


INTRODUCTION
History of three-dimensional echocardiography
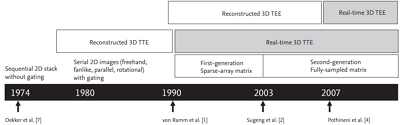
From a historical perspective, three-dimensional (3D) echocardiography was applied clinically after the development of real-time or ŌĆśliveŌĆÖ 3D echocardiography. Real-time 3D echocardiography has existed since 1990 with sparse-array transducers [1]; however, it was not actually performed in real time, requiring a slow rotation of ultrasound probes and complicated processing with relatively low spatial resolution. Since 2000, with fully sampled, higher-resolution matrix-array transducers and the software and hardware to process the information, real-time 3D transthoracic echocardiography (TTE) has been clinically applicable [2,3]. Since 2007, real-time 3D transesophageal echocardiography (TEE) has been performed regularly (Fig. 1) [4-7]. In 2004, we had an opportunity to work with early leading 3D TTE groups at the University of Chicago Medical Center under Professor Roberto Lang and the Mayo Clinic under Professor Jae K. Oh [3,5], and in 2007 we were exposed to the initial model of real-time 3D TEE at the Mayo Clinic in Scottsdale, AZ, under Professor Krishnaswamy Chandrasekaran [6]. Since the late 2000s, real-time 3D TTE and TEE have been evolving in both imaging hardware and analysis software, yielding higher temporal resolution, larger sector angles, and even single-beat, real-time 3D color Doppler. In South Korea, the majority of referral medical centers are capable of real-time 3D echocardiography in their daily clinical practice.
Role of 3D echocardiography in congenital heart disease
Among the clinical applications of real-time 3D echocardiography, that in congenital heart disease (CHD) is promising due to unique projections from the living complex anatomy (such as en face views), true volumetric quantification without geometric assumptions (especially important for complex right ventricle [RV] or functional single ventricle [FSV] assessment), and live dynamic geometric guidance during the interventional procedures [5]. Multidetector computed tomographic (MDCT) imaging or cardiovascular magnetic resonance imaging (CMR) may provide better image resolution and ventricular volume assessment in patients with adult CHD, but the former is limited due to radiation exposure or contrast agents and the latter due to intracardiac devices or coils related to prior CHD interventions or surgeries. Moreover, in contrast to 3D echocardiography, MDCT and CMR require time-consuming off-line processing that is difficult to present in a dynamic, real-time environment for procedural guidance.
At this time, with its spatial and volumetric advantages, 3D echocardiography is an important complement to but not a replacement for routine 2D or Doppler echocardiography. This review discusses the applications of 3D echocardiography in adult CHD not only for de novo or unoperated congenital defects, but also for common late problems following palliative or corrective surgeries in complex congenital defects.
CLINICAL PRESENTATIONS OF ADULT CONGENITAL HEART DISEASE
The incidence of CHD does not differ significantly between countries or over time, and was reported to be 4/1,000 live births in 1941 to 1950 [8] and 8.56/1,000 live births in 1978 [9]. Owing to advancements in fetal echocardiographic detection, neonatal and pediatric care, and surgical techniques, about 85% of children born with congenital cardiac defects survive into adulthood [10]; as a result, adults with CHD outnumber children. Thus, understanding transitional medical care from pediatric to adult internal medicine is essential, and the adult medical provider should characterize the anatomy and physiology of CHD and possible long-term complications, such as heart failure or arrhythmia.
In adults, CHD presents three disease patterns. First, de novo diagnosis of CHD, typically based on complaints of dyspnea or cardiac murmurs due to flaws such as atrial septal defects (ASD), ventricular septal defects (VSD), or patent ductus arteriosus. At this time, de novo diagnosis in adulthood is rarer due to extensive neonatal or pediatric cardiac evaluation; regardless, it is important to decide whether the defects require medical or surgical intervention, and if surgery is indicated, whether it is possible to operate without Eisenmenger syndrome. The second pattern involves patients with a childhood diagnosis without surgical intervention (mostly due to mild CHD) such as small and asymptomatic ASD, VSD, or bicuspid aortic valves without significant functional problems, requiring only observation. The third pattern includes patients who underwent palliative or corrective surgeries during childhood and subsequently have residual lesions that require medical or surgical management in adulthood. CHD, such as ASD or VSD, after closure of the defects does not typically require medication or follow-up in adulthood. However, in cases of complex CHD, clinical and echocardiographic longitudinal follow-up is essential through adulthood: (1) after total correction of the tetralogy of Fallot (TOF), follow-up for pulmonary regurgitation or RV function in adulthood and (2) after the Fontan procedure, in patients with an FSV, surveillance imaging for possible long-term complications such as heart failure, atrioventricular valve regurgitation, intracardiac thrombi, or cardiac arrhythmias is important.
OPTIMAL 3D ECHO IMAGING TECHNIQUE IN ADULT CONGENITAL HEART DISEASE
For clinical 3D echocardiography, commercially available real-time 3D TTE/TEE transducers and ultrasound systems (iE33 or Epiq 7, X3-1 or X5-1/X7-2t, Philips Medical System, Andover, MA, USA; Vivid 7 or E9, 3V or 4V/6VT, GE Healthcare, Wauwatosa, WI, USA; Acuson SC2000, 4Z1c/Z6Ms, Siemens Medical Solution, Mountain View, CA, USA) have been used [11]. Several 3D imaging protocols have been proposed [5,12], but a purpose-driven volumetric acquisition mode with a narrow-angle/high-density and a higher frame rate to maximize both axial and temporal resolution is commonly used. In addition, bi-plane or tri-plane guidance of full-volume (or single beat volume) acquisitions can be used to avoid loss of ventricular walls, leading to optimal off-line analysis of ventricular volume. In principle, a good 2D echo image is the foundation of a good 3D image, so 2D images should be optimized followed by 3D optimization with appropriate gain (echo ŌĆ£drop outŌĆØ with low gain may mimic tissue defects) and compression settings. In addition, any electrocardiogram-gated, full-volume acquisition requires expertise to avoid stitching artifacts [5]. For analysis, on-cart or off-line software is chosen according to the purpose or clinical information related to the specific congenital cardiac defects: en face views for tissue defects (ASD or VSD) and atrioventricular valve regurgitation and 3D volumetric assessment for RV and FSV.
COMMON ADULT CONGENITAL HEART DISEASE
Atrial septa defects
ASDs are one of the most common adult CHDs after bicuspid aortic valves [13]. The American College of Cardiology (ACC)/American Heart Association (AHA) 2008 guidelines recommend ASD closure in patients with RV enlargement, regardless of symptoms (class I) [14]; smaller ASDs (diameter < 5 mm) with no evidence of RV enlargement or pulmonary hypertension do not require closure. The only absolute contraindication for ASD closure is patients with irreversible pulmonary hypertension (pulmonary vascular resistance > 8 Woods units) and no evidence of left-to-right shunting [14]. Routine 2D and Doppler echocardiographic evaluation of the defect itself (location, number, size, flow direction) and associated findings (RV size and function, pulmonary arterial systolic pressure from tricuspid regurgitation velocity, tricuspid regurgitation amount, a cleft mitral valve in primum type, anomalous pulmonary venous return in sinus venosus type) are used to decide whether to perform percutaneous or surgical closure.
In addition, 3D echocardiography has three potential roles in ASD. First, it could provide an en face view of the defect to evaluate the actual types, numbers, size, and shape (which is typically oval, not round), and determine the shortest tissue rims around the defect (Fig. 2A), which is important for multiple ASD device closures and procedural monitoring (Fig. 2B) [15,16]. Among the four types of ASD (secundum, primum, sinus venosus, and coronary sinus), percutaneous transcatheter device closure is feasible only in the secundum type, excluding large defects (> 38 mm diameter) or insufficient (< 5 mm) septal rims; however, a deficient retroaortic rim (anterior rim) is not a contraindication to device closure, requiring careful consideration [17]. Second, 3D echocardiography may provide a better determination of cleft mitral valve in patients with the primum defect (Fig. 2C). Third, it can provide volumetric information for an enlarged RV or geometric details of the dilated tricuspid annulus from the en face view (Fig. 2D), which can be used for concomitant tricuspid annuloplasty during ASD patch closure. The 3D-echocardiography-derived RV global and regional ejection fractions (EF) are also strongly negatively correlated with RV afterload [18].
Ventricular septal defects
Isolated VSD is the most common form of CHD. The incidence of muscular VSD has been reported to be up to 53.2/1,000 live births [19], but accounts for only 10% of adult CHD since 89% of these defects close spontaneously after 1 year [19]. In contrast to complex VSD combined with complex congenital defects in pediatrics, isolated VSD diagnosed in adults is relatively simple with four anatomic types: infundibular VSD (supracristal or subarterial type), membranous VSD (conoventricular, the most common type; about 80%), inlet defects (atrioventricular canal type), and muscular defects. Indications for VSD closure in adults include LV volume overload and a significant pulmonary to systemic flow ratio (Qp/Qs Ōēź 2); contraindications for VSD closure include severe irreversible pulmonary arterial hypertension [13]. Routine 2D and Doppler echocardiographic evaluation of the defect (location, number, size, and flow direction or velocity) and associated findings (LV size or function, pulmonary arterial systolic pressure from VSD shunt velocity, aortic regurgitation, sinus of Valsalva dilatation, double-chambered RV) are important in evaluating and closing the defect.
Three-dimensional echocardiography has a potential diagnostic role in two ways. First, it can provide an en face VSD on the RV septal surface to assess the actual shape and size of the defect, which can be underestimated in routine 2D tomographic views [20,21], and provide information on the relationship to surrounding structures. The appropriate anatomy of the VSD location from the tricuspid and aortic valves with an adequate rim of tissue is important in transcatheter device closure [21,22]. The incremental value of 3D echocardiography over routine 2D techniques has been reported based on the assessment of combined complex lesions such as a sinus of Valsalva rupture or a Gerbode defect [23,24]. Second, 3D volumetric assessment of the LV depicts the consequence of volume overload from the hemodynamically significant VSD shunt.
EbsteinŌĆÖs anomaly
EbsteinŌĆÖs anomaly is a common congenital cause of isolated tricuspid regurgitation in adults, with a prevalence of 0.72/10,000 live births [24]. Accurate classification remains challenging due to substantial anatomical variations: in type A, there is inadequate RV volume; in type B, a large atrialized RV with a mobile anterior leaflet; in type C, restricted anterior leaflet with infundibular obstruction; and in type D, near complete atrialization of the RV [25]. The type or severity varies with the age of presentation [26]. Adult patients with symptomatic EbsteinŌĆÖs are typically mild de novo diagnoses or once-severe childhood diagnoses now dealing with the remaining symptoms or arrhythmias after tricuspid valve repair. The key echocardiographic findings include exaggerated apical displacement of the tricuspid annulus (Ōēź 8 mm/m2) compared with the mitral annulus in an apical four-chamber view and a dysplastic tricuspid valve with RV dysfunction. Since the tri-leaflets are non-planar, identification of individual leaflets from routine 2D TTE is challenging and controversial [27], as is TEE due to the far field location (the higher frequency used in TEE limits deep ultrasound penetration). Three-dimensional echocardiographic evaluation with an en face view, multi-slice or flexi-slice rotational views, or tri-plane with or without color Doppler images increased our understanding of the malformed tricuspid valve (Fig. 3) [28,29] and provided additional information on the morphology and function of tricuspid valves, right ventricular outflow tracts (RVOTs), and pulmonic valves, as well as superior RV volumetric information [30].
Repaired tetralogy of Fallot with pulmonary regurgitation
TOF is one of the most common cyanotic CHD with four anatomic features (VSD, overriding aorta, RVOT obstruction, and RV hypertrophy) and a prevalence of 4.7/10,000 live births [31]. Pulmonary atresia with VSD and major aorta-pulmonary collateral arteries is the most extreme variant of TOF, accounting for approximately one-fifth of such cases [32]. Most patients with TOF undergo intracardiac repair in the first year of life [33]; therefore, adult patients with TOF tend to have repaired TOF. Common chronic postoperative complications in adulthood are pulmonary regurgitation, RV enlargement, RV dysfunction, and arrhythmias [34]. Postoperative echocardiography is recommended annually until the age of 10 and every 2 years through adulthood [35] to identify any residual anatomic and hemodynamic abnormalities, assess their severity, and provide information for clinical decisions.
Multimodality imaging guidelines for patients with repaired TOF have been suggested [35]. Routine 2D and Doppler echocardiography are non-invasive, highly accessible techniques suitable for longitudinal follow-up of repaired TOF, but several limitations should be discussed for RV evaluation. For RV size, diameter > 42 mm at the basal level indicates RV enlargement [36]; unfortunately, the 2D tomographic image plane shows examiner dependence when comparing different planes over time, yielding inaccurate results. For RV functional analysis, a 2D-derived RV EF is not generally recommended because of the numerous geometric assumptions [36]. A 2D fractional area change (FAC) < 35% provides an estimate of RV systolic dysfunction, but not all of the RV is in view. A tricuspid annular plane systolic excursion < 16 mm represents RV longitudinal dysfunction, but decreases after cardiac surgery despite the lack of reduction in RV FAC [37] or 3D RV EF [38]. Therefore, it is not suitable for repaired TOF patients. For serial follow-up, 3D volume rendered optimal 2D planes are preferred over 2D images for comparisons. In addition, 3D echocardiography can contain the entire RV (including the RVOT) and evaluate the true volumetric changes without simplifying geometric assumptions (Fig. 4). The recently developed RV strain analysis from acquired 3D or 4D datasets provides new parameters of RV regional and global function, which integrate deformation in the longitudinal, circumferential, and radial dimensions [39].
Pulmonary valve replacement (PVR) to restore pulmonary valve competence was considered to be a positive approach in a meta-analysis of 3,118 patients from 48 studies to restore RV function [40]. A single center followed 1,014 patients with repaired TOF for 7.3 ┬▒ 6.8 years. PVR was observed in 27.4% of patients at a mean age of 31.4 ┬▒ 16.4 years [41]. Guidelines from the ACC/AHA 2008 [13], Canadian Cardiology Society 2009 [42], and European Society of Cardiology 2010 [43] recommend PVR for severe pulmonary regurgitation and symptoms of decreased exercise tolerance (class I), severe pulmonary regurgitation and moderate to severe RV dysfunction or enlargement, moderate to severe tricuspid regurgitation (class IIa), and severe pulmonary regurgitation with an right ventricle end-diastolic volume index (RVEDVi) > 170 mL/m2 (class IIa). The intervention timing depends on how long PVR could be delayed while attempting to restore optimal RV function.
To determine the optimal timing for PVR, several RV parameters have been proposed. Currently, CMR is the reference standard for RV quantification and the timing of PVR in repaired TOF with pulmonary regurgitation based on pre-operative CMR parameters: Therrien et al. [44] propose PVR if RVEDVi Ōēż 170 mL/m2 or right ventricular end-systolic volume index (RVESVi) Ōēż 85 mL/m2; Oosterhof et al. [45] apply RVEDVi < 160 mL/m2 or RVESVi < 82 mL/m2; Geva et al. [46] recommend RVESVi < 90 mL/m2 since RVESVi may be more sensitive than RVEDVi for success after PVR; and Lee et al. [47] use RVEDVi Ōēż 163 mL/m2 or RVESVi Ōēż 80 mL/m2. Owing to the high accessibility in patients with prior coils or devices, 3D-echocardiography-derived RV volume is used after TOF repair. The 3D RV volume correlates well with the CMR reference but shows slight underestimation [48]. In a majority of unselected patients with complex CHD, 3D RV volume showed fair-to-good accuracy compared with a CMR reference when using commercially available hardware and software [49], and in a single center study with 25 patients with severe pulmonary regurgitation secondary to either pulmonary valvotomy or TOF repair, 3D RV volume was comparable to magnetic resonance imaging [50]. Particularly for patients with repaired TOF, easily accessible, reliable, repeatable quantification of the RV by 3D echo is important to provide appropriate surgical timing to optimize outcomes. Further studies from multiple centers are required to evaluate 3D-echocardiography-derived RV volume indices for timing the PVR in repaired TOF.
Functional single ventricle
The term ŌĆśsingle ventricleŌĆÖ may describe not just one literal, anatomic ventricle but a single hemodynamically functional ventricle, where the description includes a variety of complex CHDs such as hypoplastic left heart syndrome, tricuspid atresia, pulmonary atresia with intact ventricular septum, and double-inlet ventricles. Typical FSV presents as only one well-developed ventricle with a rudimentary additional ventricle < 30% of its normal volume [14]. The Fontan procedure is palliative for complex CHD and not amenable to biventricular repair to direct systemic venous blood and pulmonary circulation bypassing the ventricular mass; the FSV supports only systemic circulation. The most common forms of the Fontan procedure are atriopulmonary connections and the cavopulmonary connection (intra-atrial lateral tunnel, extracardiac conduit) [51]. From a single center study of 1,052 post-Fontan patients, 10-, 20-, and 30-year survival was reported to be 74%, 61%, and 43%, respectively [52]. In adult CHD, patients with FSV are typically post-Fontan patients and follow-up assessment is recommended for long-term post-Fontan complications [52], such as ventricular dysfunction, atrioventricular valve regurgitation, arrhythmia, thromboembolic events, kidney disease, protein-losing enteropathy, and liver disease.
Generally, echocardiographic follow-up for patients with FSV falls into three categories: patency of surgically altered blood flow, single ventricular function, and atrioventricular valve regurgitation (Figs. 5-7). Of these three, quantification of single ventricular size and function remains challenging. Routine 2D echocardiographic measurements of ventricular cavity dimensions, EF, or myocardial strain are not often used to represent the entire FSV size and function due to the unreliable ventricular geometry and regional myocardial variations, such as a rudimentary ventricle. In clinical practice, the serially followed images of M-mode or 2D tomographic views for ventricular dimensions, EF, or FAC are not consistent and are difficult to compare over intervals. Three-dimensional echocardiography can provide a reliable analysis of the entire FSV and hence is useful for serial, longitudinal follow-up with optimal post-processing of the volumetric raw dataset (Fig. 6). Studies have shown that 3D echocardiographic measurements of mass and volume are comparable with those obtained by CMR [53], which tend to underestimate LV volumes but show a good correlation of LV volume and EF compared with CMR in patients with FSV [54]. In addition, ventricular torsion by 3D echo speckle-tracing has been proposed as a novel indicator of single ventricular function [55]. Three-dimensional echocardiography has also been used as a complementary tool for the evaluation of mechanisms and sites of anatomically challenging atrioventricular regurgitation in FSV (Fig. 7) [56].
FUTURE DIRECTIONS
As methods and clinical tools, 3D ultrasound technologies are innovative, providing a higher resolution and higher volume per second (enough to accommodate a subject in a single beat) along with user-friendly software and standardized image acquisition and presentation protocols. In the future, 3D echocardiography is expected to extend its clinical application with 3D or 4D strain, myocardial torsion or deformation [57], and intracavitary flow [58], which increases our understanding of the regional or multi-directional myocardial motion and complex flow hemodynamics.
One fundamental issue of 3D echocardiography is displaying a 3D image on a conventional 2D screen; this will improve in the near future with a variety of technologies used to present a genuinely 3D image, as with recent consumer 3D HDTV and virtual reality glasses. Thus, the technique of 3D imaging is moving from ŌĆ£flatlandŌĆØ to ŌĆ£spacelandŌĆØ [59]. Similarly, with the advent of 3D printing, 3D images can be converted to physical 3D models, which will be clinically useful tools for cardiologists and congenital cardiac surgeons for the planning of interventions or surgery [60,61].
CONCLUSIONS
A growing number of adult CHD patients with complicated cardiac geometries require additional imaging dimensions in clinical practice. Three-dimensional echocardiography is an important complement to routine 2D echocardiography for adult CHD. Current 3D echo techniques provide value with an anatomically correct plane (en face view of tissue defects or valves) and true volumetric information without geometric assumptions (RV or FSV).

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





