


INTRODUCTION
Percutaneous coronary intervention (PCI) is an established treatment in patients with obstructive coronary artery disease [1]. The use of drug-eluting stents (DESs) has resulted in a marked reduction in in-stent restenosis compared with bare-metal stents (BMSs) in the treatment of coronary artery disease [2,3]. Despite the beneficial effects of DES on restenosis, coronary endothelial dysfunction has been observed in areas adjacent to the DES implant site after an average of 6 months following PCI, whereas this is not the case with BMSs [4,5,6].
The improved epicardial endothelial function obtained over the shorter term in patients with an implanted stent is well known, but studies on coronary microvascular function after PCI are lacking. One recent study reported that microcirculatory function was not significantly different between patients with DESs and those with BMSs [7].
The genous endothelial progenitor cell (EPC) capturing stent (Orbus Neich Medical Technologies, Fort Lauderdale, FL, USA) is coated with anti-human CD34 antibodies that bind circulating endothelial progenitor cells from the peripheral blood to the stent surface. In an animal model, scanning electron microscopy demonstrated complete re-endothelialization of the stent struts and vessel segments within only a few hours following Genous stent placement [8]. The captured EPCs are thought to rapidly differentiate to form a functional endothelial layer on the stent surface, resulting in better results in terms of improved microvascular function than obtained with DESs.
The aim of this study was to evaluate coronary microvascular vascular function in patients receiving EPC stents and in those receiving DESs.
METHODS
Study population
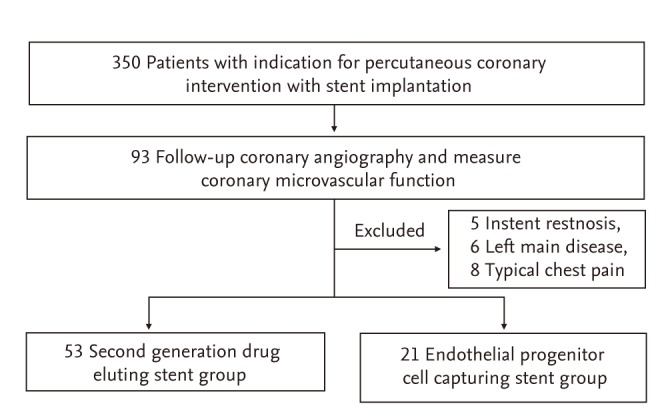
From May 2010 to September 2012, patients undergoing stent implantation for the treatment of significant de novo stenosis of the coronary artery were evaluated for study enrollment. Follow-up coronary angiography was performed 6 to 12 months after the initial PCI. Coronary microvascular function was assessed only in patients who showed no angiographic in-stent restenosis and no recurrent typical chest pain during the follow-up period (Fig. 1). From this group, 74 patients were included in the study and then further classified into two groups according to the type of stent implanted: the EPC stent (n = 21) or a second-generation DES (n = 53).
Exclusion criteria were bypass graft lesion and previous PCI for the target vessel. Patients in whom in-stent restenosis was seen on follow-up angiography or who experienced recurrent chest pain during the follow-up period were also excluded. The study was approved by the Institutional Review Board of our institution and all participants provided written informed consent.
Study design
The initial PCI was performed according to standard guidelines. The 53 patients in the DES group received the zotarolimus-eluting stent (Endeavor stent, Medtronic Vascular, Santa Rosa, CA, USA) or the everolimus-eluting stent (Xience stent, Abbott Vascular, Santa Clara, CA, USA). The 21 patients in the EPC stent group patients received the Genous stent. The optimal medical treatment for all patients was strongly recommended before and after the initial PCI. All patients were administered 100 mg of oral aspirin daily and 75 mg of clopidogrel or another antiplatelet agent daily if clinically indicated. During the follow-up period, the patients also received oral β-blockers, angiotensin receptor blockers, lipid-lowering therapy, and vasodilators, unless contraindicated.
Follow-up coronary angiography was performed 6 months after the initial PCI. A 6-Fr guiding catheter was used to evaluate the coronary arteries of all patients. In patients on medications with potential effects on vasomotor responses, treatment was discontinued at least 72 hours prior to the follow-up angiography.
Assessment of coronary microvascular function
The index of microvascular resistance (IMR) and the coronary flow reserve (CFR) were used to assess coronary microvascular function [9,10] together with the fractional flow reserve (FFR). Intracoronary pressure parameters were measured in each patient after PCI using previously described methods [11].
Using commercially available software (Radi Medical Systems, Uppslae, Sweden), the shaft of the pressure wire acts as a proximal thermistor, and the sensor located near the tip of the wire as a distal thermistor, such that pressure and temperature can be measured simultaneously. The thermodilution technique was used to determine the transit time of room-temperature saline injected into the coronary arteries [12]. The saline solution was injected in 3-mL aliquots into the designated coronary artery, and the resting mean transit time (baseline mean transit time, bTmn) was measured. Steady-state maximal hyperemia was induced by the intravenous infusion of adenosine (140 µg/kg/min). The hyperemic mean transit time (hTmn) was measured by injecting three additional 3-mL aliquots of room-temperature saline into the same coronary artery. Mean aortic pressure (Pa, measured by the guiding catheter) and mean distal coronary pressure (Pd, measured by the pressure wire) were simultaneously measured during both the resting state and the maximal hyperemic state.
CFR was calculated by dividing the resting hTmn by the bTmn. The IMR was defined as the simultaneously measured distal coronary pressure divided by the inverse of the hTmn.
Statistical methods
All statistical analyses were performed using SPSS version 11.0 (SPSS Inc., Chicago, IL, USA). For continuous variables, differences between groups were evaluated using an unpaired t test or the Mann-Whitney rank-sum test. For discrete variables, differences were expressed as counts and percentages and analyzed with using the chi-square test or Fisher exact test between groups as appropriate. Multivariate logistic regression analysis was used to assess the independent impact of variables on microvascular function. A two-tailed p value of 0.05 was considered to indicate statistical significance.
RESULTS
Baseline clinical characteristics
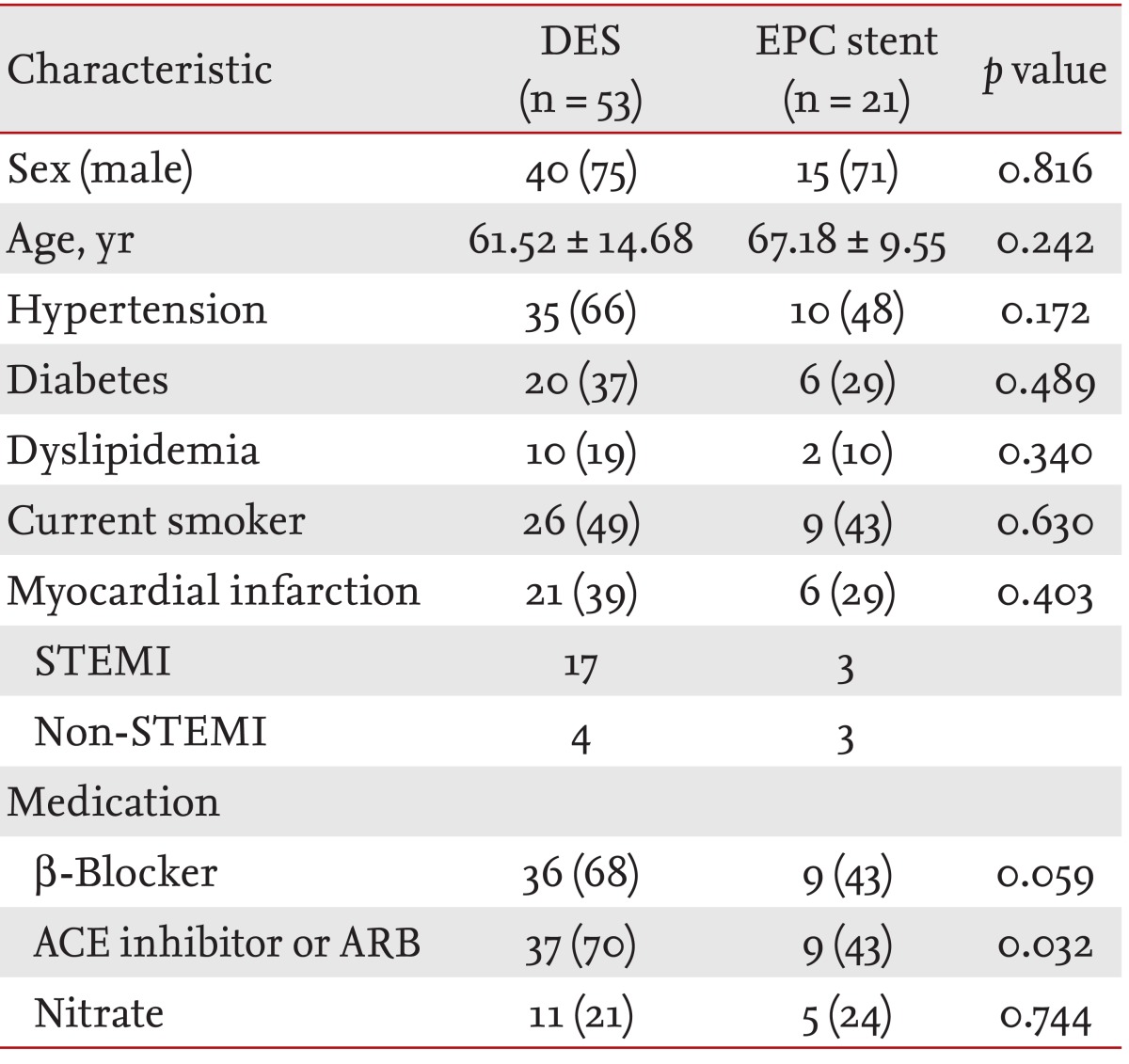
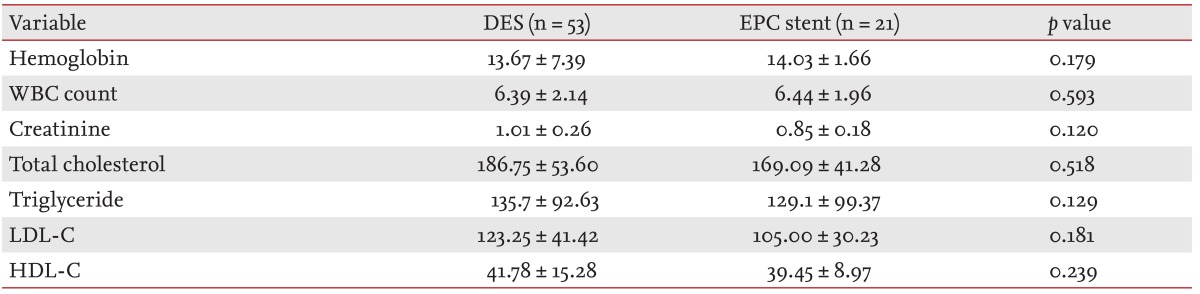
The baseline clinical characteristics of the patients included in the study are shown in Table 1. The ages of the patients and the prevalence of diabetes mellitus, hypertension, hyperlipidemia, and myocardial infarction were similar in the two groups. The two groups did not significantly differ with respect to medications, except renin-angiotensin-aldosterone system inhibitors, or in total cholesterol, triglyceride, and low and high density lipoprotein cholesterol levels (Table 2).
Coronary angiographic characteristics and microvascular function
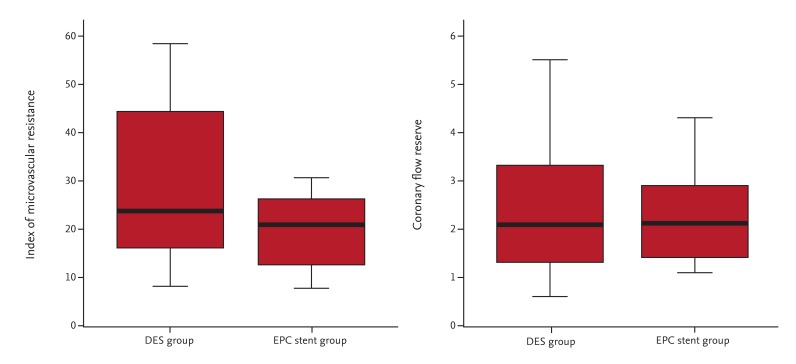
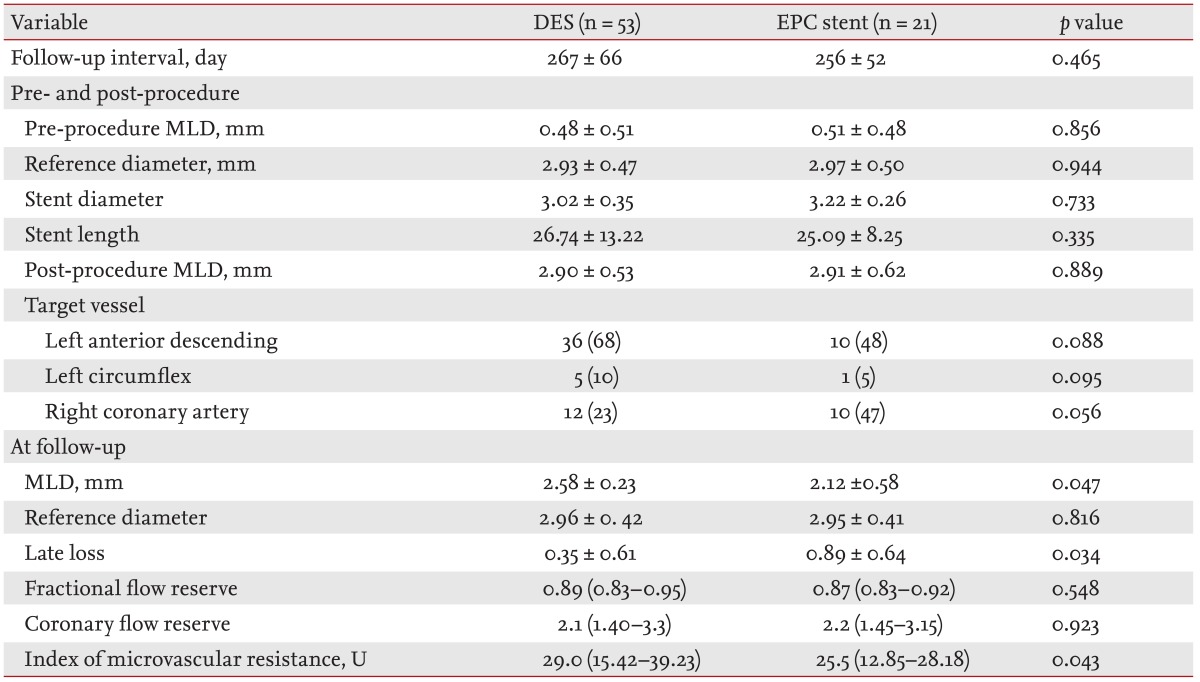
The angiographic parameters and the results of the microvascular function tests are shown in Table 3. The mean interval from the initial PCI to follow-up angiography was similar between the two groups: 267 ± 66 days for the EPC stent group and 256 ± 52 days for the DES group (p = 0.465). Their angiographic characteristics were also comparable, as were the diameters of the stents implanted in each patient and the mean total stent length. However, late loss of lumen diameter (measured at baseline and at 6 months) was significantly higher in the EPC stent group than in the second-generation DES group (0.89 ± 0.64 mm vs. 0.35 ± 0.61 mm, p = 0.034). Fig. 2 provides a comparison of the CFR and IMR values of the two groups. CFR and FFR were not significantly different (median, 2.1 [interquartile range (IQR), 1.40 to 3.3] vs. median, 2.2 [IQR, 1.45 to 3.15], p = 0.923; and median, 0.89 [IQR, 0.83 to 0.95] vs. median, 0.87 [IQR, 0.83 to 0.92], p = 0.548, respectively). IMR was significantly lower in the EPC stent group than in the DES group (median, 25.5 [IQR, 12.85 to 28.18] vs. median, 29.0 [IQR, 15.42 to 39.23], p = 0.043). The range of IMR was greater, with higher levels, in the DES group than in the EPC stent group.
Predictors of microvascular function after PCI
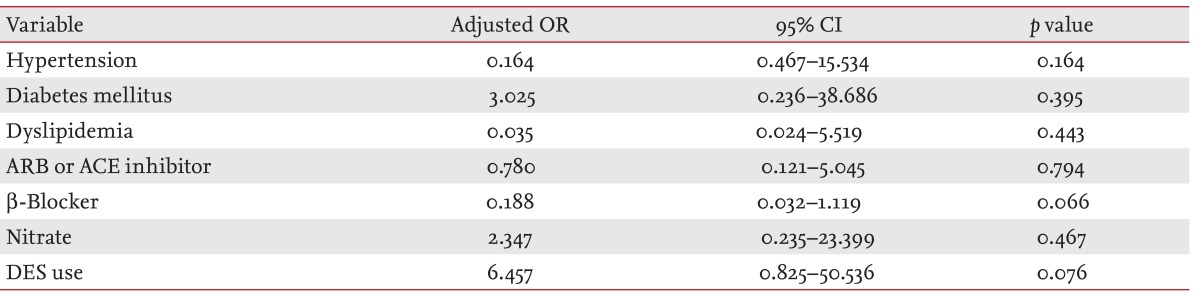
Multivariate logistic regression analysis was performed to determine the independent predictors of microvascular dysfunction after PCI. As a point of reference, in a previous study that included patients with stable coronary disease and no obvious microvascular dysfunction, the mean IMR was 22 [13]. Unfortunately, in our patient population, there were no independent predictors of an IMR after PCI that was < 22. However, the use of a β-blocker and implantation with an EPC stent showed a trend toward being predictive for this target value (Table 4).
DISCUSSION
To our knowledge, ours is the first study to compare coronary microvascular function in patients with a second-generation DES versus an EPC stent. Although the effect of stents, and DES in particular, on epicardial endothelial function has been investigated, changes in the downstream microvasculature following stent implantation have yet to be evaluated, despite the fact that the coronary microcirculation is crucial for myocardial blood flow and myocardial perfusion regulation [14,15]. In a previous study [7], microvascular function did not differ between patients who received a DES and those who received a BMS.
The difference between the results obtained in a comparison of drug-eluting versus BMSs [7] and our own findings in patients with DES versus EPC stents can be explained as follows. First, the stents used in this study were different than those evaluated in a previous study [7]. Here we compared the EPC stent with two second-generation DESs. The latter are associated with excessive inhibition of vascular cell proliferation, which may lead to rare but serious complications such as late incomplete stent apposition, aneurysm formation, and late or very late stent thrombosis due to impaired re-endothelialization [16]. The recruitment of EPCs to the site of vascular injury may promote vascular healing and has been shown to inhibit neointimal proliferation and restenosis associated with PCI [17], which in turn should have favorable effects on coronary endothelial and microvascular functions. Second, there was a difference in the measurement of microvascular function, as in this study we principally used IMR not CFR. IMR, because it is independent of hemodynamic perturbation and of the hemodynamic state, provides a more reproducible assessment of the microcirculation than CFR [10], which is highly sensitive to hemodynamic changes. Further investigation is needed to clarify the relationship between stent type and microvascular function and between the EPC stent and DESs.
Unlike in previous studies, in our study there was no independent predictor of microvascular dysfunction after PCI [18,19,20]. For example, in several reports, IMR was shown to be a significant predictor of the recovery of left ventricular function after myocardial infarction with ST elevation [18,19,20]. Whether a larger study population or restricting the study population to patients with previous myocardial infarction would have changed our results is unclear.
This study had several limitations. First, the population studied was relatively small. Second, we did not measure endothelial and microvascular function simultaneously, although endothelium-dependent epicardial function may affect microvascular function. However, this would have necessitated studies with acetylcholine, which in South Korea cannot be legally imported for human use. Third, patients with in-stent restenosis were excluded. Consistent with the results of other studies [21,22], late loss of lumen diameter was significantly more frequent in our EPC stent group, which in turn suggests greater re-vascularization of the target lesion in these patients. However, because of the controversy regarding the effect of epicardial-artery occlusion during measurement of microvascular resistance in the determination of IMR, patients with in-stent restenosis were excluded from our study. Fourth, we did not measure microvascular function at index PCI, such that changes in microvascular function after PCI could not be evaluated. However, we considered microvascular function to be more important during the stable state than during the acute state. Fifth, although the distance of the pressure wire along the length of the vessel will impact measurements of hyperemic transit time and the IMR, we did not determine the variability of IMR as a function of the distance of the wire within the vessel. Lastly, because this was an observational study, it was susceptible to residual bias due to unmeasured confounding factors.
KEY MESSAGE
Coronary microvascular function was better in patients receiving an endothelial progenitor cell (EPC) capturing stent than in patients receiving drug-eluting stents (DESs) at 6 months after percutaneous coronary intervention. However, both late loss of lumen diameter and target-vessel revascularization were unfavorable in the EPC stent group compared to the DES group.
The complete re-endothelialization achieved with the EPC stent confers beneficial effects, especially in patients with microvascular dysfunction.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





