


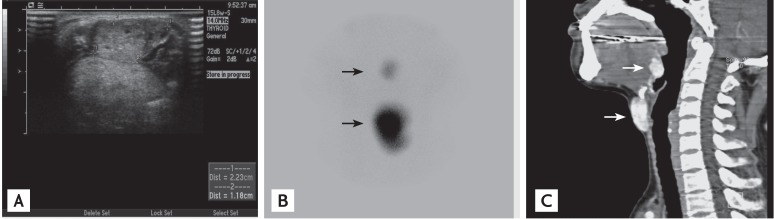
A 34-year-old woman presented with a 2-year history of anterior midline neck swelling. The physical examination revealed a soft, mobile, nontender, 2 ├Ś 1 cm, anterior midline neck mass. Ultrasonography showed a heterogeneously isoechoic mass (2.23 ├Ś 1.18 cm) in the subhyoid region, while a thyroid gland was not seen in the normal position (Fig. 1A). A 99mTc-pertechnetate scan demonstrated two distinct focal areas of radiotracer uptake in the sublingual and subhyoid regions, without uptake in the region of the normal thyroid gland (Fig. 1B). Neck computed tomography (CT) revealed two heterogeneous hyperdense enhancing masses, one in the sublingual region and the other in the subhyoid region (Fig. 1C). The thyroid function tests suggested subclinical hypothyroid status with a T4 level of 4.95 ┬Ąg/dL (normal range, 4.7 to 12.5) and thyroid stimulating hormone level of 15.26 mIU/L (normal range, 0.17 to 4.65). Anti-microsomal antibody and anti-thyroglobulin antibody were negative. A dual ectopic thyroid was diagnosed based on the radiological findings and replacement therapy with levothyroxine was initiated.
Ectopic thyroid tissue is an uncommon congenital aberration resulting from abnormal migration of the thyroid gland. The most frequent ectopic positions of thyroid tissue include the lingual, sublingual, and subhyoid areas. It is very rare for two ectopic foci to be present simultaneously. The mean age of the reported cases with a dual ectopic thyroid was 15 years. Most cases are diagnosed when they are younger than 30 years and are euthyroid or mildly hypothyroid. When assessing an anterior neck mass, it is important to differentiate ectopic thyroid tissue from other causes, such as a thyroglossal duct cyst, lipoma, lymph node, epidermoid cyst, and malignancies, to prevent inappropriate excision. Thyroid scintigraphy, along with either neck CT or ultrasonography, should be considered in cases of anterior midline neck swelling.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





