Comparison between ligation-assisted and precutting endoscopic mucosal resection for small rectal neuroendocrine tumors: a CHASID study
Article information
 , Dae Sung Kim3, Hee Seok Moon4, Hoon Sup Koo3, Hyun Deok Shin1, Ki Bae Bang1, Kyu Chan Huh3, Chungcheong-Daejeon Association for the Study of Intestinal Diseases (CHASID)
, Dae Sung Kim3, Hee Seok Moon4, Hoon Sup Koo3, Hyun Deok Shin1, Ki Bae Bang1, Kyu Chan Huh3, Chungcheong-Daejeon Association for the Study of Intestinal Diseases (CHASID)Abstract
Background/Aims
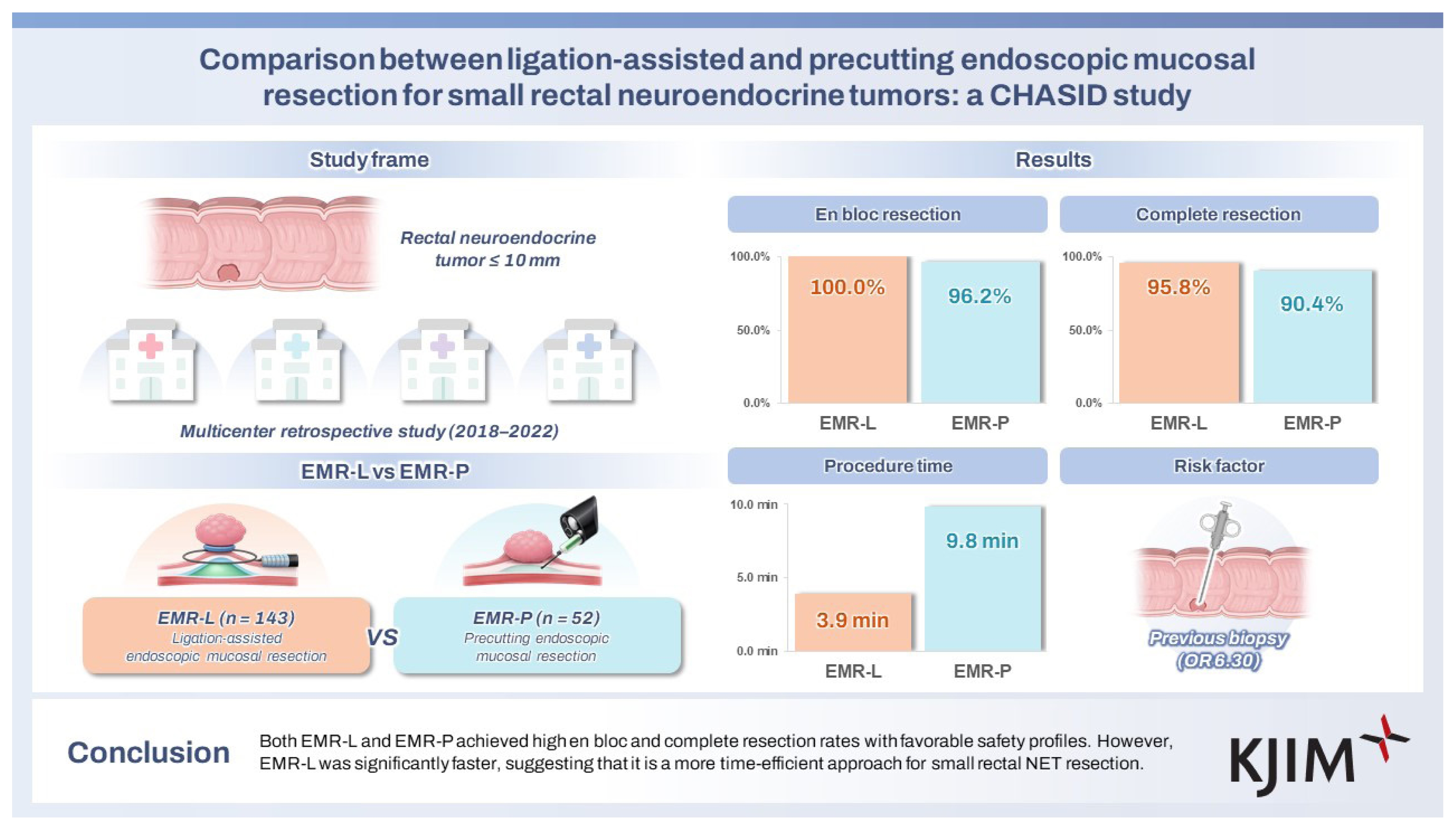
Few studies have compared modified endoscopic mucosal resection (EMR) techniques for small rectal neuroendocrine tumors (NETs). This study evaluated the clinical outcomes of ligation-assisted EMR (EMR-L) and precutting EMR (EMR-P) for the treatment of small rectal NETs.
Methods
We retrospectively reviewed patients who underwent EMR-L or EMR-P for rectal NETs ≤ 10 mm at four university hospitals between January 2018 and December 2022. Primary outcomes were en bloc resection and complete resection rates; secondary outcomes included procedural time and complications.
Results
Among a total of 195 rectal NETs, 143 were resected using EMR-L and 52 using EMR-P. Although the histopathologically measured lesion size (4.0 ± 1.7 mm vs. 5.2 ± 2.4 mm, p = 0.002) was larger in the EMR-P group, the presence of ulcer or depression and lesion location did not significantly differ between the two groups. The en bloc resection rate (100.0% vs. 96.2%, p = 0.070) and complete resection rate (95.8% vs. 90.4%, p = 0.140) also were not significantly different. However, EMR-L had a significantly shorter procedure time (3.9 ± 2.3 min vs. 9.8 ± 5.6 min, p < 0.001). No significant differences were observed in procedure-related bleeding, perforation, recurrence, or hospital stay between the groups.
Conclusions
Both EMR-L and EMR-P achieved high en bloc and complete resection rates with favorable safety profiles. However, EMR-L was significantly faster, suggesting that it is a more time-efficient approach for small rectal NET resection.
INTRODUCTION
The increased prevalence of colon cancer screening procedures, such as colonoscopy, has led to a rise in the incidental detection of rectal neuroendocrine tumors (NETs). A rectal NET, also known as a rectal carcinoid tumor, is a relatively rare type of tumor that originates in the neuroendocrine cells of the rectum [1]. Most rectal NETs are less than 10 mm in size and grow slowly, exhibiting a more favorable prognosis compared with adenocarcinomas. However, some may progress invasively and metastasize to other organs [2].
Approximately 50% of rectal NETs are incidentally detected during colonoscopy in asymptomatic individuals at an early stage. In cases of disease progression, symptoms such as lower abdominal discomfort, constipation, rectal bleeding, and diarrhea may manifest [3]. The most critical prognostic factor is tumor size. The risk of metastasis increases with lesion size, ranging from 0–10% for tumors < 10 mm, 4–30% for those 10–19 mm, and 57–80% for those ≥ 20 mm [3–5]. Additionally, metastatic risk is heightened in lesions with morphological ulceration, erythema, depression, deep muscular invasion, lymphatic or perineural invasion, a high mitotic rate, an elevated Ki-67 index, or age ≥ 60 years [6–8].
The treatment approach for rectal NETs is determined by several factors, including lesion size, morphological features, grade of differentiation, depth of vertical invasion, presence of lymphatic vessel invasion, and risk of metastasis [9]. Although the prognosis is generally favorable, locoregional or distant metastasis can occur. Therefore, complete resection is necessary for rectal NETs [10]. Several endoscopic treatment modalities are available, including conventional polypectomy, endoscopic mucosal resection (EMR), cap-assisted EMR (EMR-C), band ligation-assisted EMR (EMR-L), precutting EMR (EMR-P), and endoscopic submucosal dissection (ESD). EMR-C, EMR-L, and EMR-P are collectively classified as modified EMR techniques [1, 11]. However, because most rectal NETs originate in the submucosal layer, the rate of complete resection by conventional polypectomy or EMR is relatively low, at less than 60% [12–14].
Modified EMR techniques are more effective than conventional EMR for treating small rectal NETs [15,16]. However, few studies have specifically compared the effectiveness of modified EMR techniques, particularly between EMR-P and EMR-L. Therefore, we evaluated the clinical outcomes of EMR-L and EMR-P for the treatment of small rectal NETs.
METHODS
Study population and design
This study retrospectively reviewed patients who underwent EMR-L or EMR-P for rectal NETs smaller than 10 mm at four university hospitals in the Daejeon-Chungcheong region of Korea from January 2018 to December 2022. Cases were excluded if there were suspicions of metastasis based on abdominopelvic computed tomography or deep invasion into the proper muscle layer as indicated by endoscopic ultrasonography prior to endoscopic resection of rectal NETs. Additionally, cases were excluded if rectal NETs were removed using methods other than EMR-L or EMR-P, such as ESD, conventional EMR, or EMR-C.
Data collection and outcome measurements
All patients underwent abdominopelvic computed tomography to detect lymph node metastasis (LNM) and distant metastasis. Additionally, based on the clinical judgment of individual endoscopists, some patients underwent endoscopic ultrasonography to evaluate possible proper muscle layer invasion or LNM. The size, color, and shape characteristics of the tumors were determined by experienced endoscopists who reviewed endoscopic findings and images documented in the medical records at each participating hospital. Histopathological analyses of tumor size, en bloc resection, and complete resection were conducted by board-certified gastrointestinal pathologists at each hospital. The histological grade of each rectal NET was determined based on the Ki-67 index and mitotic activity, following the World Health Organization classification [17].
Endoscopic procedure
All procedures were performed using single-channel colonoscopes (Series 260 and 290; Olympus America, Center Valley, PA, USA). The selection of transparent caps and oval snares, ranging in diameter from 10 to 15 mm, was based on the individual preferences of the endoscopists, as was the decision to use either EMR-L or EMR-P as the resection method.
EMR-L utilizes band ligation, and the procedure was performed as follows. After a mixed solution of 0.9% saline, a small amount of indigo carmine, and epinephrine had been injected into the submucosa, EMR-L was performed by aspirating the lesion into the ligation device (a pneumatic esophageal varix ligation device from Sumitomo Bakelite, Tokyo, Japan; Shooter Saeed Multi-Band Ligator from Cook Medical, Bloomington, IN, USA), deploying the elastic band, and resecting the snare below the elastic band using an electrosurgical current (Endo Cut Q, effect 3, cut duration 1, cut interval 3, VIO 300D; ERBE Elektromedizin, Tübingen, Germany) (Fig. 1).
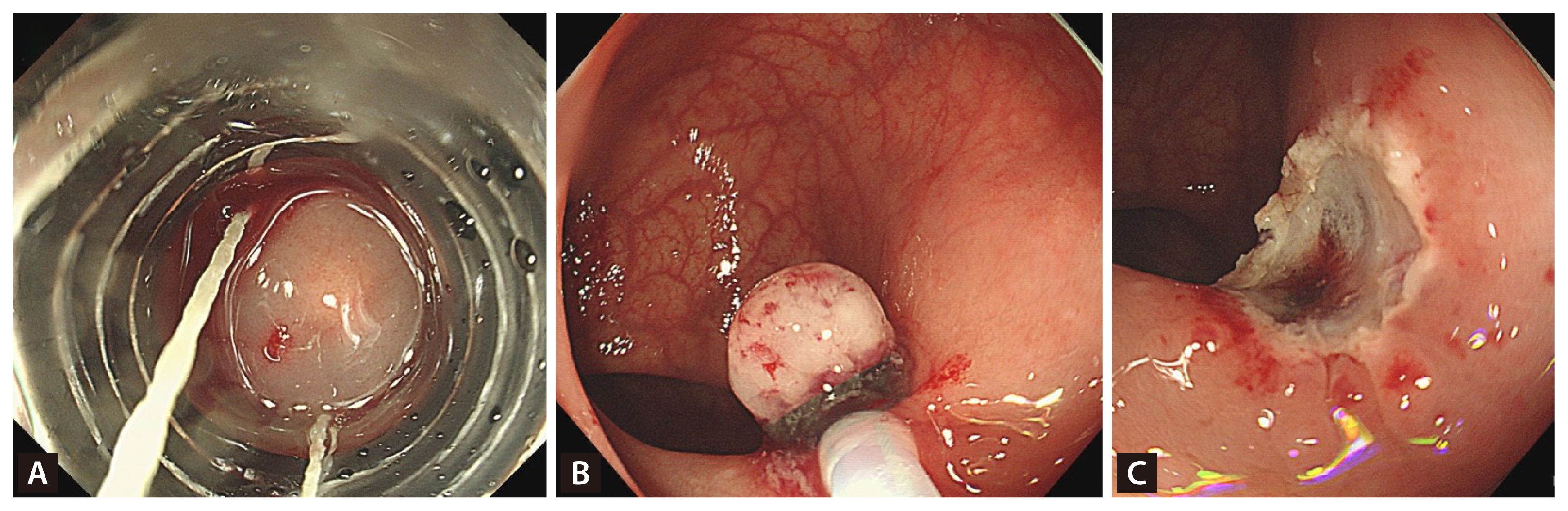
EMR-L procedure. (A) Inject a mixed solution and aspirate the lesion into the ligation device. (B) Deploy the elastic band and resect the snare below the elastic band using electrosurgical current. (C) Resect the rectal neuroendocrine tumor. EMR-L, ligation-assisted endoscopic mucosal resection.
EMR-P was performed as follows. A mixed solution of 0.9% saline was injected into the submucosa to elevate the lesion. A circumferential incision, approximately 1–2 mm from the lesion’s edge, was then made using an endoscopic knife (DualKnife; Olympus Co., Tokyo, Japan) or the tip of a snare. Following the incision, a snare was placed within the groove, tightened, and used to resect the lesion with electrosurgical current (Endo Cut Q, effect 3, cut duration 1, cut interval 3; VIO 300D) (Fig. 2). After completion of both procedures, endoscopists carefully inspected the resection site for any residual lesion and potential complications, such as perforation.
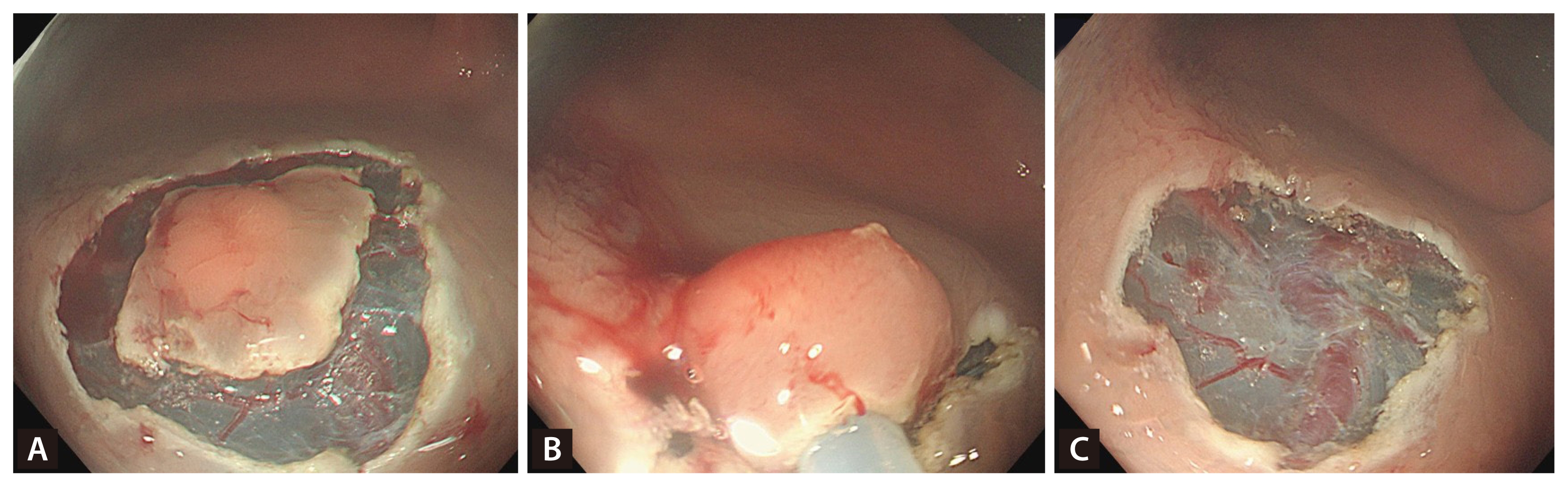
EMR-P procedure. (A) Make a circumferential incision around the lesion’s edge using an endoscopic knife or the tip of a snare. (B) Following the incision, place a snare within the groove, tighten it, and use it to resect the lesion with electrosurgical current. (C) Resect the rectal neuroendocrine tumor. EMR-P, precutting endoscopic mucosal resection.
All patients underwent abdominal computed tomography (CT) at the time of initial diagnosis to rule out metastasis. After the index endoscopic resection, most patients underwent follow-up colonoscopy within 6–12 months. Subsequent surveillance was performed at intervals of 1–2 years, according to the discretion of the treating physician. Additional abdominal CT scans were also performed selectively, depending on each physician’s clinical judgment.
Definitions of factors
The location of rectal NETs was categorized as lower (0–6 cm from the anal verge), middle (7–11 cm), and upper (12–15 cm). En bloc resection was defined as the removal of the entire tumor as a single piece, whereas complete resection entailed en bloc removal with negative margins histologically (tumor-free laterally and vertically). Total procedure time was measured from the initiation of submucosal injection to the completion of tumor resection, including any required hemostatic interventions. Perforation was defined as either direct penetration of the intestinal wall during the procedure or the presence of extraluminal air detected on a postoperative X-ray or computed tomography scan. Recurrence was defined as the reappearance of a rectal NET at the original resection site during the follow-up period.
Ethics approval and statistical analyses
This study was conducted in accordance with the Declaration of Helsinki, and was approved by the Institutional Review Boards (IRBs) of all participating institutions (Soonchunhyang University IRB No. SCHCA 2022–11–025; Dankook University IRB No. DKUH 2022-10-028-001). Due to the retrospective study, the need for informed consent was waived.
Statistical analyses were performed using SPSS software (version 21.0; IBM Corp., Armonk, NY, USA). For continuous variables, we used an independent samples t-test; the Mann–Whitney U test was used if the data did not follow a normal distribution. For categorical variables, we used either the chi-square test or Fisher’s exact test. Values of p < 0.05 were considered statistically significant.
RESULTS
In total, 195 rectal NETs were successfully removed by either EMR-L (n = 143) or EMR-P (n = 52). Mean ages were 48.7 ± 12.3 years in the EMR-L group and 50.2 ± 11.5 years in the EMR-P group, with no statistically significant difference between the two groups. A history of previous biopsy before the procedure and the estimated lesion size significantly differed between the two groups; no other factors did (Table 1).
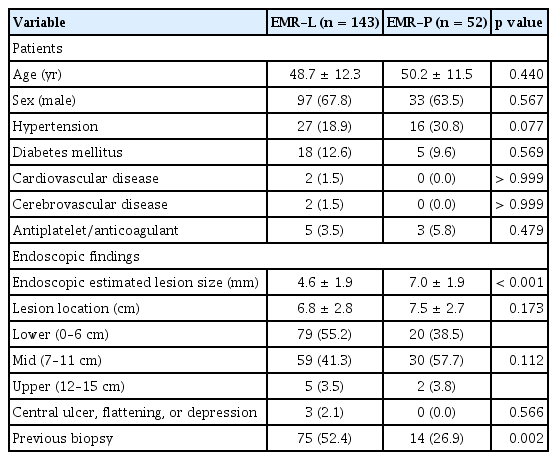
Baseline characteristics of the EMR-L and EMR-P groups
There were no significant differences in en bloc resection rate or complete resection rate (CRR) between the two groups. However, the histologically measured lesion size was significantly larger in the EMR-P group. The rates of positive lateral or vertical margins, depth of invasion, lymphovascular invasion, and tumor grade did not significantly differ between the groups. The mean total procedure time was significantly longer in the EMR-P group. However, hospital length of stay and the occurrence of complications, including post-procedural bleeding, did not show statistically significant differences between the groups. There were no cases of perforation in either group, and no recurrences were observed during the follow-up period (Table 2).
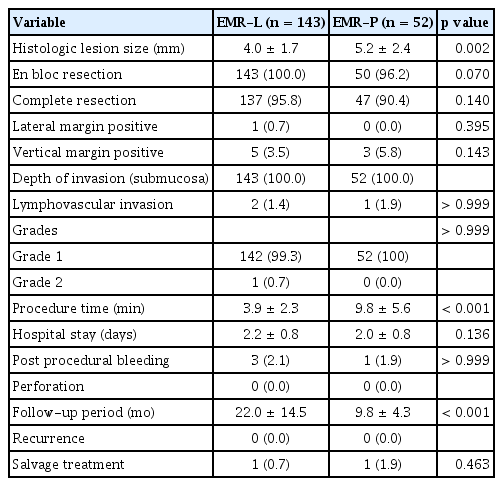
Clinical outcomes
We analyzed potential factors influencing complete resection and found no significant associations with patient-related factors such as age, sex, or underlying comorbidities. Additionally, CRRs did not differ between endoscopic resection methods. En bloc resection was the only factor significantly associated with a higher CRR (p = 0.003) (Table 3).
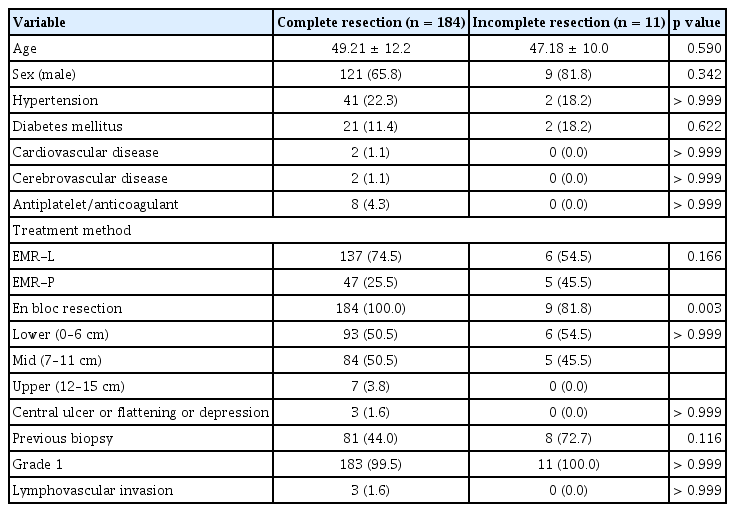
Factors associated with complete resection
In the multivariate logistic regression analysis, previous biopsy was identified as an independent predictor of incomplete resection (odds ratio, 6.30; 95% confidence interval, 1.07–37.08; p = 0.042). Other variables, including age, sex, comorbidities, and resection method, were not significantly associated with incomplete resection (Table 4).
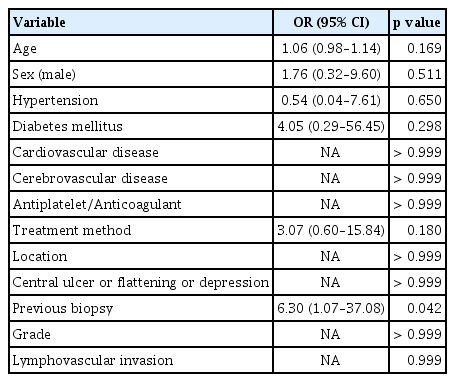
Multivariate logistic regression analysis of factors associated with incomplete resection
DISCUSSION
Treatment strategies for rectal NETs can vary depending on several factors, including tumor size, grade, stage, location, the patient’s general condition, and the endoscopist’s preference. For small rectal NETs ≤ 10 mm, endoscopic resection is the preferred treatment method due to the low risk of lymphovascular invasion, proper muscle layer invasion, regional LNM, or distant metastasis [18]. As a result, the European Neuroendocrine Tumor Society recommends endoscopic resection as the most appropriate treatment for small NETs less than 10 mm in size [10].
Several methods of endoscopic resection are available, which can be broadly categorized into conventional polypectomy, EMR, modified EMR, and ESD. EMR is the most commonly used technique for colon polyp removal. This procedure involves injecting normal saline into the submucosal layer beneath the polyp or tumor to lift it away from the underlying tissue, followed by removal using a snare with electrical current [1]. In contrast, ESD involves dissection of the submucosal layer with an endoscopic knife after submucosal injection; this technique is more challenging than other endoscopic resection methods [19]. Modified EMR is a variation of standard EMR that utilizes additional devices. Depending on the device used, it can be classified as EMR-C, which uses a cap; EMR-L, which employs band ligation; and EMR-P, which involves precutting with an endoscopic knife or snare tip [1].
Conventional polypectomy and EMR are less invasive and technically simple procedures but have a lower CRR than other methods when removing rectal NETs (52.2–84.6%) [20]. This is because rectal NETs are predominantly located in the submucosal layer of the rectal wall, leading to challenging complete resection via these methods [19]. ESD can resect rectal NETs more effectively in cases of deep involvement and has a higher CRR (82.6–100%) relative to EMR [20,21]. However, it needs more time than other methods, requires an experienced endoscopist, and has a higher risk of complications such as perforation and bleeding [1].
Modified EMR methods have demonstrated superior performance compared with conventional EMR, achieving higher CRR and shorter procedure time than ESD. As a result, they have gained widespread adoption for the removal of small rectal NETs [18]. One study showed that EMR-C for rectal NETs (4.6 ± 1.7 mm) resulted in a significantly higher CRR compared with ESD, while also demonstrating a significantly shorter procedure time (3.8 ± 1.2 min vs. 14.4 ± 7.3 min, p < 0.001) [22]. Another study that compared EMR-L (4.4 ± 2.2 mm) and ESD (5.4 ± 2.1 mm) for rectal NETs revealed no differences in CRR, but EMR-L was associated with a significantly shorter procedure time (17.4 ± 4.4 min vs. 28.8 ± 16.2 min, p = 0.5577) and shorter hospital stay (1.8 ± 3.1 days vs. 6.2 ± 2.1 days, p = 0.0162) [23]. EMR-P has also shown promising results. One study detected a CRR of 93.1% for rectal NETs (6.8 ± 2.8 mm) using EMR-P, with a mean procedure time of 9 min, a delayed bleeding rate of 5.6%, and a perforation rate of 0% [18]. Another study comparing EMR-P with ESD for small rectal NETs indicated that EMR-P had significantly shorter procedure times and shorter hospital stays, although the CRR did not significantly differ between the two groups (85.0% vs. 82.8%, p = 0.18) [24].
Few studies have compared the results of modified EMRs for rectal NETs. In one study that compared EMR-L and EMR-C for small rectal NETs, EMR-L showed a slightly (non-significantly) higher CRR. Procedure time and complication rate also did not significantly differ between the two groups [25]. In another study of small rectal NETs, EMR-P and EMR-L were not directly compared, but CRRs were 90.9% in EMR-P and 93.1% in EMR-L, and procedure times were 16.6 ± 8.5 minutes in EMR-P and 10.7 ± 4.3 minutes in EMR-L [26]. A recent network meta-analysis comparing endoscopic resection methods for rectal NETs demonstrated that EMR-L achieved a significantly higher en bloc resection rate than EMR-P, whereas the CRRs were not significantly different between the two techniques. Importantly, the rate of positive vertical margins was significantly higher in EMR-P compared with EMR-L, further supporting the relative technical advantage of EMR-L in achieving deeper and more complete resections [27].
In this study, we compared clinical outcomes between EMR-L and EMR-P for small rectal NETs. CRRs did not significantly differ between the EMR-L group (95.8%) and the EMR-P group (90.4%), consistent with previous studies [23,25,26]. Although the histologically measured size of rectal NETs was significantly larger in the EMR-P group, the average size difference between the two groups was approximately 1.2 mm, which would not have a substantial impact on the results. Interestingly, although the EMR-L group had smaller tumors, it also had a higher rate of prior biopsies. Because biopsy-induced fibrosis can complicate resection, the consistently high en bloc resection rate observed in the EMR-L group suggests that EMR-L may provide a technical advantage for small fibrotic lesions, particularly those ≤ 5 mm. Although our findings are limited, this implication underscores the potential clinical relevance of EMR-L. There were no differences between the two groups in hospital stay or complications such as postprocedural bleeding, perforation, and recurrence. However, total procedure time was significantly shorter in the EMR-L group.
This study has several limitations. First, its retrospective design may have introduced selection bias, as the choice of endoscopic resection method was at the discretion of the endoscopist. Second, although most EMR-P procedures were performed with an oval-type snare (10–15 mm), the type and manufacturer of snares were not standardized across institutions, and these factors could not be fully controlled. In addition, the precutting devices (endoscopic knife or snare tip) used in EMR-P could not be evaluated separately. Third, there was a significant difference in follow-up duration between the EMR-L and EMR-P groups, which may have biased the interpretation of recurrence outcomes. However, as no recurrence was observed in either group, the results remained unchanged when the analysis was restricted to the first 12 months after resection. Fourth, there was an imbalance in lesion size and sample distribution between the two groups. Although multivariate analysis suggested that lesion size was not an independent predictor of incomplete resection, the small number of EMR-P cases limited the statistical power for subgroup analyses. Thus, potential confounding related to lesion characteristics and operator preference cannot be excluded. Taken together, these limitations highlight the need for future large-scale prospective studies with matched cohorts and long-term follow-up to validate our findings.
Despite these limitations, this is the first study to directly compare EMR-L and EMR-P in a relatively large retrospective comparative analysis. Both EMR-L and EMR-P are excellent treatment options for small rectal NETs, offering high CRR, low complication rates, and low recurrence. Therefore, this study provides valuable information for clinicians utilizing these methods. Future studies should involve large-scale, prospective comparative designs with longer follow-up periods; they also should investigate potential differences between the use of an endoscopic knife and a snare tip.
In conclusion, both EMR-L and EMR-P achieved high en bloc and CRRs with a favorable safety profile. However, EMR-L was significantly faster than EMR-P, suggesting that it is a more time-efficient approach for small rectal NET resection.
KEY MESSAGE
1. EMR-L and EMR-P both showed high resection success and safety for small rectal NETs. EMR-L was significantly faster, making it a more time-efficient option.
Notes
CRedit authorship contributions
Sunghyeok Ryou: investigation, software, writing - original draft, funding acquisition; Yunho Jung: conceptualization, methodology, writing - original draft, writing - review & editing; Dae Sung Kim: investigation, validation, funding acquisition; Hee Seok Moon: methodology, formal analysis, software; Hoon Sup Koo: formal analysis, supervision, project administration; Hyun Deok Shin: resources, data curation, validation; Ki Bae Bang: data curation, visualization, project administration; Kyu Chan Huh: conceptualization, resources, writing - review & editing, visualization, supervision
Conflicts of interest
The authors disclose no conflicts.
Funding
This work was supported by the Soonchunhyang University Research Fund.