Tracheobronchial calcification in a patient treated with warfarin
Article information
A 81-year-old woman with underlying mitral valve stenosis and atrial fibrillation visited the emergency department complaining of left hip pain after slipping. She was treated by prosthetic mitral valve replacement in 1988 and she had received warfarin therapy for 33 years. Her vital signs were stable. On hip radiograph showed left femur intertrochanteric fracture. A chest radiograph was incidentally noted for diffuse tracheobronchial tree calcification (Fig. 1). Computed tomographic scan of the chest also showed calcification of the central and peripheral airways (Fig. 2). Laboratory testing revealed normal levels of serum calcium (8.5 mg/dL), phosphorus (2.0 mg/dL), parathyroid hormone (11 pg/mL), and vitamin D (25(OH)D) (16.6 ng/mL). Bone mineral density test revealed a T-score of −4.5, indicating osteoporosis. Finally, she was diagnosed as a tracheobronchial calcification and osteoporosis associated with taking warfarin. Warfarin inhibits the formation of vitamin K-dependent proteins. Vitamin K inhibits progression of calcification and improves bone density. Long-term Warfarin therapy would induce tracheobronchial calcification and osteoporosis. In this patient, cephalomedullary nailing was performed for the left femur intertrochanteric fracture. Denosumab was administered for osteoporosis treatment. She did not complain of respiratory symptoms.
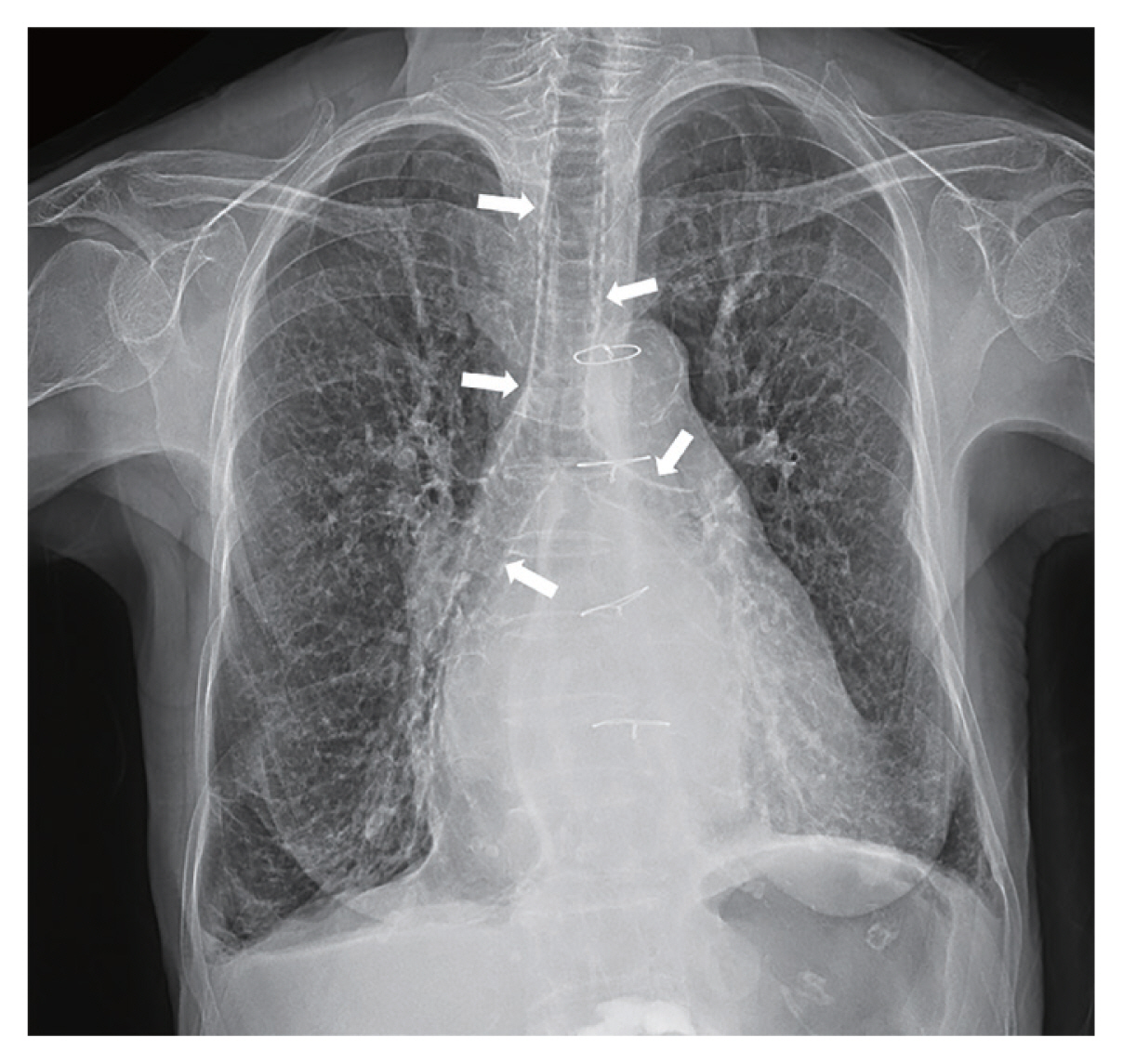
Chest radiograph showed diffuse tracheobronchial tree calcification (white arrows).
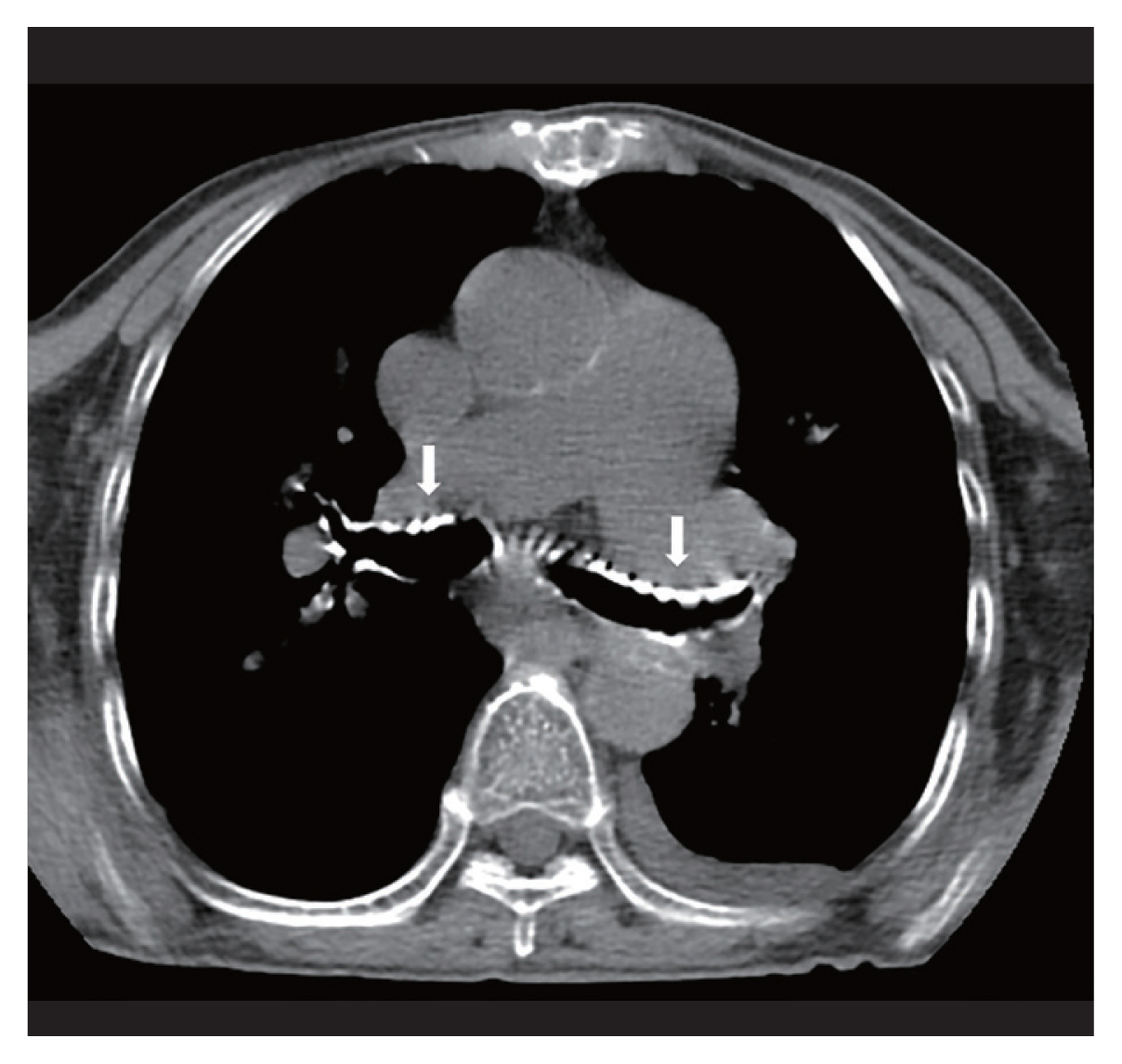
Computed tomographic scan of the chest showed calcification of the central and peripheral airways (white arrows).
Here, we describe a case of tracheobronchial calcification associated with taking warfarin. The mechanism of warfarin inducing tracheobronchial calcification is unclear, but it is thought to be due to inhibition of the activity of matrix gla protein (MGP) which prevents vascular smooth muscle proliferation and calcification. In one study, mice with mutated MGP have been shown to develop excessive calcification of the cartilage. Although warfarin-associated tracheobronchial calcification has little clinical significance, it should be distinguished from other rare pathologic conditions such as tracheobronchopathia osteochondroplastica. In addition, it is not a contraindication to continuing warfarin therapy.
Informed consent has been obtained from the patient.
Notes
No potential conflict of interest relevant to this article was reported.