperplastic polyps were relatively small. Second, single method to evaluate infection of H. pylori has a chance to give a false negative result.
In summary, H. pylori eradication induced the disappearance of hyperplastic polyps in National Cancer Screening Cohort. This study provides some evidences of H. pylori eradication in H. pylori-infected persons with hyperplastic polyps. We hope that this study contributes to an evidence of H. pylori eradication in patients with H. pylori-related gastric polyps.
KEY MESSAGE
1. Helicobacter pylori eradication induced the disappearance of hyperplastic polyp in National Cancer Screening Cohort.
2. Gastric polyp size was inversely associated with the disappearance of hyperplastic polyp.
3. Age and sex had no association with regression of hyperplastic polyps.
Notes
No potential conflict of interest relevant to this article was reported.