


INTRODUCTION
Metabolic syndrome (MetS) is a phenomenon wherein the risk factors of cardiovascular diseases, such as obesity, impaired glucose tolerance, atherogenic dyslipidemia and hypertension, appear simultaneously in one individual [1]. MetS is highly prevalent and its incidence is increasing rapidly. The prevalence of MetS among Korean adults greater than 20 years of age increased from 24.9% in 1998 to 31.3% in 2007 according to data from the Korean National Health and Nutrition Survey [2].
The key pathophysiological mechanisms of MetS include insulin resistance and visceral obesity [3]. In addition, prothrombotic and proinflammatory states are essential features of MetS. MetS may increase cardiovascular disease risk and progression via changes in adipocytokines, inflammatory markers, and oxidative stress by cross-talk between adipocytes, inflammatory cells, and endothelial cells [4-7].
Mild or severe hyperglycemia, compensatory hyperinsulinemia to overcome insulin resistance, and imbalances in intracellular insulin signaling pathways (such as the phosphatidylinositol 3-kinase pathway and the mitogen-activated protein kinase pathway) have been argued to be the mechanisms by which insulin resistance is involved in the occurrence of MetS [3]. High-sensitivity C-reactive protein (hs-CRP), a representative acute phase reactant, is a marker of atherosclerosis and endothelial cell dysfunction. Several studies have demonstrated that hs-CRP is a strong predictor and prognostic factor of future cardiovascular disease and is associated with the components of MetS [8,9]. In contrast, adiponectin is a plasma adipocytokine that is normally present at levels of up to 5 to 10 µg/mL on average and is known to prevent atherosclerotic vascular changes and impairments of glucose and lipid metabolism. Decreased plasma levels of adiponectin in subjects with visceral fat accumulation are associated with an increased cardiovascular risk [10].
Oxidative stress causes an imbalance in the ratio of reactive oxygen species to reactive nitrogen species (ROS/RNS) and antioxidants, and occurs when the net ROS/RNS exceeds the antioxidant capacity. Excessive ROS/RNS is related to various pathophysiological conditions, including atherosclerosis, diabetes, obesity, and cancer, by reducing biological activity and by altering metabolic dysregulation, cell signaling, and other cellular functions [11-14]. Oxidative stress may play a critical role in the development of MetS and act a mechanistic link between MetS and related cardiovascular diseases. Many studies have demonstrated that increased oxidative stress is the underlying cause of MetS development [13,15,16]. Nevertheless, few studies have investigated the relationships between the total antioxidant status and metabolic risk factors in Korean adults [17].
The aims of this study were to examine the differences in antioxidant capacity, as measured by biological antioxidant potential (BAP), according to the presence of MetS and to characterize the association between antioxidant capacity and insulin resistance, inflammatory markers, and adipocytokines related to MetS.
METHODS
Study subjects
A total of 92 subjects (47 control subjects and 45 MetS subjects) were selected from participants of a previous clinical study on the association between MetS/adiponectin and insulin resistance. The subjects were recruited into the previous study through advertisements for healthy adults residing in southern Gyeonggi Province and the outskirts of Seoul from June 2009 to October 2010. A total of 596 individuals aged 30 to 59 years with no history of cardiovascular disease, diabetes, hypertension, dyslipidemia, cancer, or medical treatment were enrolled. The subjects were healthy Koreans who had completed demographic information surveys, physical measurements, laboratory tests, and nutrition surveys. Of these, 50 subjects with MetS were sampled randomly, and an age- and sex-matched control group was selected from subjects without MetS to identify differences in antioxidant capacities according to the presence of MetS. A total of 92 (45 male and 47 female) subjects were included in the final analysis after excluding eight individuals whose adiponectin levels were unknown.
This study was approved by the Institutional Review Board of Bundang Jesaeng Hospital, and written informed consent was received from each participant.
Measurements
Body weight and height were measured with an automatic height and weight scale (GL-150, G-Tech International, Uijeongbu, Korea). Waist circumference was measured at the high point of the iliac crest with minimal respiration to the nearest 0.1 cm. Blood pressure was measured with a sphygmomanometer (EW3152, Panasonic, Tokyo, Japan) in the sitting position after a 5-minute rest. The body mass index (BMI) was calculated by dividing the body weight (kg) by the square of the height (m).
Venous blood was collected after at least 8 hours of fasting. The triglyceride (TG), high density lipoprotein cholesterol (HDL-C), and fasting blood glucose (FBG) levels were measured using an enzymatic colorimetric test (GPO-PAP), the enzymatic method, and the HKG6PD (UV) method, respectively. Serum insulin levels were measured using an electrochemiluminescence immunoassay, and insulin resistance was assessed by the homeostatic model assessment for insulin resistance (HOMA-IR) index using the following formula: fasting insulin (µIU/mL) × fasting plasma glucose (mmol/L) / 22.5 [2]. Plasma levels of adiponectin were measured using a commercially available enzyme-linked immunosorbent assay kit. The hs-CRP levels were measured using the turbidimetric immunoassay method. Interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α) were measured using enzyme immunoassay methods.
Antioxidant capacity
The BAP test (Diacron International s.r.l., Grosseto, Italy), measured using an automatic chemistry analyzer (Hitachi 7180, Hitachi Ltd., Tokyo, Japan), was employed to assess the antioxidant capacity. The test can be performed on venous serum, and it examines the blood concentration of antioxidants as agents that can reduce iron from the ferric (Fe3+) to ferrous (Fe2+) form. We estimated the intensity of this chromatic change photometrically. The coefficient of variation of the BAP test, based on reproducibility tests, ranged from 2.72% to 2.91%. Based on the existing reference level, an antioxidant capacity of < 2,000 µmol/L is considered to indicate reduced effectiveness of the antioxidant plasma barrier during oxidation, which is a marker of oxidative stress [18]. In this study, reduced antioxidant capacity was defined as an antioxidant capacity of < 2,000 µmol/L determined using the BAP test.
Definition of MetS
MetS was defined as the presence of three or more of the following criteria based on the National Cholesterol Education Program Adult Treatment Panel III (NCEP ATP III) guidelines: 1) abdominal obesity, waist circumference of ≥ 90 cm in men or ≥ 85 cm in women; 2) hypertriglyceridemia, serum TG concentration of ≥ 150 mg/dL; 3) low HDL-cholesterolemia, serum HDL-C concentration of < 40 mg/dL in males, or < 50 mg/dL in females; 4) high blood pressure, systolic blood pressure of ≥ 130 mmHg, and diastolic blood pressure of ≥ 85 mmHg; and 5) high fasting glucose, serum glucose concentration of ≥ 100 mg/dL. The cutoff value for abdominal obesity was defined using guidelines from the Korea Society for the Study of Obesity [19].
Statistical analysis
All statistical analyses were performed using Stata SE 10.0 (Stata, College Station, TX, USA). The values are presented as means ± standard errors for continuous variables and as numbers (%) for categorical variables. When the data were not distributed normally (i.e., adiponectin, HOMA-IR score, and hs-CRP), they were transformed logarithmically prior to statistical analysis.
The continuous variables were compared using a t test. The categorical variables were compared using a chi-square test. Linear regression analysis was performed to evaluate the associations between reduced antioxidant capacity and adiponectin, insulin, HOMA-IR score, hs-CRP, IL-6, and TNF-α after adjustments for age and sex. A multivariate logistic regression analysis was used to assess the independent predictors of MetS, including the association between MetS and antioxidant capacity, adiponectin, HOMA-IR, IL-6, TNF-α, and hs-CRP after adjustments for age and sex. A p < 0.05 was considered to indicate statistical significance.
RESULTS
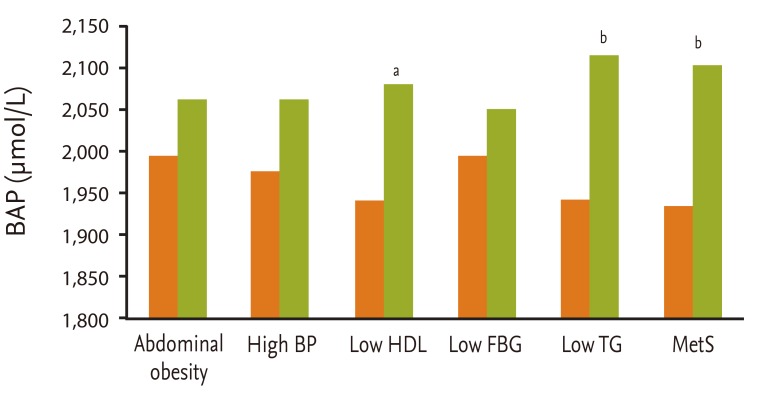
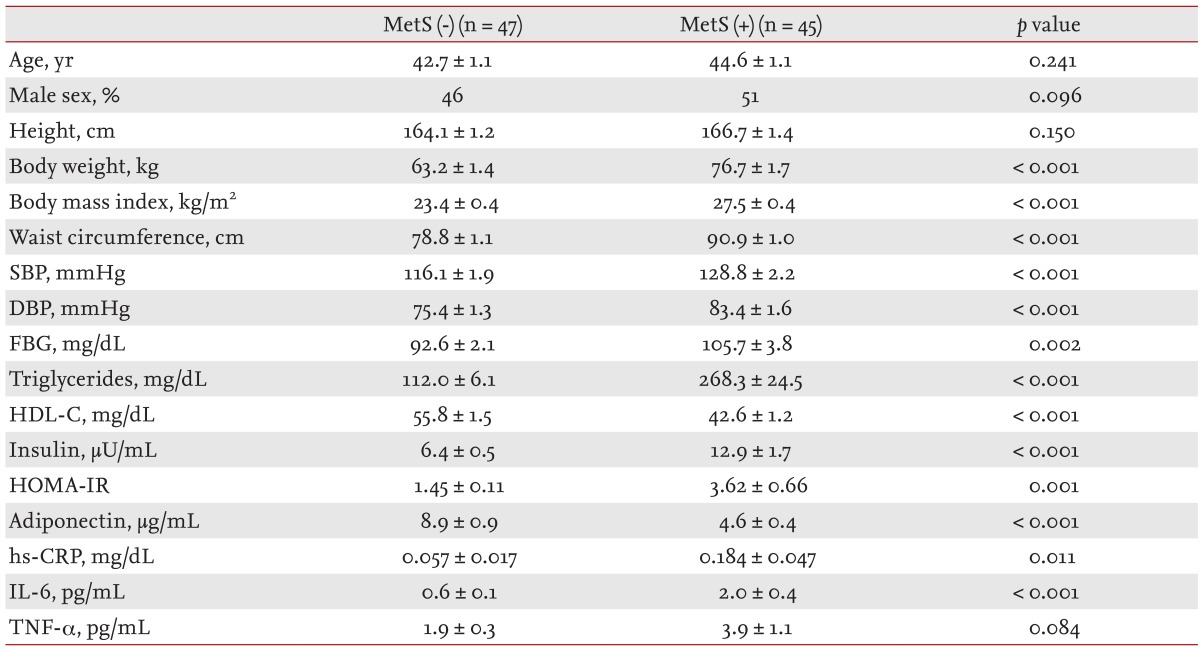
The general and biochemical characteristics of the study subjects according to MetS status are presented in Table 1. Subjects with MetS showed a significantly higher waist circumference (p < 0.001), BMI (p < 0.001), TG (p < 0.001), and HOMA-IR (p = 0.001), and lower HDL-C (p < 0.001) and adiponectin (p < 0.001) compared to those without MetS. Antioxidant capacity according to the presence of MetS and its components is depicted in Fig. 1. The mean BAP of the MetS group was 1,937.3 µmol/L, significantly lower than that of the non-MetS group. Whereas the mean BAP values of the low HDL (1,941.4 µmol/L vs. 2,081.0 µmol/L; p = 0.011) and high TG groups (1,942.3 µmol/L vs. 2,115.9 µmol/L; p < 0.001) were significantly lower than those in subjects with high HDL or low TG, the mean BAP values of the abdominal obesity, high BP, and high FBG groups were not significantly different.
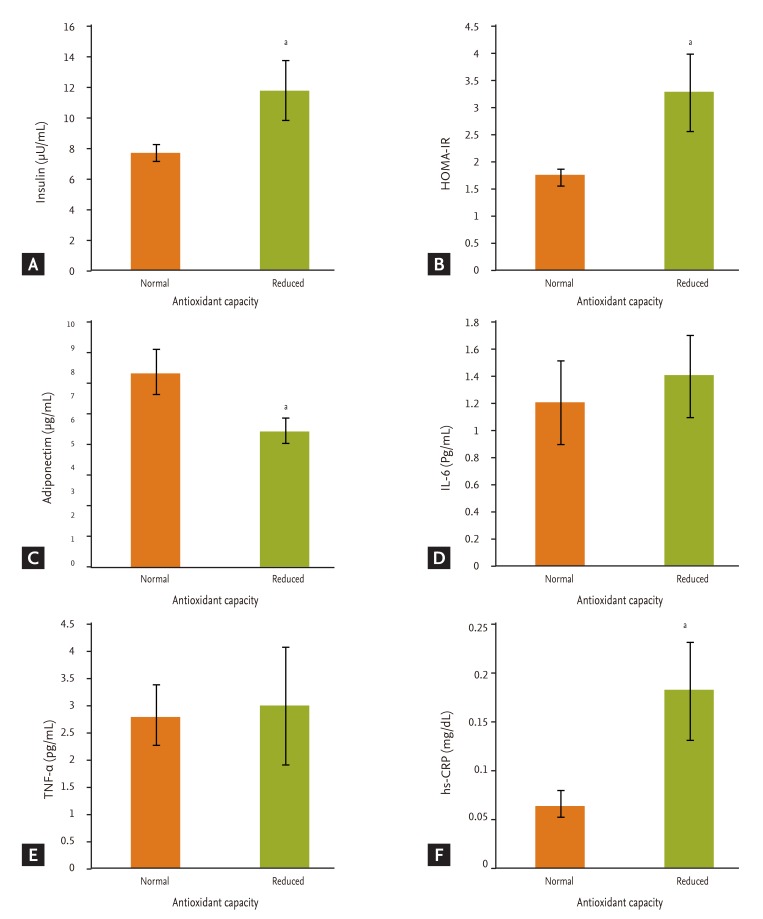
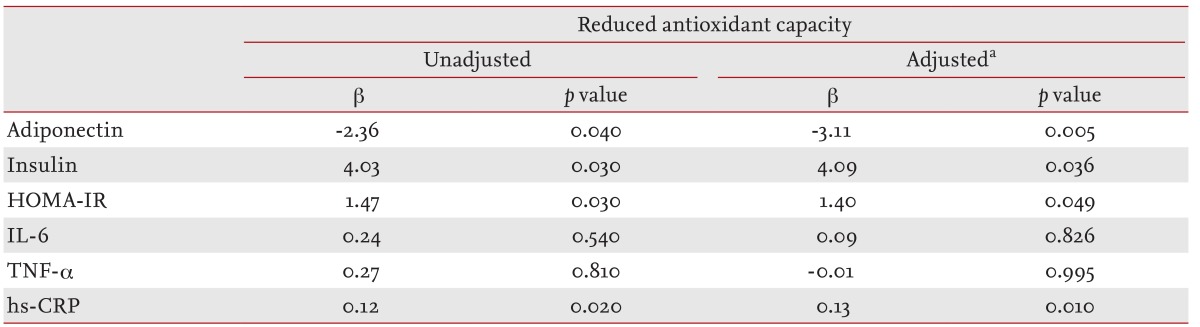
Fig. 2 presents the differences in insulin, HOMA-IR, hs-CRP, IL-6, TNF-α, and adiponectin levels according to antioxidant capacity. There were 42 persons (45.7%) with reduced antioxidant capacity and 50 (54.3%) with normal antioxidant capacity. The insulin (11.8 ± 1.9 µU/mL vs. 7.7 ± 0.6 µU/mL; p = 0.033), HOMA-IR (3.32 ± 0.72 vs. 1.84 ± 0.15; p = 0.032), and hs-CRP levels (0.183 ± 0.052 mg/dL vs. 0.066 ± 0.013 mg/dL; p = 0.020) in the reduced antioxidant capacity group were much higher than those in the normal antioxidant capacity group. The adiponectin level (5.5 ± 0.5 µg/mL vs. 7.9 ± 0.9 µg/mL; p = 0.036) was significantly lower in the reduced antioxidant capacity group. A multivariate linear regression analysis was performed to evaluate the association between reduced antioxidant capacity and inflammatory markers and adipocytokines (Table 2). After adjusting for age and sex, the reduced antioxidant capacity was negatively associated with adiponectin (β = -3.11, p = 0.017) and positively associated with HOMA-IR (β = 1.40, p = 0.049) and hs-CRP (β = 0.13, p = 0.010).
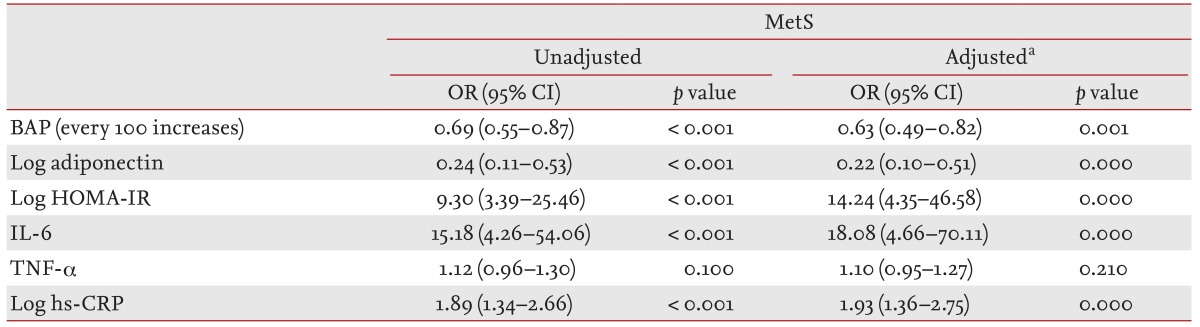
Table 3 lists the odds ratios (ORs) for MetS according to BAP, adiponectin, HOMA-IR, IL-6, TNF-α, and hs-CRP. The ORs for MetS with BAP and log adiponectin were 0.63 (95% confidence interval [CI], 0.49 to 0.82; p = 0.001) and 0.22 (95% CI, 0.10 to 0.51; p = 0.000), respectively; whereas the ORs for MetS with log HOMA-IR, IL-6 and log hs-CRP were 14.24 (95% CI, 4.35 to 46.58; p = 0.000), 18.08 (95% CI, 4.66 to 70.11; p = 0.001), and 1.93 (95% CI, 1.36 to 2.75; p = 0.001), respectively, after adjusting for age and sex.
DISCUSSION
In this study, we found that subjects with MetS showed a reduced antioxidant capacity that was significantly correlated with lower adiponectin and higher HOMA-IR and hs-CRP levels.
Among the individual components of MetS, the groups with low HDL or high TG showed significantly lower antioxidant capacities. Previous studies have consistently shown that oxidative stress is significantly associated with dyslipidemia [20-23]. Vassalle et al. [20] also demonstrated that oxidative stress, as measured by the the derivatives of the reactive oxigen metabolites test and the OXY-adsorbent test, is significan tly correlated with hypertriglyceridemia. Hansel et al. [21] showed that MetS is associated with elevated oxidative stress through dysfunctional dense HDL-C.
Several studies that examined the association between oxidative stress and MetS reported that high blood pressure was also significantly associated with oxidative stress [1,13,16,20,24,25]. However, our results did not show a difference in antioxidant capacity according to blood pressure. The antioxidant/oxidant balance is known to be normally involved in the pathogenesis of hypertension by contributing to endothelial dysfunction [13].
The reduced antioxidant capacity group had significantly higher insulin and HOMA-IR scores compared to those of the normal antioxidant capacity group, but the BAP level of the high FBG group was not significantly different from that of the normal FBG group. In a study of the effects of hyperglycemia on oxidative stress (measured by the reactive oxidative metabolites [ROM] test) and antioxidant potential (measured by the BAP test) in patients with type 2 diabetes, the mean BAP level in patients with type 2 diabetes was not different from that in the control group, but the ROM level in patients with type 2 diabetes with MetS was signif icantly higher than that in patients without MetS [26].
Among adiponectins, hs-CRP, IL-6, and TNF-α, which are useful predictors of MetS risk [27-29], low adiponectin and high hs-CRP were closely related to a reduced antioxidant capacity in our study. These results are similar to those of previous studies regarding the relationship between these indicators and antioxidant capacity, although direct comparisons might be somewhat difficult because different methods of measuring oxidative stress and antioxidant capacity were used [13,20,30,31]. Furukawa et al. [15] demonstrated that increased oxidative stress in accumulated fat could cause dysregulation of the production of adipokines, such as adiponectin, plasminogen activator inhibitor-1, IL-6, and TNF-α. In this study, however, there were no significant associations between IL-6 or TNF-α and reduced antioxidant capacity.
An increase in BAP was significantly associated with a lower OR for MetS (OR, 0.63; 95% CI, 0.49 to 0.82; p = 0.001), as shown in Table 3. Recently, the BAP test has been used; it measures the ability of a plasma sample to reduce ferric to ferrous ions and evaluates the BAP of plasma. The BAP test provides results that are largely comparable to those of the FRAP test, against which it appears to be faster and simpler to perform [32]. It is known to be useful for measuring oxidative stress in healthy individuals, as well as oxidative stress-related diseases, and for monitoring of the efficacy of antioxidant treatments. As the importance of MetS as a risk factor for developing cardiovascular disorders and diabetes is known, it is being focused on in the prevention of the onset of these diseases by means of early detection with the assessment of known pathophysiologies, such as insulin resistance, hypoadiponectinemia, and so on [1]. Considering that oxidative stress plays an important role in the development of MetS and cardiovascular complications, measuring the antioxidant barrier potential can help to identify subjects with MetS and related cardiovascular diseases.
Our study has several limitations. First, we could not consider lifestyle factors, such as smoking, nutrient intake, and alcohol intake, which are known to be associated with MetS, as well as oxidative stress. Another limitation is the small sample size. Third, our results do not provide information on a causal relationship due to the cross-sectional design of the study. However, the strength of this study is the use of precise biomarker assays.
In conclusion, MetS was signif icantly associated with reduced antioxidant capacity. The BAP test has shown significant relations to MetS, along with MetS-related factors like adiponectin, HOMA-IR, IL-6, and hs-CRP. Recently, attention has been focused on methods to prevent the onset of diseases via controlling them before the overt onset stage by predicting MetS in healthy adults. In this respect, we carefully suggest the possibility of using the BAP test as a predictive marker of MetS, as well as related cardiovascular diseases, as it shows some associations with other factors, including insulin resistance, adiponectin and hs-CRP, which are known to be related to MetS as well as cardiovascular diseases. Further long-term large-scale randomized clinical trials are needed to identify the usefulness of the BAP test as a predictor of MetS or MetS-related cardiovascular disease.
KEY MESSAGE
1. Oxidative stress plays a critical role in the development of metabolic syndrome (MetS) and increases the risk of cardiovascular complications of MetS.
2. The biological antioxidant potential test representing antioxidant capacity has shown significant relations to MetS, along with MetS-related factors like adiponectin, homeostatic model assessment for insulin resistance, interleukin-6, and high-sensitivity C-reactive protein.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





