


INTRODUCTION
The benign tumors found in the tracheobronchial tree are approximately 2% of all the lung tumors1, 2). They often cause partial or complete bronchial obstruction, and this results in cough, dyspnea and recurrent pneumonia. Surgical resection with bronchoplastic reconstruction has long been the standard treatment. After the Nd-YAG laser was first applied by Toty and colleagues in 19783), bronchoscopic surgery has seen new techniques and methods applied to treat endobronchial tumors4-7). Nowadays, the improving techniques of therapeutic bronchoscopy have been replacing conventional surgery for the treatment of intra-bronchial benign tumor.
However, for the patients with complete bronchial obstruction, there could be some limitations for performing bronchoscopic intervention. When a tumor completely obstructs the bronchial lumen, it is difficult not only to remove the tumor with an endoscopic procedure, but also to evaluate the distal airways7). Generally, bronchoscopic removal of endobronchial tumor is preferable when the tumor is small or pedunculated8).
To evaluate the role of endoscopic surgery for completely obstructive endobronchial benign tumor, we retrospectively reviewed the medical records of the patients who underwent bronchoscopic resection due to their completely obstructive benign tumors.
MATERIALS AND METHODS
From January 1999 to May 2004, 7 patients underwent bronchoscopic resection due to completely obstructive benign tumor at Samsung Medical Center, Seoul, Korea. We selected patients for bronchoscopic surgery when three criteria were met: 1) the tumor was pathologically benign, 2) it was bronchoscopically accessible and 3) it was confined within the bronchial cartilage.
Before bronchoscopic surgery, all the patients were examined by computed tomography (CT) and flexible bronchoscopy (BF200; Olympus; Tokyo, Japan). A written informed consent was obtained from all the patients.
Rigid bronchoscopy was performed under general anesthesia with using intravenous propofol injection. After a rigid bronchoscope tube (Hopkins, Karl-Storz, Germany) was intubated through the vocal cords, a rigid (Hopkins, Karl-Storz, Germany) or flexible bronchoscope (EVIS BF 1T240, Olympus, Japan) was introduced for manipulation. After the stalk of the tumor was identified with using flexible biopsy forceps (FB-21C-1, Olympus, Japan) as a probe, a Nd-YAG laser (20 watt, LaserSonics, Model 1000, USA) was applied using a G56D non-contact fiber (LaserSonics, USA). The mass was then resected using a bronchial snare or forceps. After removing of the mass, additional laser cauterization was carried out to remove any residual lesion and to control the bleeding.
The clinical outcome was defined as being successful when the bronchial lumen was reopened to more than 70% of the original diameter and the collapsed distal lung was seen to resolve on chest X-ray.
After bronchoscopic intervention, serial follow-up was done with using chest X-ray. Chest CT and flexible bronchoscopy were added to the follow-up when there was any suspicion of disease recurrence.
RESULTS
Clinical Characteristics
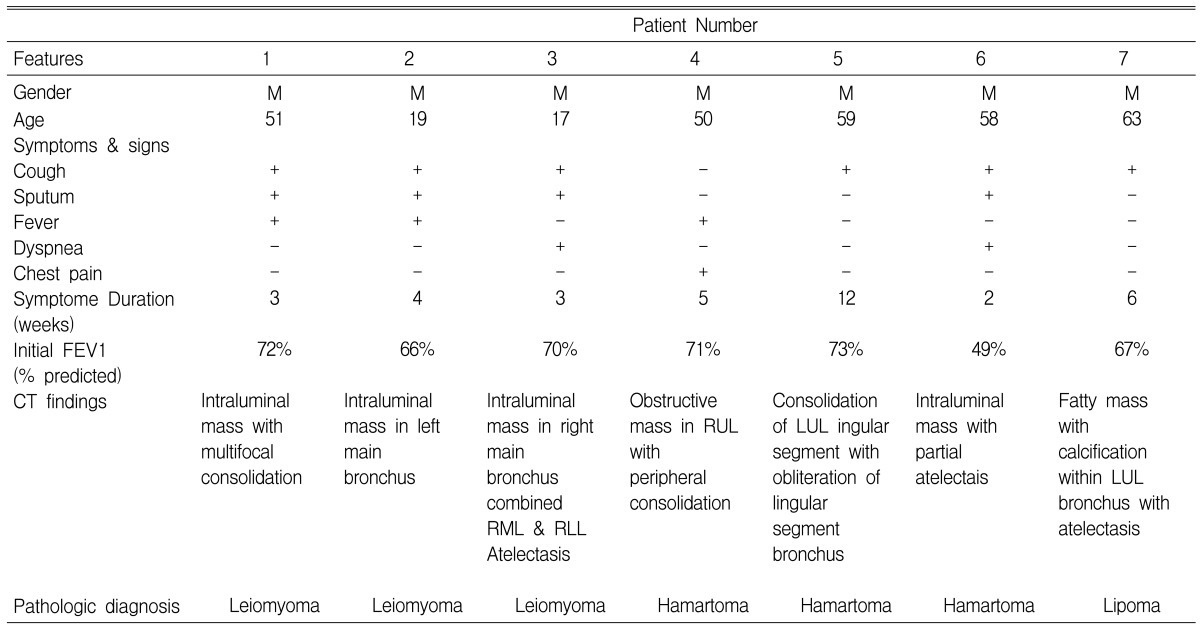
The median age of patients was 51 years (range: 17-63) and all the patients were male.
The common clinical symptoms were cough (n=6, 85.7%), sputum (n=4, 71.4%), fever (n=4, 71.4%) and dyspnea (n=2, 28.5%). The median symptom duration of these patients was 4 weeks (range: 2 to 12 weeks). Four patients were managed with antibiotics under the clinical impression of pneumonia. Three patients suffered from chronic cough and mild dyspnea. The pulmonary function testing revealed a mild obstructive pattern in 4 patients. Chest CT showed an endobronchial mass with atelectasis in 3 patients and only peripheral consolidation in 3 patients.
The histopathologic diagnoses were 3 leiomyomas, 3 harmatomas and 1 lipoma (Table 1). The location of the tumor was the lobar bronchus in 3 patients and the main bronchus and segmental bronchus in 2 patients, respectively. All the patients showed completely obstructive endobronchial mass upon bronchoscopic examination (Table 2, Figure 1).
Initial Outcome
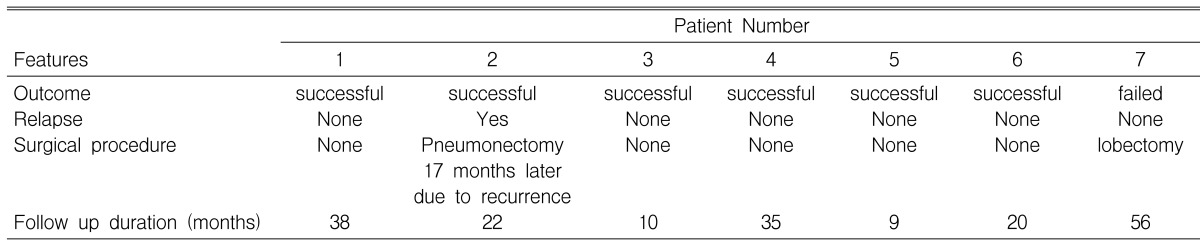
Bronchoscopic resection was successful in 6 out of the 7 patients (85.7%). For the 1 unsuccessful patient (patient 7), the location of the tumor was the lobar bronchus of the left upper lobe. Due to the very acute angulation of the left upper lobe of the patient, the mass could not be grasped with using any kind of endobronchial tools. The patient then underwent open thoracotomy and left upper lobe lobectomy.
Including the 1 unsuccessful patient, there was no mortality in all 7 patients. Pneumomediastinum developed in 1 patient (patient 2) just after the procedure. The patient was successfully treated with 3 days of oxygen therapy.
Follow-up and Recurrence
The duration of follow up was a median of 35 months (range: 9-56 months). In 5 out of the 6 successful patients, there was no recurrence during follow-up. In 1 patient (patient 2, the same patient in whom pneumomediastinum developed), recurrence of a leiomyoma was diagnosed by chest CT and bronchoscopy 17 months after the bronchoscopic surgery. As the leiomyoma was in the proximal left main bronchus, the patient underwent left pneumonectomy. The pathology after performing pneumonectomy showed a leiomyoma confined within the bronchial cartilage. After surgery, there was no complication for 17 months (Table 3).
DISCUSSION
In this study, endoscopic surgery was effective for most of the patients (6/7, 85.7%) who suffered with completely obstructive endobronchial benign tumor. In addition, the complication rate and late recurrence rate was 16.7%, respectively. When considering the morbidity of open thoracotomy, endoscopic surgery can be primarily selected for the patients with endobronchial benign tumor.
Bleeding was probably the most dangerous complication when the tumor was resected with bronchoscopy, even when the rigid bronchoscopy was performed under general anesthesia. To prevent arterial bleeding, bronchoscopists usually pre-coagulate the stalk of the tumor before the resection. For a completely obstructive endobronchial tumor, it is not easy to identify the stalk or the base of the tumor. We used flexible bronchoscopic biopsy forceps (FB-21C-1, Olympus, Japan) as a probe. Even though the bronchial lumen was completely obstructed by tumor, there could be a gap between the mass and bronchial wall. We tried to penetrate the biopsy forceps at 0, 90, 180 and 270 degrees around the mass and we were able to identify the base of the tumor by feeling resistance or touch bleeding. Then laser coagulation, mechanical resection and laser cauterization could be performed step-by-step without dangerous tumor bleeding or bronchial tearing.
Reports on the bronchoscopic removal of benign bronchial tumors have recently been increasing9-11). A large series of reports was done by Shah et al in 19952). In the 185 patients with endobronchial benign tumors, 62% experienced a "very good result" with laser resection and 38% showed a "good result". There have also been several reports about the treatment results after bronchoscopic surgery in the patients with benign endobronchial tumors12-14).
Although all of these reports suggest that bronchoscopic treatment is a good therapeutic choice for endobronchial benign tumor, there are some limitations. First, certain tumors can extend outside the cartilage. Second, there are sometimes difficulties to obtain the definitive diagnosis and there is the possible complicated histology with a malignant tumor. Finally, there are technical problems in the treatment of completely obstructive endobronchial benign tumor. A major problem in completely obstructive tumor is the difficulty in determining the correct route for recanalization into the completely obstructed bronchus, and the state of the distal lung is often unknown7). Therefore, in many completely obstructive cases, surgical treatment is preferably considered15-17). Further, there is a tendency to reserve bronchoscopic surgery for those patients who have either a small, narrow pedicle or movable lesions12, 17). However, we know how to identify the base of a tumor for completely obstructive endobronchial benign tumors and we removed them successfully.
Complications of the endoscopic surgery are pneumomediastinum or pneumothorax caused by perforation of the bronchus, uncontrolled bleeding, air embolism and cicartrical injury after excessive laser cauterization and cardiovascular instability6, 18, 19). There were no major complications in our cases, except for the one patient with leiomyoma who developed pneumomediastinum. In addition, this patient who developed pneumomediastinum was successfully treated with simple oxygen therapy. The same as reported by the previous studies, the risk of complication with this procedure is not so high2, 10, 20). In addition, cicartrical injury was not observed on follow-up when bronchoscopy was performed after we did meticulous laser cauterization.
In this study, 1 patient showed late recurrence of bronchial leiomyoma 17 months after the endoscopic surgery. Fortunately, the pathology after pneumonectomy showed that the leiomyoma was confined within the bronchial cartilage and there has been no complication after pneumonectomy until now. It was the same patient in whom pneumomediastinum developed after bronchoscopic intervention. Although there was no evidence, this recurrence could be associated with performing a less meticulous endoscopic surgery on this patient.
Although our experiences are small in number and the follow up duration was not long enough, this study could contribute to widening the application of bronchoscopic surgery for completely obstructive intrabronchial benign tumor. We hope that our findings will help prevent unnecessary surgery in the patients with completely obstructive endobronchial benign tumor.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





