


To the Editor,
Liposarcoma, a neoplasm of mesenchymal origin derived from adipose tissue, is one of the most common soft tissue sarcomas. Liposarcoma is usually located in the lower limbs of adults, and retroperitoneal tumors are uncommon [1]. It very rarely presents in the gastrointestinal tract and even less frequently in the colon [2]. Despite the potential involvement of the gastrointestinal tract, the precise location of secondary colonic tumor development has not been described yet. Herein, we report a case of colonic liposarcoma in a patient who had previously been diagnosed with retroperitoneal liposarcoma.
A 73-year-old male presented with a 3-week history of abdominal pain. Fifteen years prior, he had been diagnosed with liposarcoma in the retroperitoneal area adjacent to the right kidney. At that time, he underwent wide resection of the mass, including a right nephrectomy. The retroperitoneal mass weighed 1,440 g and measured 23 × 15 × 7 cm in dimension at initial submission. The external surface was lobulated and well-capsulated, and the cut surface revealed a highly myxoid appearance with focal hemorrhages. The renal capsule of the right kidney was adhesive to the retroperitoneal mass, and tumor cells had infiltrated the perirenal fat tissue; however, the kidney and renal pelvis were free from tumor extension. Tumor cells were mostly spindle cells, but occasional bizarre nuclei and very rare mitotic figures (less than 1/10 high power field) were also observed. The histological diagnosis was a myxoid-type liposarcoma, and the tumor was determined to be of histological grade 1, according to the French Federation of Cancer Centers Sarcoma Group grading system (FNCLCC). The patient received post-operative radiotherapy (4,500 cGy) in the involved field. Surveillance checkups by computed tomography (CT) scan were performed over 9 years, with no consequent evidence of recurrence. The patient did well for 15 years after the first operation. Clinical data were obtained from the patient's hospital records and from communications with attending physicians.
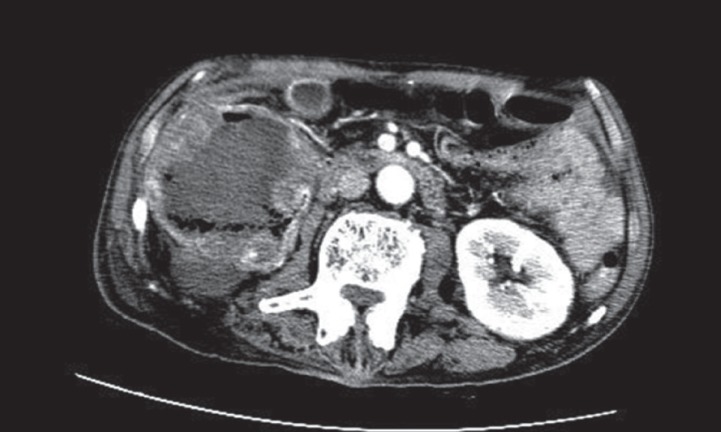
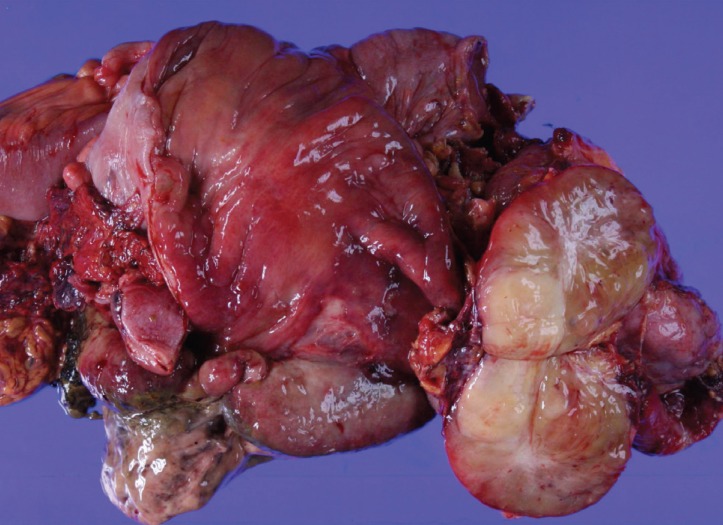
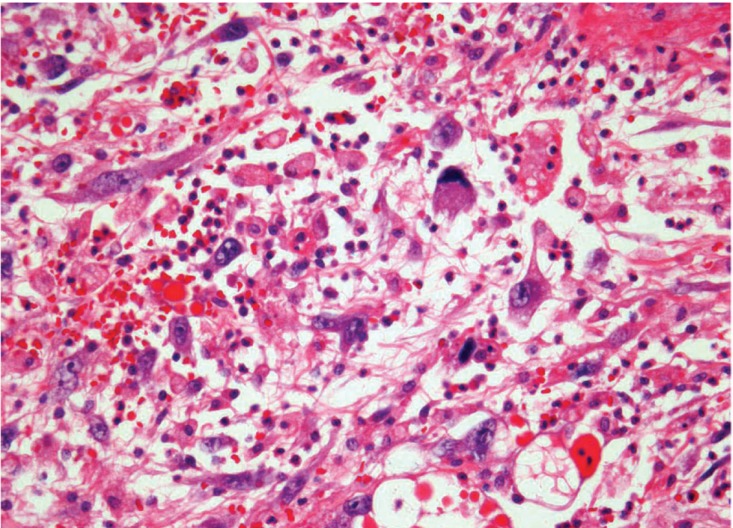
At the time of presentation with abdominal pain, physical examination on admission revealed a large, soft, tender mass, palpable in the right lower quadrant of the abdomen. A preoperative CT scan on admission showed a large, homogenous, smoothly outlined, low-attenuation tumor mass in the pelvis, close to the ascending colon (Fig. 1). Laboratory data on admission were unremarkable. Tumor markers including carcinoembryonic antigen, carbohydrate antigen 19-9 (CA 19-9), and CA-125 were within normal limits. The patient underwent a right hemicolectomy. The tumor was situated in the subserosa of the ascending colon and ileum, showing well-defined borders. Gross findings of the specimen revealed multiple yellowish capsulated masses measuring up to 12 × 11 × 5 cm. Two ulcerated lesions involving the tumor (meaning is unclear) were observed in the colonic mucosa (Fig. 2). There were no enlarged lymph nodes in the colonic mesentery. Neither ascites nor peritoneal dissemination were observed. Hematoxylin and eosin stained histological sections 4 µm in thickness were examined per centimeter of tumor diameter. Microscopic findings included large pleomorphic cells, highly vacuolated and lipid-rich cells, and lipoblasts. There was no evidence of tumor necrosis, vascular invasion, or lymph node metastases in the colonic mesentery. These findings were consistent with pleomorphic liposarcoma (Fig. 3), and the tumor was determined to be of histological grade 2, according to the FNCLCC system. Doxorubicin-based adjuvant chemotherapy was administered to the patient, who had no evidence of disease 2 years postoperation.
From a histopathological point of view, liposarcoma can be divided into three principal groups according to subtype, based on morphological features and cytogenetic aberrations: (1) atypical lipomatous tumor/well-differentiated liposarcoma (ALT/WD) and dedifferentiated liposarcoma; (2) myxoid-round cell liposarcoma; and (3) pleomorphic liposarcoma [1]. Clinical behavior has been shown to correlate with histological subtyping. ALT/WD liposarcoma is a locally aggressive, nonmetastasizing tumor with the most favorable outcome; 5-year survival rates are estimated to be 75% to 100%. Dedifferentiated liposarcoma is defined as an ALT/WD liposarcoma and has similar local effects; although it metastasizes systemically, its clinical behavior is less aggressive than that of other high-grade pleomorphic sarcomas. The 5-year survival probability for this subtype is 75%. Myxoid-round cell liposarcoma represents a morphological continuum; for this subtype, histological grading is based on the proportion of round cell component. Pure myxoid lesions are generally considered to be low-grade and are associated with a 5-year survival rate of 90%; however, a high histological grade myxoid lesion, which is often defined by greater than 5% round cell component, is a predictor of worse outcome, with a 5-year survival rate of 50%. Pleomorphic liposarcoma, the least common subtype, is associated with the worst prognosis, with a 5-year survival rate of 30% to 50%. Clinically, its behavior is similar to that of high-grade sarcoma, i.e., it metastasizes frequently, most commonly to the lungs. Pleomorphic liposarcoma can be characterized morphologically by the presence of sheets of pleomorphic lipoblasts, which contain enlarged and hyperchromatic nuclei, scalloped by cytoplasmic vacuoles [3].
The anatomical distribution of the various liposarcoma subtypes appears to be closely related to their histological type: myxoid-round cell and pleomorphic liposarcoma mostly present in the extremities, whereas ALT/WD and dedifferentiated liposarcoma occur predominantly in the retroperitoneum [1]. A study analyzing 63 cases of pleomorphic liposarcoma reported tumors located in the lower extremity (36.5%), especially the thigh (28.5%), limb girdles (17.5%), upper extremity (16%), thoracoabdominal wall (9.5%), and internal trunk (20.5%) [3]. Although liposarcoma may occur anywhere in the body, including the gastrointestinal tract, occurrence in the colon is extremely rare, with only a few cases cited in the literature [2].
Our report represents the first case of colonic liposarcoma with different histological subtypes after retroperitoneal liposarcoma. The primary tumor was diagnosed as myxoid type at the retroperitoneum, which is an infrequent site. Interestingly, at the second event after the first disease diagnosis, following a 15-year disease-free interval, a different histological type known as the pleomorphic type was observed. The fact that the second tumor was of a different histological subtype suggests the possibility of sequential development of a de novo tumor rather than a recurrence. The 15-year disease-free interval following curative resection also makes it difficult to interpret the second tumor as a recurrence. Recurrence of retroperitoneal liposarcoma tends to occur 6 months to 2 years after resection [4]. Our case is thus considered to be a double primary liposarcoma of the retroperitoneum and the colon; however, we cannot definitively exclude a potential transformation from a myxoid to a pleomorphic type liposarcoma, because of the unknown behavioral characteristics of the tumor. The majority (75%) of primary colon liposarcomas are located in the right colon, which was the case for the patient described here. Most lesions described in publications are voluminous tumors that range in maximum dimension from 4.5 to 31 cm (median, 12) [2].
Guidelines for treatment of liposarcoma have not been well established. Complete wide excision, which has been recommended by most authors, is the most important component of therapy [1]. A study using a prospective database reported that 9 out of 9 (100%) retroperitoneal myxoid liposarcoma patients who underwent complete tumor resection were free from distant recurrence after 10 years, suggesting that the extent of resection remains the most important predictor of survival [5]. The role of adjuvant chemotherapy for liposarcoma has not been determined and is controversial for colonic liposarcoma due to the rarity of this type of disease. Nevertheless, in high-grade tumor types such as pleomorphic liposarcoma, attempts to control the disease have been made using a chemotherapy regimen of doxorubicin or ifosfamide, with some notable survival benefits [3,5].
In summary, we report a unique case who developed colonic pleomorphic liposarcoma 15 years after the curative resection of retroperitoneal myxoid liposarcoma.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





