Differentiation between polycystic ovary syndrome and polycystic ovarian morphology by means of an anti-Müllerian hormone cutoff value
Article information
Abstract
Background/Aims
Although increased serum anti-Müllerian hormone (AMH) level has been suggested to be a surrogate marker of polycystic ovarian morphology (PCOM), its association with polycystic ovary syndrome (PCOS) is controversial, and its diagnostic value has not been determined. We aimed to observe the relationship between the AMH level and PCOS phenotypes and to determine the optimal cutoff value of AMH for the diagnosis of PCOS in young Korean women.
Methods
We recruited 207 women with PCOS (120 with PCOM and 87 without PCOM) and 220 regular cycling women with normoandrogenemia (100 with PCOM and 120 without PCOM). Subjects underwent testing at a single outpatient visit. Serum AMH level was measured.
Results
Women with PCOS had higher serum AMH levels than did regular cycling women with normoandrogenemia (p < 0.05). Women with PCOM had higher serum AMH levels than women without PCOM, regardless of PCOS status (p < 0.05). The optimal AMH cutoff value for the diagnosis of PCOS was 10.0 ng/mL (71% sensitivity, 93% specificity). Serum AMH was an independent determinant of total testosterone after adjustment for age, body mass index, and the number of menses/year (β = 0.31, p < 0.01). An association between AMH and hyperandrogenism was only observed in women with PCOS, and it was independent of the presence of PCOM.
Conclusion
The serum AMH level can be useful for the diagnosis of PCOS at any age less than 40 years, and the optimal cutoff value for the diagnosis of PCOS identified in this study of young Korean women was 10.0 ng/mL.
INTRODUCTION
Polycystic ovary syndrome (PCOS), which is the most common endocrine disorder in reproductive-aged women, affects 6% to 10% of premenopausal women [1]. The diagnosis of PCOS is based on a combination of clinical, biochemical, and ultrasound criteria, and the main diagnostic criteria of PCOS are polycystic ovarian morphology (PCOM), oligo-anovulation, and hyperandrogenism (HA) [2]. However, the diagnosis of PCOS can be subjective, because counting the ovarian follicular number and measuring the ovarian volume using ovarian ultrasound are technique-dependent and because obtaining standardized measurements is difficult. The number of follicles and the size of the ovary measured by ovarian ultrasound may overlap in women with and without PCOS, and PCOM has been reported frequently in women without PCOS [3]. Moreover, there is currently no consensus on the most appropriate androgen to measure for PCOS diagnosis, and diverse androgen cutoff values have been suggested for the determination of biochemical hyperandrogenemia and diagnosis of PCOS because direct immunoassay methods can be highly inaccurate for the measurement of testosterone when its level is at the lower end of the female range [4].
Anti-Müllerian hormone (AMH) is secreted by granulosa cells and small antral and preantral follicles [5]. Serum AMH levels were markedly increased in women with PCOS and were positively related with small antral follicle number [6,7]. The AMH level has been reported to be independently related to HA and PCOM [8] and to be strongly associated with the main phenotypic features of PCOS, including ovulatory dysfunction [9,10]. Therefore, increased serum AMH level has been suggested as an objective surrogate marker for the diagnosis of PCOS and has been shown to be correlated with conventional diagnostic criteria [9,11].
It is difficult to determine the optimal AMH cutoff value for the diagnosis of PCOS because the age-related decline in antral follicle number is reflected by AMH concentration. A variety of AMH cutoff values for predicting PCOS have been proposed in previous studies [12,13]. In the same age group, the serum AMH level was higher in PCOS women than in those without PCOS, and age-specific AMH cutoff values for Chinese women with and without PCOS have been suggested [14]. In addition, an AMH Z-score, the level of AMH relative to the expected mean and standard deviation for a particular age, was proposed to adjust for the age-related decline in the number of antral follicles [15]. The aim of this study was to observe the relationship between the AMH level and PCOS phenotypes and to determine the optimal AMH cutoff value for the diagnosis of PCOS in young women.
METHODS
Subjects
Between 2008 and 2010, we performed a survey of the menstrual health of young women under 40 years of age living in Seoul, Korea. Participants were recruited using newspaper and online advertisements. We enrolled 207 women with PCOS and 220 regular cycling women with normoandrogenemia. As proposed at the European Society for Human Reproduction and Embryology (ESHRE) [2], PCOS was diagnosed when two or more of the following three criteria were met: oligo- or anovulation, HA, and polycystic ovaries. Oligomenorrhea (OM) was defined as having fewer than eight menstrual cycles per year. Biochemical hyperandrogenemia was defined as a total testosterone level or free testosterone level above the 95th percentile (total testosterone ≥ 67 ng/dL or free testosterone ≥ 0.84 ng/dL) for testosterone levels in healthy women with regular menstrual cycles [16]. Clinical HA was defined as hirsutism with a modified Ferriman-Gallwey score of ≥ 3 [17]. HA included biochemical hyperandrogenemia and/or clinical HA. One of the following two criteria must be met for the diagnosis of PCOM: visualization of ≥ 12 follicles/ovary that measure 2 to 9 mm in diameter or an ovarian volume of > 10 cm3 identified by transvaginal ultrasonography or transrectal ultrasonography with a distended bladder for virginal women. Patients with similar clinical presentations, such as congenital adrenal hyperplasia, androgen-secreting tumors, and Cushing’s syndrome, were excluded from the study. Patients with 21-hydroxylase-deficient nonclassic adrenal hyperplasia were excluded based on the basal morning level of 17-hydroxyprogesterone. Subjects were excluded if they had been on medication (e.g., steroids, oral contraceptives, metformin, or thiazide diuretics) within 3 months of the evaluation or had used other drugs that could affect basal parameter status. Subjects were excluded if they had menstrual irregularities or clinical signs of HA compared to regular cycling women with normoandrogenemia. We divided the subjects based on the presence of PCOS and PCOM. Among the women with PCOS, 120 had PCOM (group 1, HA + OM + PCOM) and 87 did not have PCOM (group 2, HA + OM). Among the regular cycling women with normoandrogenemia, 100 had PCOM (group 3, PCOM), and 120 did not have PCOM (group 4, control). The subjects were divided into five groups according to age: < 20, 20 to 24, 25 to 29, 30 to 34, and ≥ 35 years. Written informed consent was obtained from all participants, and the Institutional Review Board of Ewha Womans University Mokdong Hospital approved this study.
Methods
Weight and height were measured with the subjects wearing light clothing and no shoes; body mass index (BMI) was also calculated (kg/m2). Waist circumference was measured to the nearest 0.1 cm on bare skin during mid-respiration at the narrowest indentation between the 10th rib and the iliac crest.
On the third day of the follicular phase of the menstrual cycle, a venous blood sample was obtained from each subject after an overnight fast of at least 8 hours. In women with amenorrhea, the blood samples were obtained on a random day. Total testosterone levels were measured via the chemiluminescent immunoassay method using a commercially available kit (Siemens, New York, NY, USA, mean inter- and intra-assay coefficient of variation (CV) of 4.4% and 6.2%, respectively). Sex hormone-binding globulin (SHBG) levels were measured by immunoradiometric assay using a commercially available kit (DPC, Los Angeles, CA, USA, mean inter- and intra-assay CVs of 7.9% and 5.3%, respectively). Free testosterone levels were calculated using the formula available on the International Society for Study of the Aging Male (ISSAM) web site, which is based on total testosterone, SHBG, and albumin levels obtained in the same sample from each subject. Serum AMH level was measured by enzyme-linked immunosorbent assay using a commercially available kit (Beckman Coulter, Chaska, MN, USA, mean inter- and intra-assay CVs of 4.5% and 3.6%, respectively). Serum AMH levels were compared between the five age groups.
Ultrasound examinations were performed with a 7 MHz transvaginal (or transrectal for virginal women) transducer (Logic 400 General Electric, GE Medical Systems, Milwaukee, WI, USA). Ovarian volume was calculated according to a simplified formula for an ellipsoid (0.5 × length × width × thickness) [18]. Ovarian volume was defined as the average volume of both ovaries, and the ovarian follicle number was defined as the average number of follicles in each ovary.
Statistical analysis
The statistical analyses were performed using the SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). The Kolmogorov-Smirnov statistic was used to analyze continuous variables for normality. Quantitative variables were reported as the mean ± standard deviation. Variables with skewed deviations were reported as medians and interquartile ranges. Group mean values were compared using one-way analysis of variance. All other data were evaluated by one-way Kruskal-Wallis variance analysis with post hoc pair-wise comparisons using Bonferroni’s corrected Mann-Whitney U test. The age-adjusted partial correlation analysis was used to determine the relationships between AMH level and the various parameters. Multiple linear regression analyses were performed to determine the independent association between AMH levels and total testosterone after controlling for age, BMI, and the number of menses/year. A multiple logistic regression analysis was used to assess the association between AMH levels and the presence of PCOS. A receiver-operating characteristic curve was constructed to evaluate the sensitivity and specificity of AMH level for the prediction of PCOS. A p < 0.05 was considered statistically significant.
RESULTS
The clinical, biochemical, and ultrasound data of the four groups (group 1, HA + OM + PCOM; group 2, HA + OM; group 3, PCOM; and group 4, control) are summarized in Table 1. Serum AMH level was the highest in group 1, intermediate in groups 2 and 3, and lowest in group 4. Serum AMH in group 1 was significantly higher than in the three other groups (all p < 0.05). The serum AMH levels in group 2 and group 3 were similar to each other but were significantly higher than that of group 4 (p < 0.05). The values of age, BMI, and waist circumference did not differ significantly among the four groups (all p > 0.05). Women with PCOS had higher values of total testosterone and free testosterone and lower values of SHBG and number of menses/year than did regular cycling women (all p < 0.05). The values of ovarian volume and follicle number were highest in group 1, intermediate in group 3, and lowest in groups 2 and 4 (all p < 0.05).
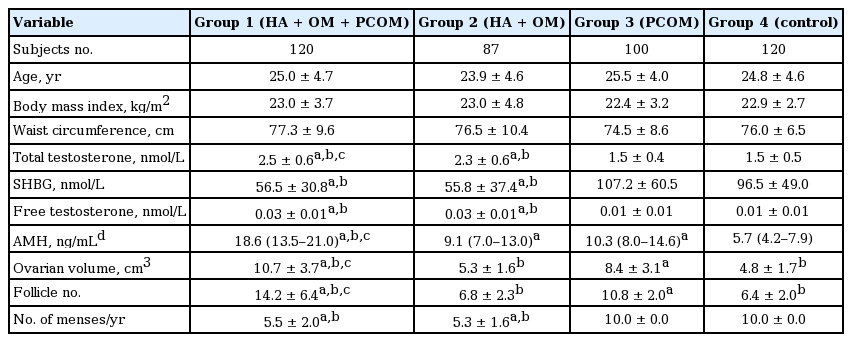
Clinical, biochemical, and ultrasound data of subjects
The serum AMH level was positively correlated with total testosterone (r = 0.33), free testosterone (r = 0.16), ovarian volume (r = 0.57), and follicle number (r = 0.39) after adjustment for age in women with PCOS (groups 1 and 2, all p < 0.05). In regular cycling women without PCOS, serum AMH level was also positively correlated with ovarian volume (r = 0.24) and follicle number (r = 0.47, all p < 0.05) but was not correlated with total or free testosterone (groups 3 and 4) (Table 2).
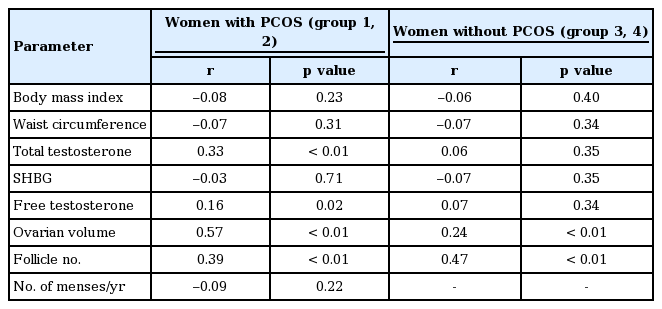
Partial correlation analysis between anti-Müllerian hormone levels and the various parameters after adjustment for age
AMH level was significantly positively correlated with total testosterone (r = 0.208 and r = 0.347) and ovarian volume (r = 0.329 and r = 0.473) in women with PCOS, regardless of the presence of PCOM and was significantly positively correlated with ovarian volume (r = 0.334) and follicle number (r = 0.441) in regular cycling women without PCOM. AMH level was not significantly correlated with ovarian volume and follicle number in regular cycling women with PCOM (Table 3).
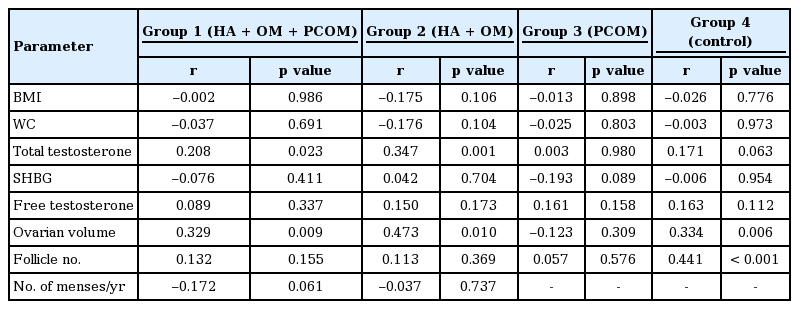
Partial correlation analysis between anti-Mullerian hormone levels and the various parameters after adjustment for age
The multiple linear regression analyses showed that serum AMH was an independent determinant of total testosterone after adjustment for age, BMI, and the number of menses/year (β = 0.31, p < 0.01) in women with PCOS (Table 4). AMH was also shown to be the strongest predictor of PCOS by multiple logistic regression analysis (odds ratio, 1.29; 95% confidence interval [CI], 1.15 to 1.43) after controlling for age, BMI, total testosterone, and the number of menses/year (Table 5).
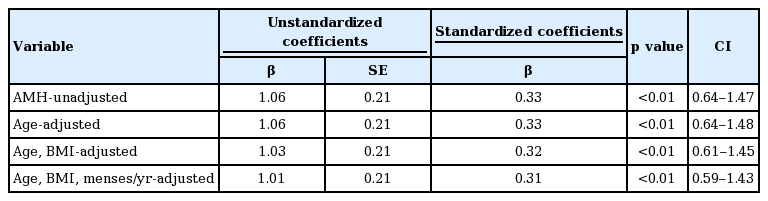
Association of AMH with total testosterone by multiple linear regression analyses in women with polycystic ovary syndrome
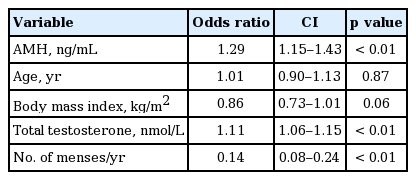
Multiple logistic regression analysis for predicting the polycystic ovary syndrome
When we divided the subjects according to age into groups with 5-year intervals, serum AMH level did not show any significant age-dependence in women with PCOS or regular cycling women (Supplementary Figs. 1 and 2). The optimal AMH cutoff value for diagnosing PCOS was 10.0 ng/mL (71% sensitivity, 93% specificity), and the area under the receiver-operating characteristic curve was 0.88 (95% CI, 0.84 to 0.91) (Fig. 1).
Receiver-operating characteristic curve for the diagnostic capability of serum anti-Müllerian hormone (AMH) levels for diagnosis of polycystic ovary syndrome. AUC, area under the curve; CI, confidence interval.
DISCUSSION
In this present study, we compared the AMH levels among four groups according to the presence of PCOS and PCOM. Serum AMH level was the highest in group 1 (HA + OM + PCOM) and the lowest in group 4 (control). Women with PCOS had higher serum AMH levels than did regular cycling women, regardless of the presence of PCOM, and women with PCOM had higher serum AMH levels than did women without PCOM, regardless of the presence of PCOS.
AMH was positively associated with HA only in women with PCOS, not in regular cycling women regardless of the presence of PCOM. We also observed that serum AMH level did not differ between the five age groups (< 20, 20 to 24, 25 to 29, 30 to 34, and ≥ 35 years). The AMH optimal cutoff value for PCOS diagnosis was 10.5 ng/mL in young Korean women.
The association of AMH level with HA observed in our study was consistent with the finding of previous studies that AMH level was positively correlated with symptom severity in PCOS [19,20]. AMH concentration was previously shown to be positively correlated with testosterone level in normogonadotropic anovulatory infertile women [21]. Additionally, one study showed that AMH level was positively related to the number of 2- to 5-mm follicles and was positively correlated with serum testosterone in women with PCOS [6,22-24]. In our study, AMH level was significantly associated with total testosterone, even after adjustment for age, BMI, and the number of menses per year. In multiple regression analysis, the number of small follicles and serum androgen levels were positively correlated with the AMH level in women with polycystic ovaries with and without HA and in normal controls during controlled ovarian hyperstimulation. HA was associated with an additional increase in AMH level in women with polycystic ovaries [25]. HA may affect AMH secretion. It has been hypothesized that intra-ovarian HA promotes early follicular growth in a mechanism involving the androgen receptor [26]. Increased serum AMH level in women with PCOS could be due to increased androgen levels in the presence of an excess of small antral follicles.
The serum AMH level was significantly positively correlated with ovarian volume and follicle number in young Korean women with PCOS. AMH is produced by the granulosa cells of follicles from the time of follicle growth initiation [27]. AMH serum level has been reported to be closely correlated with small antral follicle number in both healthy women and women with PCOS [23,28]. Disrupted folliculogenesis resulting in the arrest of follicular growth and excess accumulation of small antral follicles may increase serum AMH level in women with PCOS [29].
Serum AMH level has been reported to decline with age [27]. However, serum AMH level was not correlated with age in women with PCOS in our study, which is consistent with the finding of no significant difference in AMH level according to age in women with PCOS in a previous study in Korean PCOS patients under the age of 40 years in which the study subjects were divided into five age groups: ≤ 20, 21 to 25, 26 to 30, 31 to 35, and 36 to 40 years [30]. In a European study, serum AMH levels in women with PCOS were 2- to 3-fold higher than those in controls and remained elevated until 40 years of age [22]. The lack of AMH decline with age in women with PCOS may be due to a supraphysiologic concentration of AMH in those women compared to in regular cycling women.
The serum AMH cutoff value for PCOS diagnosis identified in our study was higher than those of previous studies. In adolescent and young adult Chinese patients (age from 17 to 25 years) with PCOS, the serum AMH cutoff value for PCOS diagnosis was 8 ng/mL, with a sensitivity of 62% and a specificity of 70% [31]. In a study performed in PCOS women from a European population (age from 22 to 36.4 years), 8.40 ng/mL was suggested as the serum AMH cutoff value for PCOS diagnosis, with a sensitivity 67% and a specificity 92% [23]. ROC analysis suggested that a serum AMH value of 5 ng/mL (sensitivity 84%, specificity 82%) was the best determinant of PCOS status in Australia [32]. The difference of ethnicity could affect the different results. An ROC curve analysis showed an AMH cutoff value of 7.8 ng/mL (sensitivity 76%, specificity 87%) for PCOS diagnosis in Korean women (21 to 39 years) [33]. The differences in the AMH cutoff values determined by different studies may be due to the different methods and assays used to measure AMH and to differences in the included subjects. Compared to the previous study in Korean PCOS women [33], BMI was slightly higher in our PCOS subjects, although age did not differ between the two studies. Recently, an increase in serum AMH levels was observed in samples that had been stored for a 30-week period [34]. Because the assays used to measure AMH did not differ between these two studies, fluctuations in serum AMH level due to storage should be considered.
A strength of our study was its relatively large sample size. Because there was no difference in age between the PCOS women and regular cycling women, we could exclude the confounding effect of age on AMH levels. However, further prospective studies are needed to evaluate AMH levels in older women with PCOS (over 40 years). In a previous prospective study of PCOS women aged 35 to 39 years, there was a significant decrease in AMH at re-evaluation after 5 years [35]. Another limitation of this study is that because universally accepted methods and assays for measuring serum AMH level are lacking, it is difficult to generalize the results of our study.
In conclusion, we observed that serum AMH level was associated with hyperandrogenemia in women with PCOS. Serum AMH level can be useful for PCOS diagnosis at any age under 40 years. The optimal serum AMH cutoff value for PCOS diagnosis identified in this study of young Korean women was 10.0 ng/mL.
KEY MESSAGE
1. The serum anti-Müllerian hormone (AMH) level can be useful for the diagnosis of polycystic ovary syndrome (PCOS) at any age less than 40 years.
2. The optimal AMH cutoff value for the diagnosis of PCOS identified in this study of young Korean women was 10.0 ng/mL.
3. Serum AMH was an independent determinant of total testosterone after adjustment for age, body mass index, and the number of menses/year.
Notes
No potential conflict of interest relevant to this article was reported.