Asymptomatic Disseminated Cysticercosis in an Immunocompetent Patient
Article information
A 68-year-old previously healthy man presented with chest discomfort. He was diagnosed with angina pectoris. Chest radiography showed multiple rice-like subcutaneous calcifications (Fig. 1A). The patient confirmed that he had observed these subcutaneous nodules all over his body, which showed no change in number and size for over 10 years (Fig. 2A). He lived in a rural area where pigs are raised and was fond of consuming pork; further, he confirmed having no past history of seizures and tuberculosis. Total serum immunoglobulin E level was 19.1 IU/mL. Blood enzyme-linked immunosorbent assay for Taenia solium was negative for cysticercosis IgG antibodies. Stool examination showed normal results. For evaluation of neurocysticercosis, brain computed tomography scan was performed, and a few dot-like calcified lesions in the brain parenchyma was observed (Fig. 1B). Femur radiography showed numerous oval-shaped calcifications in the thigh soft tissue (Fig. 1C). Analysis of subcutaneous tissue biopsy specimen from the upper left arm showed a well demarcated encapsulated calcific nodule in intramuscular area (Fig. 2B and 2C). On the basis of the above results, we made a final diagnosis of disseminated cysticercosis. However, the patient presented only palpable subcutaneous nodules, and the diagnosis of disseminated cysticercosis was an incidental finding. No antiparasitic therapy was initiated, and the patient showed no complication at 7 months after diagnosis.
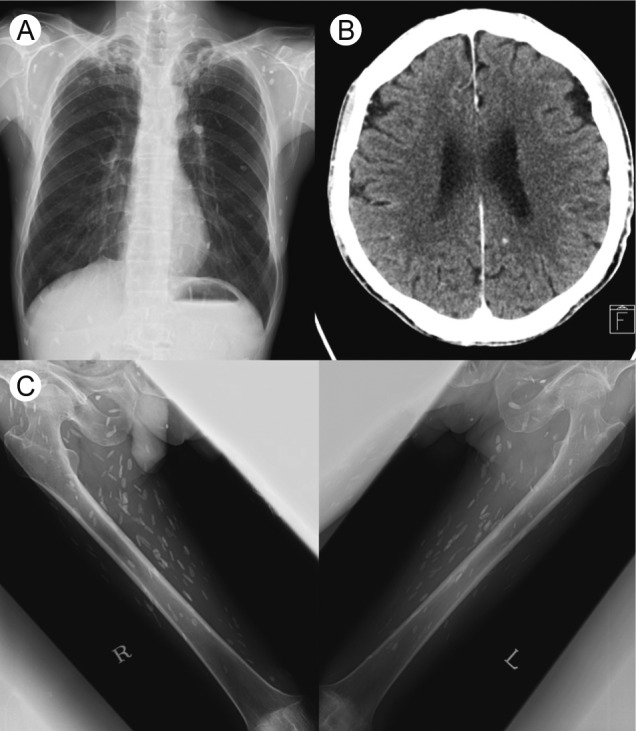
(A) Chest radiography showing multiple rice-like subcutaneous calcifications. (B) Brain computed tomography showing a few dot-like calcified lesions in the brain parenchyma. (C) Femur radiography showing numerous oval-shaped calcifications in the soft tissue of the thigh.
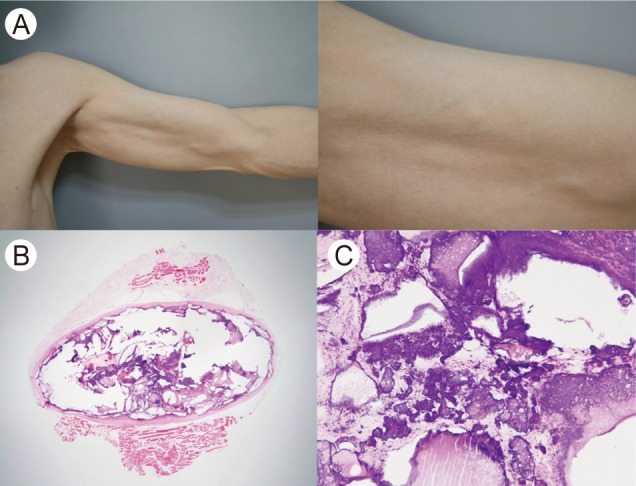
(A) Subcutaneous nodules were observed all over his body, but had not changed in number or size for more than 10 years. (B, C) Subcutaneous dystrophic calcification was demonstrated in the subcutaneous tissue biopsy specimen from the upper left arm (B: H&E, × 12.5; C: H&E, × 200).
Acknowledgments
The authors wish to thank Dr. Jeong Hyeon Lee, the Department of Pathology, Korea University Anam Hospital for the helpful pathological review.
Notes
No potential conflict of interest relevant to this article was reported.