Medical disputes involving lower gastrointestinal endoscopies: cases from the Korean Medical Dispute Mediation and Arbitration Agency
Article information

Abstract
Background/Aims
As the number of lower gastrointestinal endoscopies and high-risk examinees increases, the incidence of adverse events associated with these endoscopies has also increased. Medical disputes and lawsuits related to adverse events are rapidly increasing.
Methods
Medical disputes related to lower gastrointestinal endoscopy that had been filed in Korean Medical Dispute Mediation and Arbitration Agency (K-medi) from April 2012 to August 2020 were evaluated with the corresponding medical records and written appraisal. Facilities, patients, procedures, adverse events, and outcome-related variables related to medical disputes were analyzed.
Results
As the number of lower gastrointestinal endoscopies in Korea increases each year, the number of medical disputes related to lower gastrointestinal endoscopy appraised by K-medi has also increased yearly during the same period. Among the 121 cases analyzed, 86 (71.1%) were conciliated and 35 (28.9%) were cosigned by prosecution. Perforations accounted for the largest proportion of cases (93 cases, 76.9%). Most patients (n = 119, 98.3%) underwent non-emergent procedures, and only 10 (8.3%) underwent them for therapeutic purposes. Approximately one-fifth of the patients (n = 25, 20.7%) died.
Conclusions
The number of medical disputes related to lower gastrointestinal endoscopy are increasing. To prevent this, it is important to review the data on existing cases and establish specific response guidelines.

INTRODUCTION
With increasing public awareness of health checkups and increased access to medical care, the number of endoscopies performed in South Korea has steadily increased. As colonoscopies have proven to be very effective in reducing the risk of colorectal cancer, and advanced endoscopic treatment methods have also been developed and are preferred, the number of screening, diagnostic, and therapeutic lower gastrointestinal endoscopies performed in Korea has increased significantly. In addition to endoscopies being performed on young examinees, the number performed on elderly examinees with multiple comorbidities has greatly increased owing to an aging population. Cha et al. [1] reported that the annual number of colonoscopies increased from 264,345 to 2,098,850 and the number of colonoscopies with polypectomy increased from 24,179 to 624,786 between 2002 and 2013. In elderly people (75 years or older), the number of colonoscopies increased from 7,854 to 79,283, and the number of colonoscopies with polypectomy increased from 1,010 to 24,308 during the same period [1].
As the number of endoscopies performed by high-risk examinees increases, the incidence of endoscopy-related adverse events inevitably increases [2]. However, owing to the lack of a system for the systemic and reliable collection of information on the occurrence of immediate and delayed adverse events related to endoscopies, the exact incidence rate is unknown. One survey estimated that the incidence of adverse events related to lower gastrointestinal endoscopy is steadily increasing [3]. In addition, medical disputes over adverse events related to lower gastrointestinal endoscopies have recently become a major social issue for the public and the medical community [4].
Foreign countries have long made efforts to organize and prepare guidelines for the definition, terminology, severity classification, and management of adverse events [5,6] but such efforts have not been made domestically. To prevent medical disputes and accidents and to take appropriate action, it is necessary to have a good understanding of the current domestic situation. Therefore, the Korean Society of Gastrointestinal Endoscopy was requested by the Korean Medical Dispute Mediation and Arbitration Agency (K-medi) to analyze cases of medical dispute for academic purposes. Therefore, this study aimed to evaluate the characteristics of medical disputes related to lower gastrointestinal endoscopy using cases filed in K-medi.
METHODS
Data source
In South Korea, K-medi was established in April 2012 to create a fair medical environment by resolving medical disputes or claims on medical professional liability, providing a qualified and unbiased appraisal of medical accidents, and achieving equitable relief for both plaintiffs and dependents through medical mediation [7]. Medical disputes filed in K-medi for qualified and unbiased appraisal of medical accidents from April 2012 to August 2020 were retrospectively evaluated using the corresponding medical records and written appraisals. In general, the K-medi database is not available for assessment because each case contains sensitive information. However, in this study, the assessment of the database by accredited researchers was approved by a mutual agreement between K-medi and the Korean Society of Gastrointestinal Endoscopy for academic purposes.
The endoscopy quality management committee of the Korean Society of Gastrointestinal Endoscopy was provided with medical records and written appraisals with completely anonymized variables for 3 months through locked computers that could not be copied, changed, or stored in a computer or other storage devices. The Korean Society of Gastrointestinal Endoscopy participants were instructed several times to strictly prohibit the use of materials for purposes other than contracted service businesses, and each participant signed a written pledge.
Most of the cases were medical disputes in which the individuals directly involved in the affair on medical negligence, such as medical institutions/medical professionals or patients/guardians requested mediation and arbitration to K-medi. The cases were defined as “conciliation cases” in this study. Civil and criminal litigation cases in which medical evaluations were requested by the police or prosecutors for qualified and unbiased medical appraisal of medical accidents to prepare for medical litigation to K-medi were also included as “cosigned cases.”
This study is a retrospective analysis of cases proceeding with a medical dispute and requested for medical evaluation to K-medi. Therefore, it does not refer to all adverse events occurring in the entire Republic of Korea or in specific institutions or regions. Because most medical disputes are resolved through conversations and agreements between medical institutions/ medical professionals and patients/guardians and financial compensation for damages, data that represent the characteristics of all medical disputes, especially adverse events, should never be considered. Because of the nature of the data, comparisons between the groups were judged as inappropriate and were not performed. In addition, the causative factors of the adverse events were not analyzed. For indirect comparison, the number of lower gastrointestinal endoscopies performed in Korea during the same period (2012–2020) was surveyed and presented according to year, administrative district, and medical institution. Diagnostic lower gastrointestinal endoscopy was defined using the codes E7660, 7670, and 7680. Diagnostic lower gastrointestinal endoscopy was defined including the codes Q7691–7692, Q7741–7742, Q7700, Q7680, Q7730, Q7701–7703, QX706, Q7751–7752, Q7710, Q7670, and Q7720. Data were collected from the Health Insurance Review and Assessment Service (HIRA) Big Data Open Portal (https://opendata.hira.or.kr/) [8].
Definition and terminology
Medical disputes that occurred before, during, or after lower gastrointestinal endoscopy were included. Cases without written appraisals, those unrelated to lower gastrointestinal endoscopy, and duplicates were excluded. The analysis target was limited to the data provided by K-medi, and if it was not clearly presented in the provided data, it was classified as “impossible to verify.”
Cases were classified into “conciliation case” or “cosigned case” according to the route through which they were referred to K-medi for medical intervention. If the case was requested as a “conciliation case” and the appraisal was completed, but one party objected to the mediation and filed a civil or criminal lawsuit and the appraisal was requested again, the case was finally classified as a “cosigned case,” and it was deleted from “conciliation case.”
Variables were divided into patient-, facility-, procedure-, adverse event-, and outcome-related categories.
1) Patient-related variables included sex, age, comorbidities (diabetes mellitus, hypertension, cirrhosis, heart disease, cerebrovascular disease, chronic renal disease, chronic obstructive pulmonary disease, asthma, hematologic disease, and malignancy), medications (anti-platelet, anticoagulant, nonsteroidal anti-inflammatory drug, and steroid), previous abdominal surgery, and previous abdominal radiation therapy.
2) Facility-related variables: type of medical institution (tertiary or academic hospital, general hospital, hospital, clinic) and administrative district (Seoul, Gyeonggi-do, Chungcheong-do, Gyeongsang-do, Jeolla-do, Jeju-do, and Gangwon-do).
3) Procedure-related variables: emergency or not (non-emergent procedure, emergent procedure), purpose of endoscopy (screening, diagnostic, therapeutic), and sedation or not (sedative, non-sedative).
4) Adverse event-related variables: point of awareness (during endoscopy, after endoscopy), referral to a higher-level medical institution/consultation with other medical departments (yes, no), and immediate action after adverse event occurrence (conservative management, endoscopic management, radiologic intervention, surgery, and inability to take action).
5) Outcome-related variables: final patient status (treatment, treatment completion, disability, and death).
Because most cases involved perforations, a subgroup analysis was performed using additional variables.
1) Sites of perforation: terminal ileum, ascending colon (including hepatic flexure of the colon), transverse colon (including splenic flexure of the colon), descending colon, sigmoid colon, and rectum.
2) Cause of perforation: diverticulum, stricture, adhesion, biopsy, polypectomy, endoscopic submucosal dissection, underlying disease (including already perforated diverticulum and tumor), and impossible to verify (other cause was not clearly identified according to the data provided by K-medi). In cases in which overlapping causes were present, the investigation was conducted in duplicate.
Severity of adverse event (perforation): mild (procedure aborted because of an adverse event; post-procedure medical consultation; unplanned admission or prolongation for ≤ 3 nights), moderate (repeat endoscopy for an adverse event; transfusion; interventional radiology for an adverse event; unplanned admission or prolongation for 4–10 nights; intensive care unit admission for 1 night), severe (surgery for an adverse event; permanent disability; unplanned admission or prolongation for > 10 nights; intensive care unit admission for ≥ 2 nights), and fatal [6].
Ethical statement and statistical analysis
Because the analyzed data provided by K-medi did not contain any personal information, the Institutional Review Board approval was waived by the ethics committee of Hanyang University Guri Hospital (no. GURI 2023-03-025-004). The study was conducted in accordance with the principles of the Declaration of Helsinki.
Categorical variables were expressed as numbers and percentages. Continuous variables are expressed as means and standard deviations. Because of the nature of the data, comparisons between arbitrarily manipulated groups were considered inappropriate and were not performed. Therefore, no statistical program was used in this study.
RESULTS
Baseline characteristics of medical dispute cases filed in K-medi
The analysis in this study included medical disputes related to lower gastrointestinal endoscopy and those that occurred before, during, and after endoscopy. A total of 141 cases were requested for analysis by K-medi, and excluding cases unrelated to lower gastrointestinal endoscopy, cases with no written appraisal report, and duplicate cases, a total of 121 cases were included in the analysis (Fig. 1).

Flowchart of the study.
Of the 121 cases analyzed, perforation was the most common, occurring in 93 cases (76.9%), followed by 7 cases (5.8%) of other adverse events and 7 cases (5.8%) of medical disputes. Six patients (5.0%) had diagnosis-related disputes, 3 (2.5%) had bleeding, and 1 (0.8%) had cerebrovascular disease. Other adverse events included necrotizing fasciitis (one case), sepsis due to small bowel necrosis (one case), post-polypectomy coagulation syndrome (two cases), bowel preparation-related ileus (one case), and ischemic colitis (two cases) (Fig. 1).
The number of conciliation and cosigned cases by year after K-medi was established, was found to be gradually increasing every year. Considering that only the cases in which appraisals were completed in the first half of 2020 were included, an increasing trend was more evident (Fig. 2A). According to the HIRA big data, the number of diagnostic and therapeutic lower gastrointestinal endoscopies performed in Korea has also shown a gradual increase (Supplementary Fig. 1).
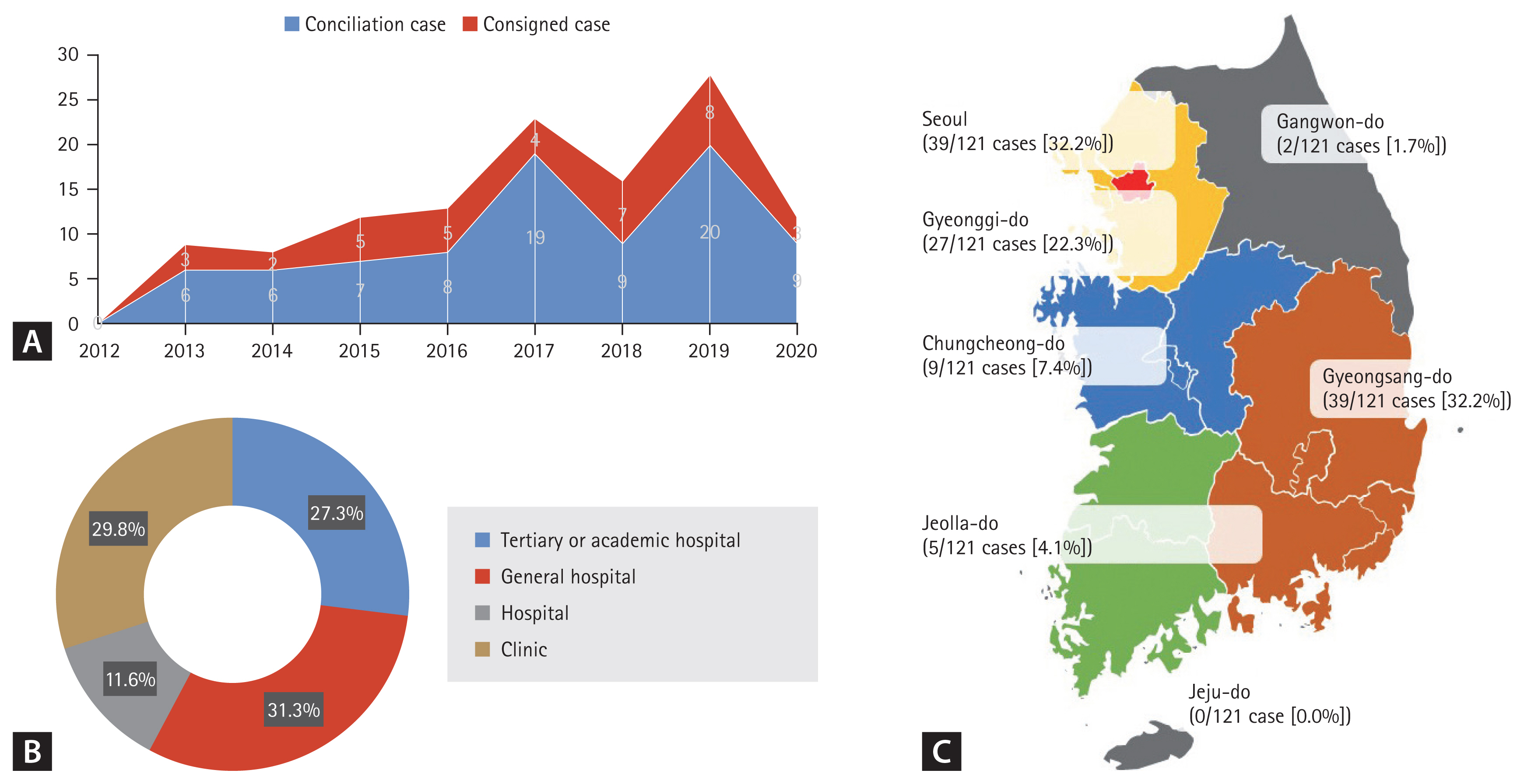
Distribution of lower gastrointestinal endoscopy cases referred to the K-medi. (A) Annual trends in the number of lower gastrointestinal endoscopy cases referred to the K-medi. (B) Number of lower gastrointestinal endoscopy cases referred to the K-medi by medical institution type. (C) Number of lower gastrointestinal endoscopy cases referred to the K-medi by administrative district. K-medi, Korean Medical Dispute Mediation and Arbitration Agency.
Patient and facility-related variables of medical dispute cases filed in K-medi
Of the 121 patients, 69 were male (57.0%) and 52 were female (43.0%). Male tended to have a higher incidence of bleeding (100.0%) and diagnostic problems (83.3%). The average age was 63.6 ± 12.4 years (range 30–87 years). Although the number of cases was limited, the mean age was lowest in patients with diagnostic problems (53.3 years) and highest in patients with cerebrovascular disease (80 years). The most common comorbidity was hypertension (n = 54, 44.6%), followed by malignancy (n = 22, 18.2%) and diabetes mellitus (n = 18, 14.9%). There was a history of abdominal surgery in 35 patients (28.9%) and radiation therapy in 2 patients (1.7%). Antiplatelets were administered to 24 patients (19.8%) and anticoagulants to 5 patients (4.1%). All patients with bleeding were on an antiplatelet or anticoagulant (Table 1).
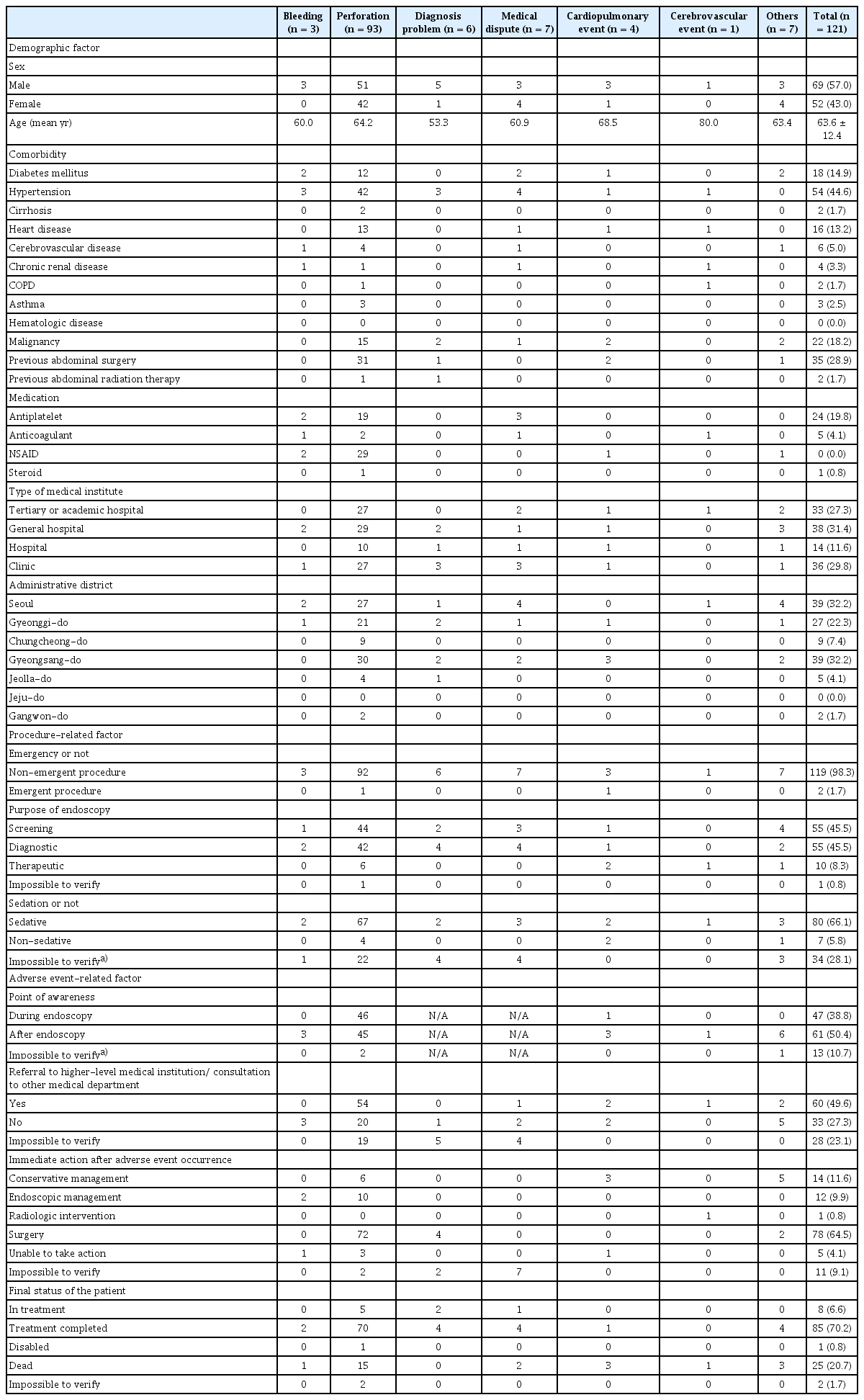
Demographic, procedure, and adverse event-related factors of cases referred to the Korean Medical Dispute Mediation and Arbitration Agency according to types of adverse events
Regarding the number of medical dispute cases by medical institute type, they most commonly occurred at the general hospital level, with 38 cases (31.3%), followed by 36 cases (29.8%) at the clinical level, 33 (27.3%) at the tertiary or academic hospital level, and 14 (11.6%) at the hospital level (Table 1, Fig. 2B). According to the HIRA big data, of all lower gastrointestinal endoscopies performed in Korea, 48% were performed at the clinical level, 19% at the hospital level, 22% at the general hospital level, and 11% at the tertiary or academic hospital level (Supplementary Fig. 2A). The distribution according to the type of medical institution was similar when divided into diagnostic and therapeutic lower gastrointestinal endoscopies (Supplementary Fig. 2B, C).
When considering the number of medical dispute cases by administrative district, most cases were observed in Seoul and Gyeonsang-do, with 39 cases (32.2%) each, followed by Gyeonggi-do with 27 cases (22.3%), and Chungcheong-do with 9 cases (7.4%) (Table 1, Fig. 2C). According to HIRA big data, of all lower gastrointestinal endoscopies performed in Korea, 23.6% were performed in Seoul, 28.3% in Gyeonsang-do, 25.2% in Gyeonggi-do, and 9.7% in Chungcheong-do (Supplementary Fig. 3A). The distribution according to administrative district was similar when divided into diagnostic and therapeutic lower gastrointestinal endoscopies (Supplementary Fig. 3B, C). In Seoul and Gyeonsang-do, the proportion of medical dispute cases referred to K-medi was slightly higher than the overall lower gastrointestinal endoscopy proportion.
Procedure and adverse event-related variables of medical dispute cases filed in K-medi
Almost all cases (n = 119, 98.3%) involved medical disputes related to non-emergency procedures. Most procedures were performed for screening (n = 55, 45.5%) or diagnostic purposes (n = 55, 45.5%), and 10 (8.3%) were related to therapeutic endoscopy. Among 87 confirmed cases (71.9%), 80 (66.1%) involved sedation (Table 1).
Of 118 of the confirmed cases (97.5%), the occurrence of adverse events was recognized during the endoscopic procedure in 47 cases (38.8%) and after the procedure was completed in 61 cases (50.4%). Of 93 confirmed patients (76.9%), 60 (49.6%) were transferred to a higher-level hospital or consulted another department after an adverse event occurred (Table 1).
Of 110 confirmed cases (90.9%), 78 (64.5%) required surgical treatment as the first action after an adverse event. There were 14 cases (11.6%) in which the first action after occurrence was conservative treatment, and 12 cases (9.9%) were treated endoscopically. No action was taken after the occurrence in five cases (4.1%) (Table 1).
Of 119 confirmed patients (98.3%), most (n = 85, 70.2%) completed the treatment. One patient (0.8%) was disabled, and 25 patients (20.7%) died (Table 1).
Type of adverse events and demographic factors of medical dispute cases according to types of arbitration
This project included 86 conciliation and 35 cosigned cases. Perforation was the most frequent adverse event in both conciliation (n = 61, 70.9%) and cosigned cases (n = 32, 91.4%), with 76.9% of all cases filed in K-medi. Among conciliation cases, the proportion of each type of adverse event showed a similar distribution to that of all cases filed in K-medi. Among the cosigned cases, most were perforation cases, including two cases (5.7%) of cardiopulmonary events and one case (2.9%) of other adverse events. The case classified as other adverse event among the cosigned cases was that of intestinal obstruction and necrosis due to a hernia that occurred through a mesenteric defect in the terminal ileum in association with bowel perforation (Fig. 3).

Types of adverse events associated with lower gastrointestinal endoscopy-related medical disputes. (A) Total. (B) Conciliation cases. (C) Cosigned cases.
According to the type of arbitration, 86 conciliation cases and 35 cosigned cases were included and analyzed. The proportion of male (conciliation cases, 59.3% vs. cosigned cases, 51.4%) and mean age (conciliation cases, 63.2 ± 12.4 years vs. cosigned cases, 64.4 ± 12.4 years) were similar (Table 2).

Demographic, procedure, and adverse event-related factors of cases referred to the Korean Medical Dispute Mediation and Arbitration Agency (K-medi) according to types of arbitration
While the most common comorbidity was hypertension (conciliation cases, 45.3% vs. cosigned cases, 42.9%), followed by malignancy (conciliation cases, 19.8% vs. cosigned cases, 14.3%), the proportions of patients with heart disease (conciliation cases, 16.3% vs. cosigned cases, 5.7%), cerebrovascular disease (conciliation cases, 5.8% vs. cosigned cases, 2.9%), and malignancy were lower in cosigned cases than in conciliation cases. The history of previous abdominal surgery (conciliation cases, 31.4% vs. cosigned cases, 22.9%) was also lower in cosigned cases than in conciliation cases (Table 2).
Considering the type of medical institution, medical dispute cases at the hospital and clinical levels accounted for 31.4% (n = 27) of conciliation cases and 65.7% (n = 23) of cosigned cases. Considering the administrative district in which the medical disputes occurred, the proportion of conciliation cases (36.0%) was higher than that of cosigned cases (22.9%) in Seoul. In Gyeongsang-do, the proportion of cosigned cases (25.6%) was higher than that of conciliated cases (48.6%) (Table 2).
Procedure and adverse event-related variables of medical dispute cases according to types of arbitration
Among the conciliation and cosigned cases, only one case each was a medical dispute related to an emergency procedure (conciliation cases, 1.2%; cosigned cases, 2.9%). Among the conciliation cases, most of the procedures were for screening (n = 34, 39.5%) or diagnostic purposes (n = 42, 48.8%), and nine cases (10.5%) were related to therapeutic endoscopy. Among the cosigned cases, there was a higher proportion of screening endoscopies (n = 21, 60.0%) and a lower proportion of therapeutic endoscopies (n = 1, 2.9%). Of the confirmed cases, most involved sedation in both conciliation (n = 53, 61.6%) and cosigned cases (n = 27, 77.1%) (Table 2).
When considering only classifiable cases, the proportion of conciliation cases with the timing of recognition of the occurrence of adverse events was similar during (n = 35, 40.7%) and after completion of endoscopy (n = 37, 43.0%). However, in the cosigned cases, the proportion of cases in which adverse events were recognized was higher in cases after the completion of endoscopy (n = 21, 60.0%) than in cases during endoscopy (n = 12, 34.3%). Among the confirmed cases, the proportion of patients transferred to a higher-level hospital for consultation with another department after the occurrence of adverse events was higher in cosigned cases (n = 26, 74.3%) than in conciliation cases (n = 34, 40.7%) (Table 2).
Of the confirmed cases, the proportion of patients in whom the immediate action after an adverse event was surgery was higher for the cosigned cases (n = 26, 74.3%) than for the conciliation cases (n = 52, 60.5%). Of the confirmed patients, most were in treatment (n = 6, 7.0%) or had completed treatment (n = 67, 77.9%) in conciliation cases, whereas the proportions were lower in cosigned cases (in treatment: n = 2, 5.7%; treatment completed: n = 18, 51.4%). The proportion of patients in whom the final outcome was death was higher in the consignment (n = 12, 34.3%) than in the conciliation group (n = 13, 15.1%) (Table 2).
Medical appraisal results by K-medi
Based on the appraisal report, a causal relationship was revealed between the overall process of endoscopic procedures and medical disputes in most cases (n = 99, 81.8%), except for four cases (3.3%) that were difficult to clearly classify (Table 3). In addition, after excluding 17 cases (14.0%) that were difficult to classify clearly, inadequacies in the overall endoscopic procedure were recognized in more than half of the cases (n = 65, 53.8%) (Table 3).
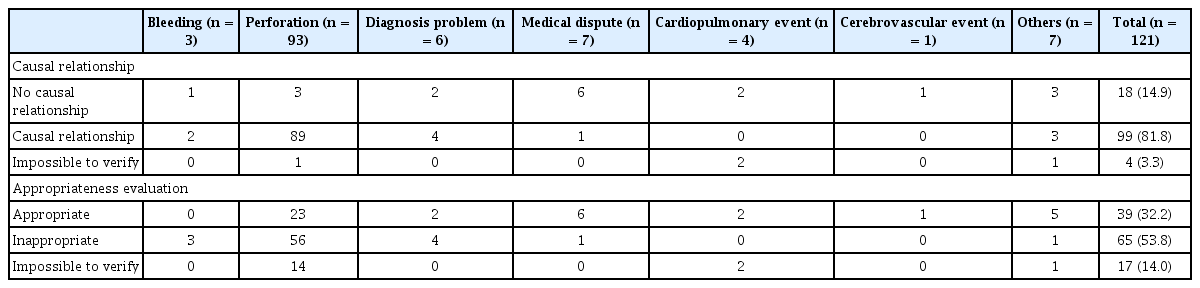
Causal relationship and appropriateness evaluation results of arbitration by the Korean Medical Dispute Mediation and Arbitration Agency (K-medi) according to types of adverse events
Subgroup analysis of perforation cases
Among all perforation cases, which account for the majority of all lower gastrointestinal endoscopy-related medical dispute cases requested for medical appraisal by K-medi (n = 93/121, 76.9%), four cases of perforation related to bowel preparation and one case of intra-abdominal bleeding due to intra-abdominal damage caused by the endoscope were excluded. Therefore, a subgroup analysis was performed on narrowly defined perforation cases, which indicated that bowel wall defects occurred because of the scope or accessory device used (n = 88, 72.7%). There were 58 conciliation cases (n = 58/88, 65.9%) and 30 cosigned cases (n = 30/88, 34.1%).
Female comprised a higher proportion of fatal cases (n = 9/39, 23.1%) and a lower proportion of moderately severe cases (n = 4/39, 10.3%) than male (fatal cases: n = 2/49, 4.1%; moderately severe cases: n = 8/49, 16.3%) (Fig. 4A). By age group, all perforation cases in patients < 50 years were moderate or severe (n = 30/30, 100.0%). However, fatal cases included those aged ≥ 60 years (n = 2/24, 8.3%) and reached a quarter of those aged ≥ 70 years (n = 9/34, 26.5%) (Fig. 4B). Compared with patients without a history of abdominal surgery or radiation therapy, those with a history had a lower rate of moderate severity (n = 1/32, 3.1%; without history, n = 11/56, 19.6%) and a higher rate of fatalities (n = 5/32, 15.6%; without history, n = 6/56, 10.7%) (Fig. 4C).

Severity of perforation in lower gastrointestinal endoscopy-related medical disputes according to patient demographics and procedural factors. (A) By sex. (B) By age group. (C) History of abdominal surgery or radiation therapy. (D) By purpose of procedure. (E) By point of awareness. (F) By perforation site. (G) By cause of perforation.
According to the purpose of the procedure, there were no fatalities among therapeutic endoscopy cases (n = 0/29, 0.0%), and the proportion of moderate severity (n = 9/29, 31.0%) was higher than that of diagnostic endoscopy (n = 3/59, 5.1%) (Fig. 4D). When divided according to the time of recognition of perforation occurrence, the severity of perforation was similar between groups (Fig. 4E). The most common site of perforation was the sigmoid colon (n = 61/88, 69.3%). Nine patients died (n = 9/61, 14.8%) from sigmoid colon perforation, and two (n = 2/7, 28.6%) died from rectal perforation (Fig. 4F). When analyzing perforation cases according to the cause of perforation, the proportion of severe or fatal cases was higher in the groups with diverticulum/adhesion/stricture (n = 28/29, 96.6%) and underlying diseases vulnerable to bowel perforation (n = 6/6, 100.0%). Underlying diseases included rectal cancer that had already been perforated before endoscopy, surveillance after low anterior resection surgery for rectal cancer, Crohn’s disease with a history of surgery (small bowel resection and anastomosis), cecal diverticulitis, sigmoid colon diverticulitis, and multiple connective tissue disorders with vasculitis and serositis (pericarditis and pleuritis). In cases of perforation presumed to have been caused by biopsy/ polypectomy, the proportion of cases with moderate severity was high (n = 7/25, 28.0%), and there were no fatal cases (n = 0/25, 0.0%) (Fig. 4G).
When analyzed according to the purpose of the procedure, the proportion of cases in which perforation was recognized during the procedure was higher in diagnostic endoscopy than in therapeutic endoscopy (diagnostic endoscopy, n = 38/59, 64.4%; therapeutic endoscopy, n=6/29, 20.7%) (Fig. 5A). Among the patients with perforations that occurred during diagnostic endoscopy, endoscopic management was performed in 18 out of 59 patients (30.5%) and surgery in 35 out of 59 patients (59.3%) as an immediate action (Fig. 5B). As a final management, endoscopic management was performed in 4 out of 59 patients (6.8%) and surgery in 50 out of 59 patients (84.7%). In one case (n = 1/59, 1.7%), conservative management was the final management. In four cases (n = 4/59, 6.8%), no immediate or final action was taken (Fig. 5C). Among the patients with perforations that occurred during therapeutic endoscopy, as an immediate action, endoscopic management was performed in 7 out of 29 patients (24.1%), and surgery was performed in 17 out of 29 patients (58.6%) (Fig. 5B). As a final management, endoscopic management was performed in 5 out of 29 patients (17.2%), and surgery was performed in 19 out of 29 patients (65.5%). In five cases (5/29, 17.2%), conservative management was the final management. There were no cases in which action was not taken immediately or at the end (Fig. 5C). The proportion of severe or fatal adverse events was higher with diagnostic endoscopy (n = 56/59, 94.9%; therapeutic, n = 20/29, 69.0%), and there were no fatal cases with therapeutic endoscopy (Fig. 5D).

Differences in perforation characteristics in medical disputes related to lower gastrointestinal endoscopy according to procedural purpose. (A) Point of awareness. (B) Immediate action after perforation. (C) Final management after perforation. (D) Classification of perforation severity.
Among the 25 cases in which bowel perforation occurred after biopsy/polypectomy, the severity of perforation was compared between 5 cases in which prophylactic clipping was performed, even though perforation was not grossly apparent, and 20 cases in which prophylactic clipping was not performed. The proportion of severe cases was higher in the group that did not undergo prophylactic clipping (n = 17/20, 85.0%; clipping, n = 1/4, 20.0%) (Fig. 6).

Classification of perforation severity based on medical disputes related to lower gastrointestinal endoscopy with clipping after biopsy or polypectomy.
There were four cases in which perforation occurred during diagnostic endoscopy, but the patients died without immediate or final action. These cases are summarized by case and presented in Table 4. Among the 93 cases classified as perforation, the remaining 5 cases, excluding the 88 cases in which the above subgroup analysis was performed, are summarized by case and presented in Table 4. Three cases of bleeding occurred in patients taking antiplatelet or anticoagulant agents, all of whom underwent polypectomy. A cerebrovascular event and four cardiopulmonary cases are also summarized by case and presented in Table 4.
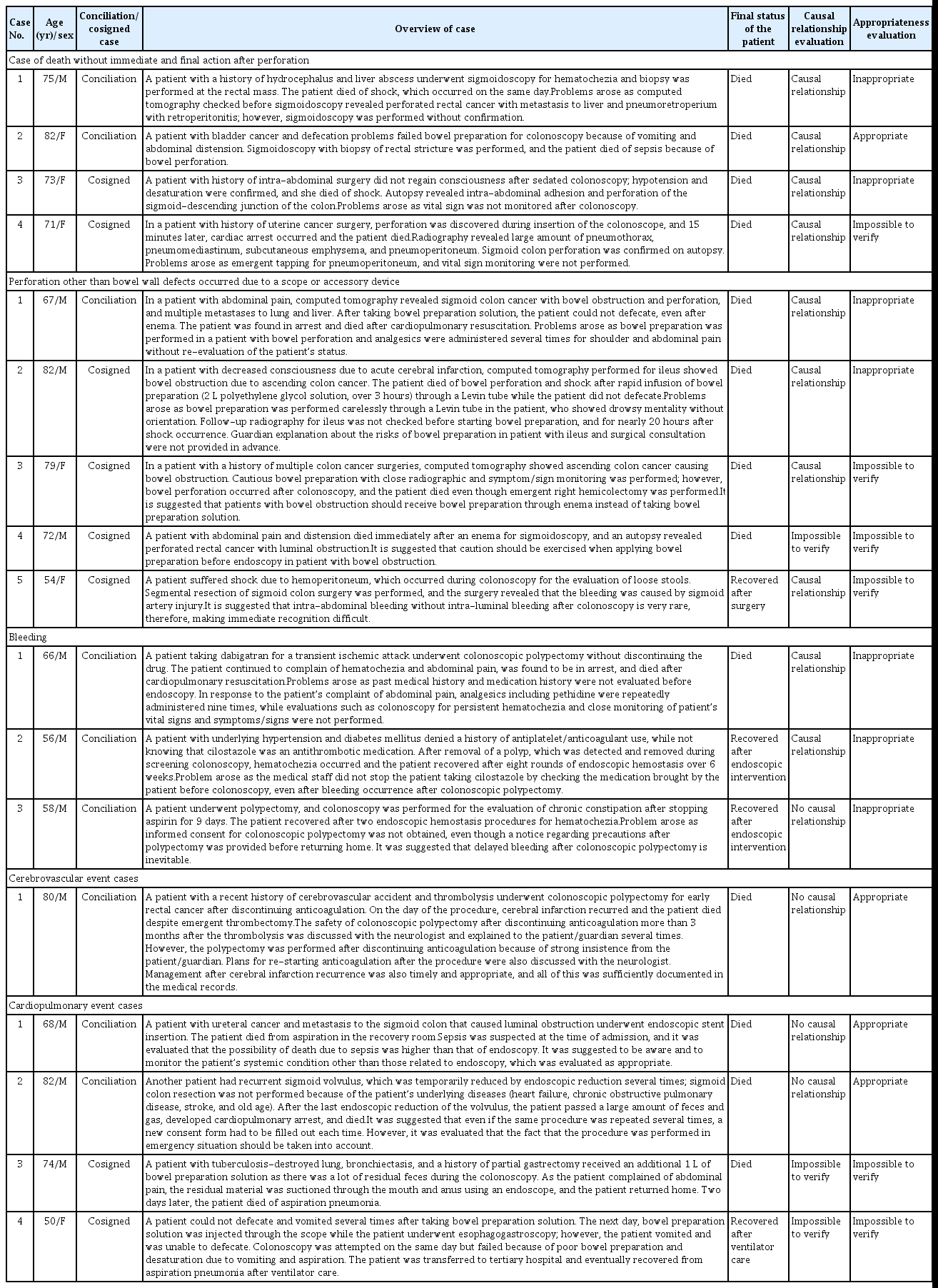
Summary of individual cases
DISCUSSION
This study evaluated medical disputes related to lower gastrointestinal endoscopy that had been filed in K-medi with the corresponding medical records and written appraisal. As the number of cases of lower gastrointestinal endoscopy in Korea increases each year, the number of medical disputes related to lower gastrointestinal endoscopy appraised by K-medi has also increased every year during the same period. Among the 121 cases analyzed, 71.1% were for conciliation and 28.9% were consigned by prosecution. Perforation accounted for more than three-quarters of all cases. Most patients underwent non-emergent procedures and only 8.3% were treated for therapeutic purposes. Approximately a fifth were cases of patients who died.
While approximately 52% of all lower gastrointestinal endoscopies in Korea were performed in Seoul and Gyeonsang-do, about 65% of all medical disputes filed in K-medi occurred in Seoul and Gyeonsang-do. In these areas, the proportion of medical dispute cases referred to K-medi was slightly higher than that of the other area. Although approximately 30% of all medical disputes occur at the clinical level, approximately 48% of all lower gastrointestinal endoscopies in Korea were performed at the clinical level. In addition, while approximately 27% of all medical disputes occurred at tertiary or academic hospital-level medical institutions, approximately 11% of all lower gastrointestinal endoscopies in Korea were performed at tertiary or academic hospital-level medical institutions. This means that the proportion of medical disputes occurring in these areas and in tertiary or academic hospital-level medical institutions is higher than in other areas or types of medical institutions. However, caution must be taken when interpreting, as this does not refer to a total investigation of the “rate of medical accidents,” but rather the “rate of medical disputes appraised by K-medi.” Another important factor to consider is that various patient and procedural factors significantly influence the occurrence of medical accidents. South Koreans has very high access to medical care. However, considering that endoscopies in patients with major diseases, such as cancer or multiple comorbidities, and high-risk procedures are mainly performed at tertiary medical institutions in Seoul and large cities, these regions and tertiary or academic hospital-level medical institutions have a higher risk of medical accidents and disputes. In addition, approximately 18% of all lower gastrointestinal cases include malignancy, and it can be assumed that these patients are at high risk of medical accidents and disputes [9]. Clinic-level medical institutions are expected to mainly perform endoscopy screenings and low-risk endoscopic procedures in relatively low-risk patients. However, approximately 30% of all medical disputes occurring at the clinical level cannot be considered a low percentage. Additionally, it can impose a significant burden on the treatment environments of primary medical institutions [10,11].
In this study, most cases were medical disputes related to non-emergency and screening/diagnostic endoscopy, although the risk of adverse events occurring during therapeutic and emergent endoscopies is generally much higher [12,13]. This suggests that when adverse results occur compared to expected results, there is a high risk of progression to disputes owing to the lack of acceptance and negotiation of the adverse results compared with those of emergency/ therapeutic endoscopy. Based on the results of this study, diagnostic errors can lead to disputes even if they occur at a young age. Similarly, in the cosigned cases, the proportions of comorbid heart disease, cerebrovascular disease, malignancy, and history of abdominal surgery were lower than those in the conciliation cases. In addition, in consigned cases, the proportion of disputes occurring after screening/ diagnostic endoscopy was higher, and the proportion of disputes occurring after therapeutic endoscopy was lower than that in conciliation cases. In cosigned cases, the proportion of cases that occurred at clinic/hospital-level institutions was higher, whereas in conciliation cases, the proportion of general hospital/tertiary or academic hospital-level medical institutions was higher. Among the conciliation cases, most were in or had completed treatment; however, the proportion of deaths was high in the cosigned cases. Among the cosigned cases, a high proportion of adverse events were observed after the endoscopic procedure was completed. These results have important implications for future studies. However, since this is an analysis of cases where medical appraisal were conducted at K-medi as medical disputes, rather than a full investigation of the occurrence of total adverse events, various social, economic, and cultural factors in addition to medical factors come into play, and interpretation may be difficult [14]. Even if a medical accident occurs, it does not always proceed as a medical dispute and is referred to an arbitration agency or judicial agency; in most cases, the dispute is concluded by an agreement between the patient/guardian and the hospital/doctor. Therefore, the proportion of patients who died in this study was found to be very high, approximately 20.7%.
Most perforations were for screening/diagnostic purposes and most were delayed perforations. Although there were five cases (4.1%) in which action could not be taken, the rate of immediate surgery was high. There were cases in which disputes arose even though the treatment was completed endoscopically or surgically, especially with conservative treatment. In Korea, there is a misconception that perforations occurring during endoscopy are due to intentional negligence by doctors, which tends to easily lead to disputes. However, despite an increasing number of studies on the technical difficulties, there has been no significant change in the incidence of adverse events, especially perforation and bleeding, after lower gastrointestinal endoscopy. There is an inevitable portion of adverse events such as perforation that can occur stochastically, regardless of the experience of the procedure [15]. Therefore, it is important to improve public awareness and provide information on the precautions regarding the possibility of delayed adverse events following lower gastrointestinal endoscopy.
Among perforation cases, the fatality rate was higher in female, older patients, and those with a history of abdominal surgery or radiation therapy. Fatal cases included only those with sigmoid and rectal perforations. The severity was higher in perforations that occurred after diagnostic endoscopy than in those that occurred after therapeutic endoscopy. There were no fatal cases, and many had moderate severity. There was no difference in severity depending on the time of recognition of the occurrence of perforation; however, it should not be interpreted that the results were not different, even if the perforation was recognized after the procedure. When a perforation is recognized during therapeutic endoscopy, immediate action is taken endoscopically or surgically; therefore, it is highly likely that an agreement will be reached between the patient/guardian and the doctor/hospital, and that it will not proceed into dispute. In cases of perforation during therapeutic endoscopy, perforations recognized after the procedure are often difficult to manage endoscopically, and the number of cases considered for surgical treatment from the beginning is higher. However, in cases of perforation that occurs during diagnostic endoscopy, taking action may not be possible, as the patient’s condition rapidly deteriorates. Therefore, there were four cases (6.8%) of perforation in which action was not taken, despite the absence of such cases on therapeutic endoscopy. This suggests that it is important to be aware of the steps to be taken in emergency situations, such as resuscitation and tapping for tension pneumoperitoneum [16].
This study had some limitations owing to the characteristics of the data used. The analysis was performed retrospectively using written appraisal and only a part of medical records which were collected, stored, and provided by K-medi, and requests for additional necessary data were not possible. Therefore, information on important variables, such as body mass index, laboratory findings, and vital signs, could not be included as analysis variables because there were too many missing data points. Moreover, it was impossible to analyze adverse events other than perforations because of the small sample size. Furthermore, this study includes a retrospective analysis of cases proceeding with a medical dispute and requested for medical evaluation to K-medi. Therefore, it does not refer to all adverse events occurring in the entire Republic of Korea or in specific institutions or regions. Because most medical disputes are resolved through conversations and agreements between medical institutions/medical professionals and patients/ guardians, and financial compensation for damages, data that represent the characteristics of all medical disputes, especially adverse events, should never be considered. Due to the nature of the data, comparisons between the groups were judged as inappropriate and were not performed. In addition, the causative factors of the adverse events were not analyzed. To partially overcome this limitation, the number of lower gastrointestinal endoscopies performed in Korea during the same period (2012–2020) was surveyed and presented by year, administrative district, and type of medical institution for indirect comparison, using data collected from the HIRA Big Data Open Portal. The K-medi database is not publicly available for assessment because each case contains sensitive information. However, in this study, the assessment of the database by accredited researchers was approved for academic purposes through a mutual agreement between K-medi and the Korean Society of Gastrointestinal Endoscopy. Therefore, although the data do not represent all adverse events occurring throughout the Republic of Korea, the characteristics of medical disputes related to lower gastrointestinal endoscopy can be better understood from these highly selected cases.
With the increasing public awareness of health checkups and increased access to medical care, the number of screening, diagnostic, and therapeutic lower gastrointestinal endoscopies performed in South Korea has steadily increased. Moreover, owing to the aging population, the number of endoscopies performed in elderly patients with multiple comorbidities has greatly increased [1]. An increase in the number of high-risk endoscopic procedures performed on high-risk patients will inevitably lead to more medical accidents [17,18]. Relatively common adverse events such as perforation and bleeding, and rare adverse events such as air embolism and splenic injury are often difficult to predict or prevent in advance [12]. Although various studies have been conducted over a long period, lower gastrointestinal endoscopy-related adverse events occur at a certain rate, which means that adverse events can inevitably occur stochastically regardless of the experience of the procedure [15]. However, owing to differences in perspectives on medical accidents and expectations of medical outcomes, medical accidents have recently been disputed in Korea. Oh et al. [19] analyzed 22 lawsuits involving colon perforation that occurred after lower gastrointestinal endoscopy and excluded those from 2005 to 2015. In this study, most cases were ruled in favor of the plaintiff (n = 20/22), and the allegations against the defendants were performance errors, improper monitoring after the procedure, and a lack of informed consent. To prevent this trend from worsening, it is necessary to review, consider, and objectively evaluate existing medical accidents and dispute cases. Endoscopy-related academic societies should provide legal advice on appropriate responses to medical disputes and improve awareness of the legal community through constant communication. Moreover, public campaigns should be conducted to inform patients that endoscopy-related adverse events inevitably occur at a certain rate, and that it may not be appropriate to undergo screening endoscopy with old age or major comorbidities. Endoscopy-related medical accidents that inevitably occur must be covered by “compensation for unavoidable medical accidents” operated by the government. Finally, stomach and colorectal cancer screening should not be performed in a nonselective manner, regardless of the upper age limit or comorbidities, through the national cancer screening program in Korea.
This study is the first to analyze medical dispute cases related to lower gastrointestinal endoscopy, which underwent medical appraisal by K-medi. In the future, follow-up research should be conducted to analyze the causative factors and suggest specific measures based on existing medical disputes to prevent similar cases. To do so, a uniform definition of lower gastrointestinal endoscopy-related adverse events should be used as well as a standardized system and recording methods when medical accidents and disputes occur [15]. These efforts will be essential not only for patient safety but also for the safety of medical professionals.
KEY MESSAGE
1. As the number of lower gastrointestinal endoscopies in Korea increases each year, the number of medical disputes related to lower gastrointestinal endoscopy appraised by K-medi has also increased yearly during the same period.
2. Perforation accounted for the largest proportion of the cases.
3. Most patients underwent nonemergent procedures for screening or diagnostic purposes.
Notes
Acknowledgments
We thank the Korean Medical Dispute Mediation and Arbitration Agency for allowing us to review the database related to medical disputes of lower gastrointestinal endoscopies. This study was conducted as part of a project commissioned by the Medical Dispute Mediation and Arbitration Agency in Korea from October 2020 to June 2021, titled “Analysis of the types and causes of gastrointestinal endoscopy-related medical accidents to make effective preventive measures.”
CRedit authorship contributions
Eun Hye Oh: conceptualization, data curation, formal analysis, writing - original draft, funding acquisition; Jeong Eun Shin: conceptualization, formal analysis, writing - review & editing; Jun Yong Bae: data curation; Yoon Suk Lee: data curation; Yehyun Park: data curation; Yong Hwan Kwon: data curation; Chang Nyol Paik: data curation; Jun Kyu Lee: data curation; Tae Hee Lee: conceptualization, writing - review & editing, supervision, funding acquisition
Conflict of Interest
The authors declare no conflicts.
Funding
This work was supported by research funds from Soonchunhyang University and Hanyang University (HY-202300000001157).