


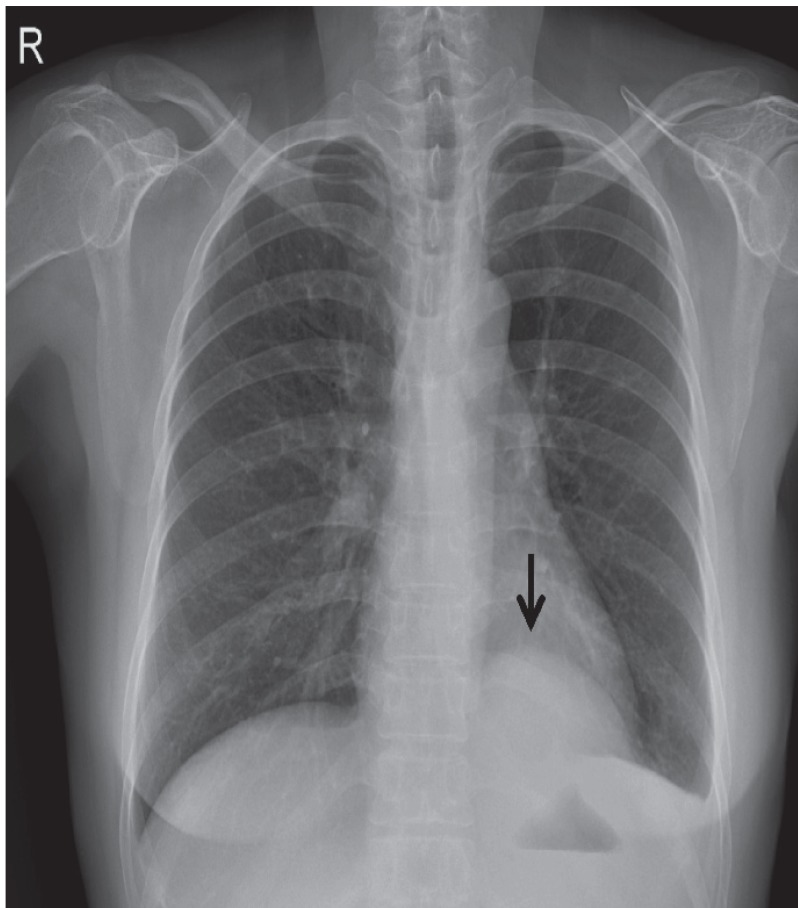
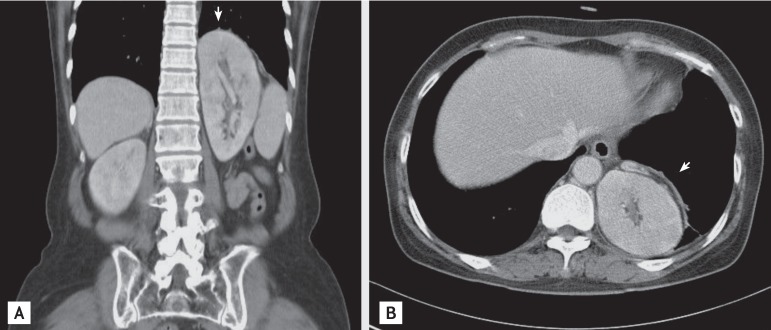
A 56-year-old Korean female attended the emergency department complaining of fever, abdominal pain, difficulty in urinating, and a cough. A physical examination revealed tenderness in the epigastric region with costovertebral angle tenderness and decreased breath sounds in the left lower lung. Initial urine and blood cultures revealed Escherichia coli. A plain chest radiograph showed a mass in the left side of the chest (Fig. 1). An abdominal computed tomography (CT) showed renal enlargement and multifocal decreased attenuation in both renal cortices, which implied acute pyelonephritis. In addition, the CT also showed posterior diaphragmatic hernia with herniation of the upper pole of the left kidney into the thorax, which was posteriorly located, suggestive of a left-sided Bochdalek hernia (Fig. 2). A kidney, ureter, and bladder X-ray radiograph performed immediately after the CT scan showed the left kidney was displaced upwards and a normal flow from the kidneys, through the ureters, to the bladder. Voiding cystourethrogram showed no evidence of vesicoureteral reflux. The patient's condition improved with 14 days of antimicrobial treatment.
An intrathoracic kidney is an extremely rare congenital anomaly. Treatment is necessary for the ectopic kidney if urinary tract obstruction or vesicoureteral reflux is present. Ectopic kidneys show increased incidence of ureteropelvic junction obstruction, vesicoureteral reflux, and multicystic renal dysplasia. Most intrathoracic kidneys are asymptomatic with a benign course, and require no urological intervention. For this reason, most cases are detected unexpectedly, as occurred in this case, and discovered incidentally on a routine chest radiograph, showing mediastinal or lung mass.
Intrathoracic kidneys with Bochdalek hernia have been only rarely reported in Korea. However, the physician's awareness of an intrathoracic kidney in a plain radiograph will assist with early detection, differential diagnosis, adequate diagnostic evaluation, and the therapeutic plan to treat the lung or mediastinal mass. It is emphasized that an intrathoracic kidney should be considered in the differential diagnosis of a mass at the base of the lung on a chest radiograph.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





