Assessment of bone marrow involvement in patients with lymphoma: report on a consensus meeting of the Korean Society of Hematology Lymphoma Working Party
Article information
Abstract
In September 2011, the Korean Society of Hematology Lymphoma Working Party held a nationwide conference to establish a consensus for assessing bone marrow (BM) involvement in patients with lymphoma. At this conference, many clinicians, hematopathologists, and diagnostic hematologists discussed various topics for a uniform consensus in the evaluation process to determine whether the BM is involved. Now that the discussion has matured sufficiently to be published, we herein describe the consensus reached and limitations in current methods for assessing BM involvement in patients with lymphoma.
INTRODUCTION
The evaluation of bone marrow (BM) status is a key process in the initial workup of patients diagnosed with lymphoma. Despite its importance, the complexity of the BM evaluation process has sometimes caused institutional heterogeneity and may be an obstacle in multi-center clinical trials involving patients with lymphoma.
In September 2011, the Korean Society of Hematology Lymphoma Working Party held a nationwide conference to establish a consensus for assessing BM involvement in patients with lymphoma. At this conference, many clinicians, hematopathologists, and diagnostic hematologists discussed various topics for a uniform consensus in the evaluation process to determine whether the BM is involved. It is now considered to have become sufficiently mature to be published. Hence, in this report, we describe the consensus reached and the limitations in current methods for assessing BM involvement in patients with lymphoma.
IMPORTANCE OF A BONE MARROW EXAMINATION IN LYMPHOMA
The BM is the most common site of extranodal involvement in lymphoid malignancies and the frequency of BM involvement varies according to the lymphoma subtype (Table 1). Compared to aggressive lymphoma, relatively high frequencies have been reported in indolent lymphomas, such as mantle cell lymphoma (MCL), follicular lymphoma (FL), and marginal-zone lymphoma [1]. Because BM involvement of lymphoma is definite evidence of disseminated disease [2,3], the assessment of BM status in patients with lymphoma provides important information for decisions regarding treatment. In particular, in the subtypes of lymphoma in which local treatment modalities, such as radiotherapy and concurrent chemoradiation, have a role in definitive therapy, knowledge about the presence or absence of BM involvement is vital. Hodgkin lymphoma, FL, mucosa-associated lymphoid tissue (MALT) lymphoma, and extranodal NK/T cell lymphoma, nasal type, are examples [4,5].
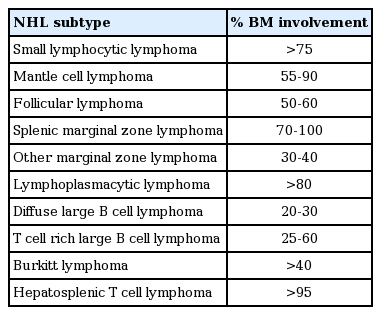
Incidence of bone marrow involvement in non-Hodgkin lymphoma
Currently, noninvasive clinical staging by computed tomography (CT), magnetic resonance imaging (MRI), or positron emission tomography (PET)-CT cannot fully assess BM involvement, which is possible only by pathological staging (aspiration and trephine biopsy). Thus, although clinical stage can suggest localized diseases (stage I or II), it is not uncommon for the final stage to change to stage IV due to positive BM involvement. For example, recent studies that have analyzed patients with MALT lymphoma have demonstrated that a considerable proportion of patients (10% to 44%) shows BM involvement despite single MALT organ disease [6-8].
Determining BM status is important for the prognosis of patients. The International Prognostic Index (IPI) consists of five clinical variables: age, serum levels of lactate dehydrogenase (LDH), performance status (PS), stage, and extranodal involvement. Of these, BM status can influence both stage and extranodal involvement. If a patient of clinical stage IE (e.g., gastric lymphoma) has only one positive variable among age, serum LDH, and PS, the prognosis may depend mainly on the BM status. With no BM involvement, the IPI score would be 1 and this patient would be in the low-risk group. In contrast, positive BM involvement makes the IPI score 3, placing the patient in the intermediate-high risk group. According to the IPI system, the low-risk group shows a response rate of 87%, 70% 5-year relapse-free survival, and 73% 5-year overall survival. However, the intermediate-high risk group shows a response rate of 55%, 49% 5-year relapse-free survival, and 43% 5-year overall survival [9]. A recent trial suggested that frontline autologous stem cell transplantation may provide clinical benefits to high-risk patients with aggressive non-Hodgkin lymphoma (NHL) compared to low-risk patients [10,11].
ROLE OF MORPHOLOGY AND IMMUNOHISTOCHEMICAL ANALYSES
The pattern of infiltration is a key morphological feature to consider when generating a logical list of differential diagnostic considerations. These infiltration patterns, although not absolutely specific, may provide diagnostic clues both for the discrimination of benign and malignant infiltrates and for NHL subtyping. However, patterns can change during the course of the disease, and mixed patterns frequently occur. Five major patterns of BM infiltration can be discerned (Table 2) [12].

Patterns of lymphomatous bone marrow
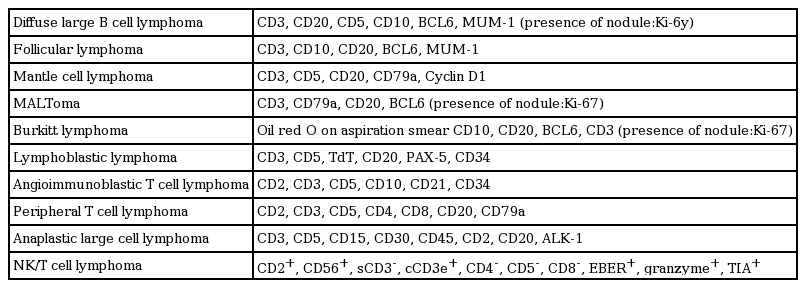
Nevertheless, the morphological features of lymphoma in BM involvement vary widely and frequently differ from these typical patterns. Particularly in cases with individual infiltration of lymphoma cells, it can be difficult to recognize the involvement of lymphoma in BM. Moreover, the histological features of BM involvement are sometimes discordant with those of extramedullary lesions. Thus, in addition to a morphological assessment, immunohistochemical studies are required for a complete diagnostic approach. Features of the morphological, immunohistochemical, and diagnostic clues are summarized in Tables 3 (B-NHL) and 4 (T-NHL) [12].
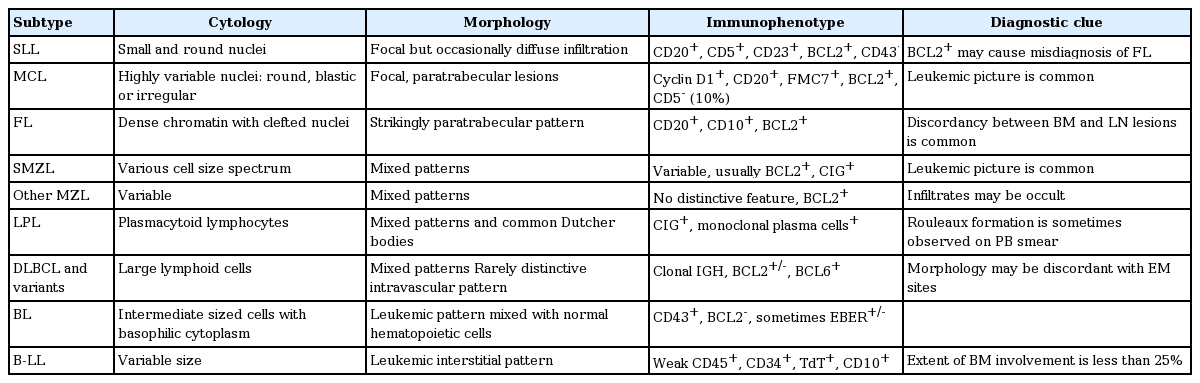
B cell non-Hodgkin lymphomas in the bone marrow

T cell non-Hodgkin lymphoma in bone marrow
Small B cell NHLs
Small B cell NHLs include chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), lymphoplasmacytic lymphoma (LPL), FL, MCL, and marginal-zone lymphoma. They frequently involve the BM and make up a large percentage of cases of BM infiltrates in patients with lymphomas.
CLL/SLL is usually of B cell origin and involves the BM and peripheral blood. The involved BM is usually hypercellular, with interstitial, nodular, and mixed or diffuse infiltration of small neoplastic lymphocytes with clumped chromatin and scanty cytoplasm. Proliferation centers with larger cells are less common than in lymph nodes. Immunohistochemically, the tumor cells are positive for CD19, CD20, CD79a, CD23, CD5, and CD43 but negative for cyclin D1 [13-15].
MCL involves the BM in 55% to 90% of cases and can show various patterns, including predominantly paratrabecular infiltrates with a uniform population of small to medium-sized lymphocytes having cleaved or angular nuclei, dispersed chromatin, inconspicuous nucleoli, and scant cytoplasm [16]. The tumor cells usually express surface immunoglobulin M (IgM), CD19, CD20, CD22, CD79a, CD5, CD43, and characteristically, cyclin D1. Demonstration of the characteristic CD5+/CD23– immunophenotype and of cyclin D1 expression, complemented by CD20 staining, is very sensitive for the detection of residual disease. Blastoid and pleomorphic variants of MCL have to be distinguished from lymphoblastic lymphoma (LL)/acute leukemia and large-cell lymphoma [12].
Low-grade FLs show BM involvement in 50% to 60% of cases. In the BM, FL cells are characteristically localized in the paratrabecular region, but may infiltrate interstitially with significant fibrosis and be virtually invisible in an ordinary morphological examination. The follicular growth pattern, which is typical in lymph nodes, is only seen rarely. Immunohistochemically, the lymphoma cells are positive for surface Ig, CD19, CD20, CD22, CD79a, bcl2, bcl6, and CD10, and negative for CD5 and CD23 [17].
Nodal and extranodal marginal zone lymphomas (MZLs) infiltrate the BM less frequently than in other small B cell NHLs, possibly with a higher frequency for nodal MZL. They usually show intertrabecular, nodular infiltrates, which may contain reactive germinal centers [16]. Central nodules and patchy or more diffuse infiltration may be observed, but the histology of the BM alone is usually not diagnostic [18].
LPL is most often encountered in the presence of the clinical syndrome of Waldenstrom’s macroglobulinemia, with the presence of an IgM paraprotein and BM involvement. Histologically, the BM shows variably distributed, often interstitial and diffuse patterns of small lymphocytes, lymphoplasmacytoid cells, and plasma cells with variable fibrosis [16].
High-grade B cell NHL
Diffuse large-cell B cell lymphoma (DLBCL) has a low f requency of BM infiltration and the patterns of infiltration are highly variable, ranging from subtle, focal infiltrates to a packed marrow with complete replacement of hematopoiesis [16]. The BM is infiltrated by a heterogeneous cell population, including large neoplastic cells with vesicular nuclei, prominent nucleoli, basophilic cytoplasm, and frequent mitotic figures. The tumor cells may express germinal center-type immunophenotypes, such as CD10+ or CD10–/BCL6+/MUM1–, or activating B cell-like (non-germinal center)-type, such as CD10–/BCL6+/MUM1+ or CD10–/BCL6– [19,20]. So-called discordant infiltrates, meaning small neoplastic cells in BM with DLBCL at another site, have been reported to be associated with a better prognosis than concordant BM infiltration [21].
T-cell/histiocyte-rich large B-cell lymphoma (TCRBCL) is another distinctive type of DLBCL with unique features in the BM. Similar to extramedullary disease, BM infiltrates in TCRBCL show a predominance of non-neoplastic T cells and variable numbers of histiocytes. Neoplastic large B cells are typically infrequent and overall morphological features overlap with peripheral T cell lymphoma (PTCL) and Hodgkin lymphoma. The CD20+, EMA+, CD30–, and CD15– phenotype of the neoplastic large cells helps to distinguish TCRBCL from Hodgkin’s lymphoma [12,17].
BM involvement in Burkitt lymphoma (BL) ranges from scattered interstitial foci to complete replacement of the normal marrow elements by medium-sized blasts with inconspicuous nucleoli, basophilic cytoplasm, and sometimes, a “starry sky” pattern, due to numerous mitotic figures. Necrosis is frequent [18]. BL shows a mature B cell phenotype with coexpression of surface IgM, CD20, CD10, and BCL6, but lacks CD5, BCL2, and TdT [12].
B-LL and leukemia are biologically related disorders that differ only in terms of disease distribution. B-LLs predominate outside the BM and cases with < 25% BM infiltration are arbitrarily designated lymphomas, whereas cases with > 25% neoplastic cells in the BM are termed leukemias [12]. BM involvement in B-LL shows patchy interstitial infiltrates of lymphoblasts and this may be morphologically subtle due to their admixture with normal hematopoietic cells. Immunohistochemical staining and flow cytometric immunophenotyping may be essential to detect occult neoplastic cells. The neoplastic lymphoblasts are slightly larger than lymphocytes, with round or convoluted nuclei, fine chromatin, inconspicuous nucleoli, and scant, faintly basophilic cytoplasm. Mitotic figures are common. The blasts usually pack the marrow spaces but occasionally infiltrate patchily. Lymphoblasts are strongly reactive for TdT and CD34 immunohistochemical stains. In addition to typical B cell markers, B-LLs are frequently positive for CD10 [17,18].
T cell NHLs
Neoplastic T cells frequently produce systemically acting cytokines. The BM may be the site of a cytokine response even in cases in which the lymphoma itself does not involve the BM. Indeed, florid BM hemophagocytic syndromes often result from systemic cytokine-mediated histiocyte activation [12].
Angioimmunoblastic T cell lymphoma (AITL) in BM shows polymorphic, sparsely admixed, large atypical cells in a background of abundant non-neoplastic cells. Increased neoangiogenesis and reticulin fibrosis are common, but characteristic arborizing vasculature in the lymph node is rarely observed. The presence of large, transformed, EBV-positive B cells in the infiltrate may point to a diagnosis of AITL, but can also lead to confusion with TCFBCL or Hodgkin lymphoma [16]. The tumor cells are usually reactive to immunohistochemical staining for CD2, CD3, CD4, CD5, CD7, and CD10. PD1 and CXCL13 are also expressed in neoplastic T cells. However, detection of CD10+ neoplastic cells in BM can be difficult, and the diagnosis of AITL usually requires a biopsy of an extramedullary lesion, particularly a lymph node [12,18].
In BM involvement in PTCL not otherwise specified (NOS), interstitial or paratrabecular infiltration is common. The infiltration is polymorphic, similar to an extramedullary lesion, with variable numbers of small, medium, and large neoplastic lymphoid cells admixed with eosinophils and histiocytes, which may mask the underlying lymphoma. Occasional Reed-Sternberg-like cells may be present [17]. Because BM involvement in PTCL-NOS is observed in up to 40% of cases, a careful examination is required. Although discrete foci predominate, subtle interstitial infiltrates may be encountered, which can be overlooked in a morphological review, and thus immunohistochemistry is essential in such cases. Immunohistochemically, the neoplastic lymphoid cells are usually positive for T cell markers such as CD3, CD2, CD5, and CD7. However, some T cell markers may be aberrantly deleted. Sometimes, it can be difficult to decide whether the T cells are truly neoplastic in interstitial involvement in T cell lymphoma even with molecular and/or immunohistochemical studies [18].
Anaplastic large lymphoma cells in BM core biopsy sections are often dispersed individually among benign hematopoietic cells [16]. Large neoplastic cells with abundant cytoplasm, large pleomorphic kidney-shaped nuclei, and multiple, prominent eosinophilic nucleoli grow in a cohesive pattern. Immunohistochemical assessments of CD30 and anaplastic lymphoma kinase are essential for detecting morphologically subtle infiltrates [12].
Although mycosis fungoides rarely involves the BM, even in patients with advanced disease or Sézary syndrome, helper T cells with small, convoluted, or cerebriform nuclei can infiltrate the BM with no characteristic pattern. Immunohistochemically, they are positive for CD2, CD3, CD5, CD7 (in ~30% of cases), and CD4, and negative for CD25 [12].
BM in acute lymphoblastic leukemia/lymphoma of T cell origin is morphologically similar to B-LL/leukemia, typically characterized by a massive, diffuse infiltrate of monomorphic blasts with greatly reduced hematopoiesis. Immunohistochemistry for TdT, which is usually strongly positive in the nuclei of blasts, CD99, CD3, CDIa, and T cell markers can aid the determination of the cell lineage and help discriminate it from other neoplasms [16].
Hodgkin lymphoma
BM involvement in Hodgkin lymphoma is uncommon; it is seen in only 5% of patients [22,23]. For a reliable morphological evaluation, generous BM trephine biopsy specimens of 1 to 2 cm in length and multiple-step sectioning are required. The histological features of Hodgkin lymphoma subtypes are usually indistinguishable. Focal fibrosis and abnormal mononuclear cells may be a diagnostic clue, but classic Reed-Sternberg cells may not be present [24]. The neoplastic cells in classic Hodgkin lymphoma are immunohistochemically positive for CD30 and CD15, and negative for CD45 and CD20. The lymphocytic and/or histiocytic cells of nodular lymphocyte-predominant Hodgkin lymphoma are CD20+, CD30–, and CD15– [17,18].
Recommendations for immunohistochemical profiles for the evaluation of BM involvement in lymphoma
A BM biopsy is considered positive for lymphoma involvement in the presence of lymphoid substitution of normal BM hematopoietic cells; the percentage of BM involvement is calculated as the extent of the lymphoid population versus the whole BM cellularity, and the patterns of infiltration are known and immunohistochemistry profiles can be applied according to the morphology of neoplastic lymphoid cells or a pathological diagnosis at extranodal sites (Table 5).
Recommendation of immunohistochemistry profiles for the evaluation of bone marrow involvement of lymphoma
There are some diagnostic challenges in the evaluation of BM in patients with lymphoma. The first issue is the distinction between reactive nodular lymphoid infiltrates and nodular infiltrates of the lymphoma. This is a common diagnostic problem in BM trephines in patients with low-grade lymphomas. Such reactive infiltrates can be found in various disorders, including aging, autoimmune diseases, infections, and myeloproliferative neoplasms. A more mixed cellular composition, well-defined borders, an intertrabecular location, a low number of infiltrates, and the absence of reticulin fibrosis are morphological features that are more commonly found in benign lymphoid nodules. Germinal centers are relatively rare in benign infiltrates. Immunophenotyping usually shows a predominance of T cells and a lack of aberrant markers and immunoglobulin light chain restriction [16].
Second, in cases of aberrant expression in nodal lesions, aberrantly expressed antigens can provide diagnostic clues for evaluating the BM. Peripheral T cell lymphoma is a typical example of this; most peripheral T cell lymphoma patients present with aberrant expression in peripheral lymph nodes. This is usually characterized by downregulation of CD5 and CD7, with a predominant CD4+/CD8– phenotype. CD4/CD8 double positivity or double negativity is sometimes seen in the absence of a follicular T helper cell phenotype (CD10+, BCL6+, PD1+, and CXCL13+). Aberrant expression of CD20, CD79a, and/or CD30 have also occasionally been observed [25].
ROLE OF FLOW CYTOMETRY
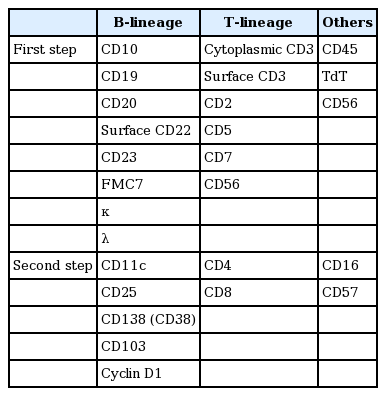
Flow cytometry is useful and may be essential for the diagnosis of leukemic manifestations of a lymphoma. The leukemic phase indicates lymphoma cells ≥ 25% among nucleated cells in the peripheral blood or BM aspirate [25]. Usually, lymphoma cells are gated as CD-45bright/side-scattered light (SSC)low by flow cytometry, but immature lymphoid cells are CD45intermediate or negative, TdT+, and CD34+. The lineage markers on lymphocytes are CD19 for the B cell lineage, CD3 for the T cell lineage, and CD56 for the NK cell lineage. According to European LeukemiaNet, the B-oriented panel includes CD19+ cells with other markers such as CD5, CD20, CD22, CD23, CD103, CD10, κ and λ light chains, surface Ig, CD25, CD79b, and CD38; the T-oriented panel includes CD3+ cells with other markers such as CD2, CD4, CD5, CD8, and CD7; and the NK-oriented panel includes CD56+ cells with other markers such as CD16, CD57, CD45, CD158, CD94, and cytotoxic granule-associated proteins (TIA-1, granzyme-B, perforin) as an activated cytotoxic phenotype [26]. Analyses of leukemic BM involvement in Korean patients with NHL have shown that the leukemic phase is associated with a poor prognosis, such as low complete remission, low 5-year survival rate, and a high death rate [27].
Recently, EuroFlow suggested eight-colored antibody panels for standardized n-dimensional flow cytometric immunophenotyping of normal, reactive, and malignant leukocytes. The lymphoid screening tube detects aberrant mature lymphocyte populations of B, T, and NK lineages, but this eight-color tube does not allow the precise diagnosis and classification of the aberrant lymphocyte populations detected. This needs further characterization with plasma cell dyscrasia, B-chronic lymphoproliferative disease (B-CLPD), T-CLPD, and NK-CLPD panels [28].
In February 2006, the Korean Society of Diagnostic Hematology recommended a minimum antibody panel for the diagnosis and classification of CLPDs [29]. Recently, this recommendation was modified, considering recent progress in the flow cytometric analysis of lymphoid malignancies (Table 6). After gating on CD45bright/SSClow, combinations of κ/λ/CD20 (or CD19)/CD45, CD5/CD10/CD20 (CD19)/CD45, or CD4/CD8/CD3 (CD7)/CD45 are useful for the interpretation of flow cytometric results. For example, because a mature B cell lymphoma shows immunoglobulin light chain restriction, the antibody combination of κ/λ/CD19 (or CD20)/CD45 is useful. To see aberrant antigen expression, the combination of CD5/CD10/CD19 (or CD20)/CD45 is also useful. In the panel of CD5/CD10/CD19 (or CD20)/CD45, after the serial gating of CD45+bright/low and CD19 (or CD20)+ gating, the flow cytometric cytograms of CD5+ CD10–, CD5– CD10+, CD5+ CD10+, and CD5– CD10– patterns indicate specific subtypes of mature B cell lymphomas. Mature T&NK cell lymphomas frequently show aberrant T cell antigen expression, such as a lack of pan-T antigens (CD5, CD7). To identify the restricted populations of T cells, the antibody combination of CD4/CD8/CD3/CD45 is used, and serial gating of CD45+bright/low and CD3+ identify specific subtypes of mature T&NK cell lymphomas such as CD4+ CD8–, CD4– CD8+, CD4+ CD8+, and CD4– CD8– patterns. The immunophenotypes of the specific subtypes of lymphoid malignancies are summarized in Tables 7 and 8.
Minimum antibody panel for diagnosis of chronic lymphoproliferative diseases
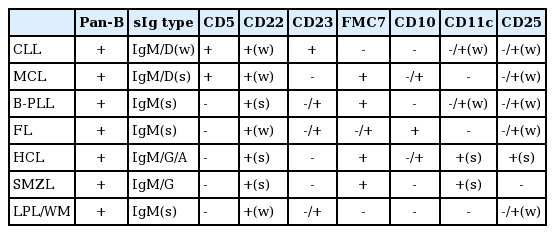
Immunophenotypes of B cell lymphoid malignancies
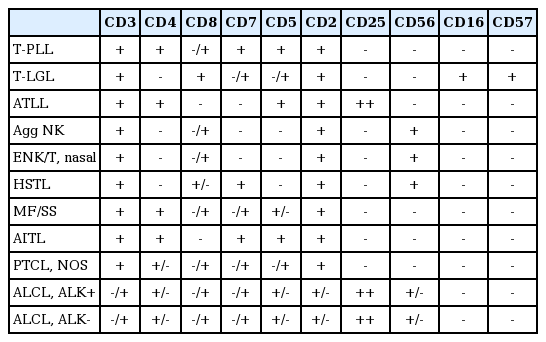
Immunophenotypes of T cell and NK cell lymphoid malignancies
ROLE OF CYTOGENETIC ANALYSES
Cytogenetic analyses can provide important information for discriminating lymphomatous BM and predicting prognoses in certain types of lymphoma. For example, del(11q) or del(17p) in CLL indicate a worse prognosis, and thus aggressive treatment such as allogeneic stem cell transplantation should be considered early in the course of therapy. Fluorescence in situ hybridization (FISH) is particularly useful for detecting clonal lymphoma cells in BM. Types of probes for FISH that are validated and of clinical importance are summarized in Table 9.
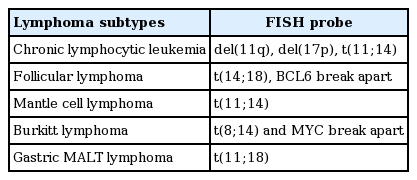
Types of probe for fluorescence in situ hybridization
ISSUES TO BE INVESTIGATED
Currently, a pathological examination does not assess the whole BM and the interpretation of a BM specimen usually requires a highly experienced hematopathologist. Although the revised response criteria for malignant lymphoma, published in 2007, indicates that uninvolved BM should be normal histologically with a small (< 2%) clonal B cell population detected by flow cytometry [30], there are still some diagnostic challenges.
First, the differential diagnosis of reactive lymphoid infiltrates from nodular infiltrates of low-grade lymphomas remains a common problem. Although some diagnostic clues based on morphology have been suggested [16,31], some cases may remain unresolved. To clarify this uncertainty, molecular studies using DNA- or RNA-based polymerase chain reaction should be considered. Although this technique still does not cover the whole range of problems, it should be considered whether some proven tests, such as immunoglobulin heavy chain gene rearrangement analysis and T cell receptor analysis, should be involved in the standard. The next issue associated with BM morphology concerns the clinical meaning of concordance with the morphology of the lymphoma cells in the lymph node. In patients with DLBCL, some have shown infiltrates of small B cell lymphoma cell in BM, instead of large B cells (discordant involvement). Under this condition, it is presumed that DLBCL developed as a transformation from an occult small B cell lymphoma, or alternatively, two unrelated lymphomas are present [21]. Recently, it has been reported that in multivariate analyses, including individual factors of the IPI system, concordant BM involvement has an independently negative impact on prognosis whereas discordant BM involvement does not [32]. If this can be validated in a prospective cohort, the morphology of lymphoma cells in BM involvement should be considered when predicting prognosis in patients with DLBCL.
Another issue is flow cytometry analyses. As mentioned above, flow cytometry is essential when assessing BM involvement. Current guidelines regard a small clonal population (< 2%) as uninvolved BM [30]. However, to the best of our knowledge, no clinical study has addressed this issue. Moreover, recent advances in flow cytometry technology have caused a wide range of variation in the sensitivity of flow cytometric analyses among institutions. Thus, it is desirable to document the minimal criteria for flow cytometry technology in a standard guideline. The last issue in flow cytometry is the meaning of discordance between a bone marrow biopsy (BMB) and flow cytometry. Recently, in a study that included 757 NHL patients, there was considerable discordance between BMB and flow cytometry [33]. For example, in FL and LPLs, the discordance rates were up to 22% and 24%, respectively. Based on BMB and flow cytometry results, four subsets can be created in patients with NHL: positive BMB and positive flow cytometry, positive BMB and negative flow cytometry, negative BMB and positive flow cytometry, and negative BMB and negative flow cytometry. To date, no study has analyzed the prognostic significance of each group. It could be valuable to investigate whether there are prognostic differences among these subgroups. Moreover, the relationship between prognosis and the degree of involvement remains unclear. Although some retrospective analyses have revealed significant correlations between degree of BM involvement and prognosis [34-37], this has not been validated. To clarify this issue, it is important to establish uniform criteria for quantifying the degree of BM involvement objectively, so as to minimize differences among interpreting pathologists.
Finally, we discuss whether BM status can be evaluated by clinical staging using CT, MRI, or PET-CT. Because of technical limitations of these imaging modalities, BM assessment is currently possible only by a pathological examination. Because a BM biopsy at multiple sites is impossible in routine clinical practice, hematopathologists and clinicians have accepted results from BM examinations at the iliac crest on the assumption that this area may reflect whole BM status. However, technical advances in imaging modalities have shown that this is not true. A recent prospective study that compared the performance of BMB, whole-body MRI, and PET-CT to evaluate lymphomatous BM invasion demonstrated that noninvasive morphological procedures could be superior to a pathological BM examination [38]. In that study, most patients with abnormal BM findings on MRI or PET-CT showed BM infiltration in areas other than the iliac crest. Recently, resolution and sequence protocols of MRI have made rapid progress, sufficient to detect lymphomatous BM invasion [39]. Usually, MRI is considered to have high sensitivity, but specificity may be suboptimal for assessing lymphomatous BM invasion [40]. Nevertheless, it is expected that ongoing advances in technical aspects will make it possible to assess BM status by imaging without a pathological exam. Moreover, it is considered that PET-MRI, a new, developing imaging modality combining PET and MRI, may be promising for BM evaluations and applicable in the near future [39].
CONCLUSIONS
BM involvement in patients with lymphoma provides important information in clinical practice. Despite the limitations of current BM evaluation methods, standardization of the BM evaluation process is important to improve patient care. Based on standardized protocols, discussions about how to define positive lymphomatous BM should be in progress. Furthermore, because recent technological advances in flow cytometry and imaging modalities are expected to impact clinical practice in the near future, interdepartmental collaboration including the areas of medicine, hematopathology, radiology, and nuclear medicine is more important than ever.
Notes
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This work was supported by the Korean Society of Hematology Lymphoma Working Party.