Acute Embolic Occlusion of the Left Common Iliac Artery Treated With Intra-Arterial Thrombolysis and Percutaneous Thrombectomy
Article information
Abstract
Acute embolic occlusion of the common iliac artery is a rare medical emergency that is not only limb-threatening, but also potentially life-threatening. Several treatment options exist for acute limb ischemia, although no treatment is clearly best. We report a case of acute embolic occlusion of the left common iliac artery in a patient with atrial fibrillation who was treated successfully using mechanical thrombectomy following intra-arterial thrombolysis.
INTRODUCTION
Acute embolic occlusion of a limb artery is a rare but serious medical emergency because acute limb ischemia is not only limb-threatening, but also potentially life-threatening. It requires prompt diagnosis and management. Surgery, local thrombolysis, percutaneous thrombectomy, and stenting have all been used to treat acute embolic limb ischemia, but the best treatment strategy remains controversial.
We report a case of acute embolic occlusion of the left common iliac artery in a patient with atrial fibrillation who was treated successfully with combined local thrombolysis and mechanical thrombectomy.
CASE REPORT
A 56-year-old woman was admitted to our hospital with sudden-onset pain, absent pulses, paresthesia, and pallor of the left lower extremity that had begun 10 hours before admission. She had been diagnosed with atrial fibrillation at another hospital 4 years before this presentation.
Computed tomographic (CT) angiography of the left lower extremity showed total occlusion of the proximal left common iliac artery (Fig. 1). Initially, we performed intra-arterial thrombolysis with urokinase 200,000 units for 1 hour. Follow-up angiography revealed antegrade flow with large residual thrombi (Fig. 2), so we decided to perform a percutaneous mechanical thrombectomy through the ipsilateral femoral artery using the OASIS™ thrombectomy system (Medi-Tech/Boston Scientific, Watertown, MA) (Fig. 3). Immediate post-procedural angiography demonstrated almost complete patency of the previously occluded artery. Follow-up CT angiography 14 days later showed a normal left common iliac artery (Fig. 4).
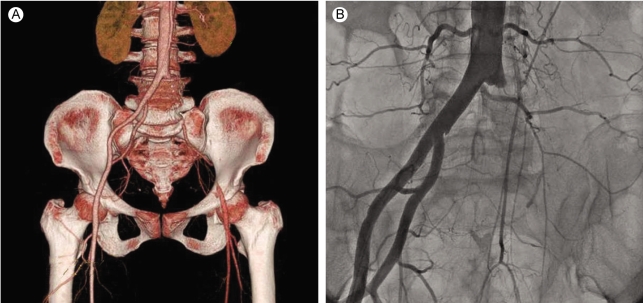
Immediate CT (A) and conventional angiography (B) on admission showed total occlusion of the proximal left common iliac artery.
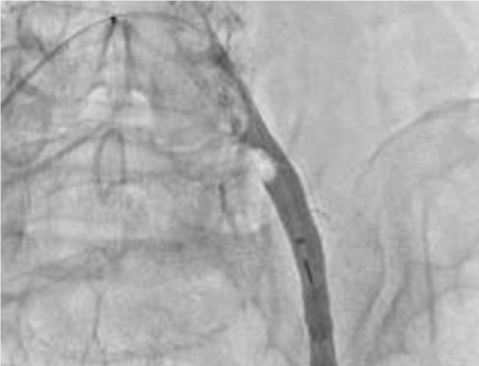
Follow-up angiography after initial intra-arterial thrombolysis using urokinase 200,000 units for 1 hour showed antegrade flow with large residual thrombi.

Percutaneous mechanical thrombectomy with the OASIS™ thrombectomy system through the ipsilateral femoral artery.
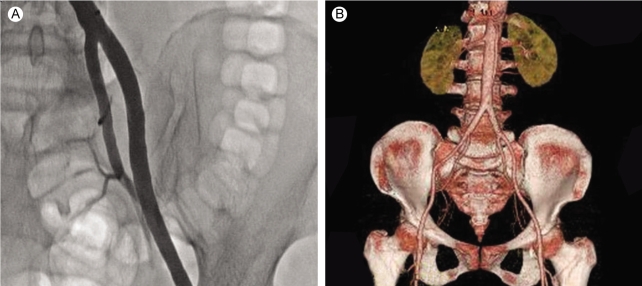
Immediate post-procedural angiography (A) and follow-up CT angiogram (B) after 2 weeks showed complete patency of the previously occluded artery.
The patient tolerated the procedures well with no complications and was clinically stable at the 9-month follow-up.
DISCUSSION
A recent epidemiologic study showed that peripheral artery obstruction occurs in 14 of every 100,000 people in the general population [1]. The most common cause of non-traumatic acute limb ischemia is embolism or thrombosis. The heart is the major source of emboli in patients with valvular disease with or without atrial fibrillation or ventricular mural thrombus after myocardial infarction. Thrombotic obstructions of the peripheral arteries are generally associated with atherosclerotic progression. However, differentiating these two pathologies clinically is difficult in most cases, and impossible in 10-15% of cases [2,3].
Classically, the symptoms of acute limb ischemia are dominated by the six Ps (pain, pallor, paralysis, poikilothermia, paresthesias, and pulselessness) or 'blue toe syndrome' [4]. Patients in whom acute limb occlusion is suspected are evaluated using digital subtraction angiography (DSA), duplex ultrasonography, CT angiography, and magnetic resonance angiography. Although DSA is regarded as the gold standard for limb ischemia imaging, CT angiography has recently come into wider use [5-7].
Various options have been proposed for the management of acute embolic limb ischemia. For years, surgical procedures such as embolectomy, bypass, and amputation were considered the gold standard treatment for total common iliac artery occlusion. However, early operative intervention has several procedural limitations and is characterized by a high mortality rate, with a 30-day mortality rate of 15-25% [8,9].
Randomized studies have shown that thrombolysis is generally as effective as surgery. Therefore, local thrombolysis has become a treatment modality in appropriately selected patients [10,11]. Moreover, several recent studies have reported that percutaneous mechanical thrombectomy has a high success rate, with low ampu-tation and mortality rates [12,13]. Primary endovascular stenting is not usually considered for the treatment of acute embolic limb lesions due to the fear of distal embolization [14]. Therefore, instead of using surgery or stenting, we decided to combine treatment with intra-arterial thrombolysis and percutaneous thrombectomy.
In conclusion, initial local thrombolysis followed by mechanical thrombectomy, as performed in this case, is an option for treating acute embolic occlusion of the common iliac artery.