Hemorrhagic Fever with Renal Syndrome Complicated with Pregnancy: A Case Report
Article information
Abstract
Hantaviruses cause two forms of human disease: hemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome. Hantavirus infection can occur in pregnant women and it can have an influence on the maternal and fetal outcomes, although this is a rare finding even in endemic areas. We describe here a recent case of HFRS complicating pregnancy.
INTRODUCTION
Hantaviruses that belong to the family Bunyaviridae cause two forms of human disease: hemorrhagic fever with renal syndrome (HFRS) and hantavirus pulmonary syndrome (HPS). HFRS manifests as an abrupt onset fever, thrombocytopenia, hemorrhage and acute renal failure1). Several pathogenic hantaviruses including Hantaan virus, Seoul virus, Dobrava virus and Puumala virus are primarily responsible for HFRS in Asia and Europe. In contrast, HPS is a recently recognized disease caused by Sin Nombre virus in America2). This syndrome is characterized by an acute progressive noncardiogenic pulmonary edema that often resembles acute respiratory distress syndrome. All the hantaviruses are associated with a primary rodent reservoir, and human infections occur after the inhalation of the aerosolized virus that's excreted in rodent urine and feces.
Hantavirus infection can be fatal in pregnant women. Moreover, infectious agents traversing the placenta can infect the fetus and seriously affect the fetal health status. However, the effects of hantavirus infection on the maternal and fetal outcomes have not been well studied. We describe here a case of HFRS complicating pregnancy and we review the other Korean cases of HFRS in pregnant women.
CASE REPORT
A 31-year-old, otherwise healthy, woman, (gravida 0 and para 0), at 15 weeks of gestation was admitted to our hospital on October 29, 2004 due to fever, chills, eyeball pain and back pain of 4 days' duration. The patient had undergone intrauterine insemination on June 24, 2004 before achieving pregnancy. She began to complain of facial edema and blurred vision just after admission. She denied having a cough, diarrhea or dysuria. She and her husband were beef cattle-breeders in the rural Yangju area of Gyeonggi Province, Korea. On examination, her blood pressure was 110/80 mm Hg and her temperature was 38.3℃. She displayed flushing of the face, conjunctival hemorrhage and bulbar conjunctival edema. Her chest auscultation was normal. Mild tenderness was bilaterally found on her costovertebral angle, but no skin rash was evident. The laboratory tests revealed the following: leukocyte count: 21,300/µL (normal range: 4,000-10,000/µL), platelets: 83,000/µL (normal range: 150,000-400,000/µL), creatinine: 0.9 mg/dL (normal range: 0.7-1.4 mg/dL), aspartate transaminase: 67 U/L (normal range: <40 U/L), sodium: 135 mmol/L (normal range: 135-145 mmol/L), and potassium: 3.8 mmol/L (normal range: 3.5-5.5 mmol/L). Urinalysis revealed proteinuria and hematuria. Cultures of her blood and urine were sterile. Fetal ultrasound showed fetal growth that was consistent with the gestation dates.
Her condition deteriorated over the following days. Her blood pressure dropped to as low as 60/40 mmHg despite massive administration of physiologic saline on day 2, and her platelet count decreased to 15,000/µL on day 5. Her oliguria and elevated serum creatinine levels of up to 4.2 mg/dL necessitated the administration of diuretics intermittently from day 3 to day 7. However, from day 8 her renal functions progressively improved. The patient recovered completely and was discharged on day 14. The antibody titer for Hantaan virus, which was determined using a high-density particle agglutination test (Hantadia, Greencross, Korea) was 1:640 on day 5. A repeat titer showed an increase to 1:2,560 at the time of discharge, but it was 1:1,280 two weeks after discharge. Serologic tests for Leptospira, Orientia tsutsugamushi and HIV were negative.
The pregnancy continued uneventfully, and the patient was lost to follow-up. Six months later, she vaginally delivered a 2,900-g healthy female infant without complications at another hospital. However, no additional tests for Hantaan virus were performed on her or her baby at the time of delivery.
DISCUSSION
Hantavirus infection that complicates pregnancy has rarely been reported in the literature3-10), although hantavirus infections in some women can lead to obstetric and fetal complications.
In Korea, only 8 cases of HFRS complicating pregnancy (including the present case) have been reported11-16). These are summarized in Table 1. The gestational age at the time of diagnosis ranged from 15 to 29 weeks, and none of the reported patients showed evidence of abnormal fetal development, distress or pregnancy complication before presentation. Of these 8 cases, the pregnancies did not achieve full-term in three of the pregnant women, and it's interesting that they were all in the early third trimester of pregnancy when they contracted the disease. These three pregnancies resulted in intrauterine fetal death, preterm delivery but fetal death after birth, and preterm cesarean section, respectively11, 13, 16). Among these cases, only one case of transplacental transmission of Hantaan virus was confirmed both serologically and pathologically13). In another case, the stillborn infant showed strong pathological evidence of Hantaan virus infection11). However, it could be argued that in this case any serologic testing of the fetus was not performed and the autopsy findings were consistent with those seen for pregnant women with other illnesses that cause profound hypotension17). In the other cases, including our case, the presence of transplacental Hantaan virus transmission remains unknown because the appropriate fetal laboratory tests were not performed.
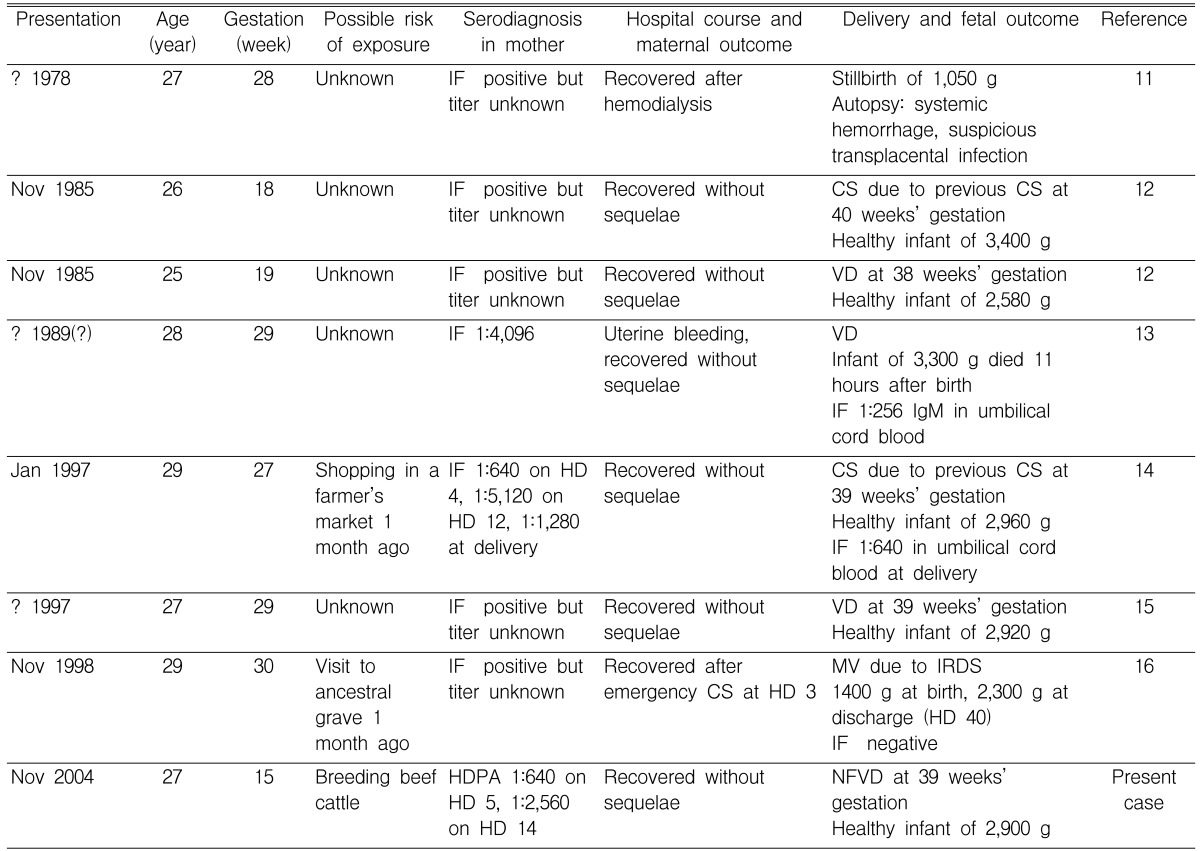
Summary of Eight Cases of HFRS Complicating Pregnancy in Korea
The maternal and fetal outcomes of pregnancy complicated by HFRS have also been reported in China, where the most severe form of HFRS caused by Hantaan virus occurs (the same form occurs in Korea)18-20). One of these China studies suggested there was maternal-to-fetal transmission, but the fetal infection was not unequivocally confirmed by any pathological and/or serological evidence19). Nevertheless, in a previous report, post-natal deformity was not observed in healthy babies born naturally to mothers who recovered from HFRS20).
Infections caused by other hantaviruses such as Puumala virus3-6) and Sin Nombre virus7-10) during pregnancy have also been noted. There have been no reported cases of HFRS caused by Puumala virus that led to fetal death3-6). A case series of HPS in pregnancy showed that some Sin Nombre virus infections caused fetal complications, including fetal death in utero7). In contrast with Hantaan virus infections in pregnancy, there is no evidence of transplacental transmission to the fetus for Puumala virus or Sin Nombre virus3-7, 9, 10). For example, in a recent study of 5 pregnant women with HPS, one case of maternal death and 2 cases of fetal loss were identified, but no histopathologic and/or serological evidence for the vertical transmission of Sin Nombre virus was found in any case7).
These findings of hantavirus infection in pregnancy might suggest that Hantaan virus infection has a higher risk of transplacental transmission than other infections caused by other hantaviruses, but that this rate is still low. It might also be suggested that infections caused by Hantaan virus and Sin Nombre virus in pregnant women are more likely to cause severe fetal complications than does Puumala virus. However, these suggestions remain speculative because only a small number of cases of hantavirus infections in pregnant women have been reported in the literature to date.
In conclusion, hantavirus infection during pregnancy, especially that caused by Hantaan virus, can cause unfavorable obstetric and fetal outcomes. Although hantavirus infection occurs only rarely during pregnancy, this condition should be considered in the differential diagnosis involving fever, thrombocytopenia, hemorrhagic manifestations and acute renal failure in pregnancy, and especially when these symptoms are seen in an endemic area.