


INTRODUCTION
Since chronic obstructive pulmonary disease (COPD) was considered a disease of elderly male smokers, women have been less likely than men to be diagnosed with COPD [1]. However, as the prevalence of smoking in women has steadily increased over time, COPD is being diagnosed more frequently in women than in men especially in high-income countries [2-4]. The prevalence and the morbidity and mortality rates of COPD have steadily increased in women during the past decades [5]. As the COPD mortality rate in men is steeply decreasing, the gender difference in COPD mortality is narrowing [6].
Despite increasing awareness of the burden of COPD in women, knowledge regarding gender differences in COPD is mainly limited to a pattern of gender-specific characteristics [7]. Women with COPD are more likely to be younger and never-smokers [8-10]. Women are more predisposed to small airway disease, while emphysema is reported less frequently in them [11,12]. Some studies have reported a greater prevalence of dyspnea and worse health-related quality of life in women [8,9,13-16], while others have not [17,18]. Comorbidities, including cardiovascular disease, are more frequently associated with COPD in men; osteoporosis, anxiety, and depression, in women [9,13,19].
However, studies investigating gender differences in COPD outcomes, including exacerbations are scarce [7]. Although there were a few post hoc analyses of randomized controlled trials [8,15,20], the rest were cross-sectional or retrospective cohort studies [21,22]. These post hoc analyses reported a higher rate of exacerbations in women than in men. While increased oxidative stress and transforming growth factor β1 signaling regulated by female hormones were proposed as mechanisms underlying the greater susceptibility to COPD in women than in men for a given level of cigarette smoke exposure [23,24], it remains unclear if these proposed biological mechanisms can explain any gender differences in COPD outcomes. Moreover, it was demonstrated that patients with COPD enrolled in these clinical trials differed from real-world patients in terms of gender ratio, lung function, quality of life, and exacerbations: they were predominantly male, with a history of exacerbations in the preceding year, and had worse lung function and quality of life when compared with the real-world patient population [25]. We aimed to evaluate whether COPD outcomes including exacerbations, lung function, and symptoms differ by gender in a prospective, longitudinal study.
METHODS
Patients
We recruited participants from two different prospective cohorts in the Republic of Korea: the Korean Obstructive Lung Disease (KOLD) cohort, recruiting participants at 17 centers since 2005 [26], and the Korean COPD Subgroup Study (KOCOSS; NCT02800499) cohort, recruiting participants at 45 centers since 2011 [27]. Participants were eligible for the present study if they were 40 years or older, had post-bronchodilator forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) less than 0.7, and had a tobacco smoking history of at least 10 pack-years. Participants with a tobacco smoking history of less than 10 pack-years were also included if they had a biomass fuel (firewood or briquette) exposure history of at least 10 years. Participants who were followed up for less than 6 months and those who did not complete baseline information were excluded. The present study was approved by the Institutional Review Board of the Seoul National University Hospital (H-1706-079-859). All participants provided written informed consent and the study was conducted in accordance with the tenets of the Declaration of Helsinki.
Measurement of variables and outcomes
The following clinical data were collected from each cohort: age, gender, body mass index, smoking status, a history of biomass fuel (firewood or briquette) exposure, a history of exacerbations during the previous year, and comorbidities. Biomass fuel exposure was determined by the same questions in both cohorts: “Have you ever burned firewood for cooking or heating for over a year in your lifetime? If yes, how many years have you burned firewood as fuel?” and “Have you ever used briquettes for cooking or heating for over a year in your lifetime? If yes, how many years have you used briquettes as fuel?”
After a baseline visit, patients were followed up every 3 months (the KOLD cohort) or 6 months (the KOCOSS cohort) with detailed interviews. At each visit, all exacerbations were recorded by a study physician or trained nurse. An exacerbation was defined as moderate when any worsening of respiratory symptoms led to treatment with systemic corticosteroids, antibiotics, or both, and severe if it led to a hospital admission or an emergency department visits [28,29].
Participants underwent pre- and post-bronchodilator spirometry at baseline and at least annually thereafter. Symptom scores including the St. George’s respiratory questionnaire for COPD (SGRQ-C) [30], COPD assessment test (CAT) [31], and modified Medical Research Council (mMRC) Questionnaire [32] were recorded at baseline and at least 6-month intervals. The use of drugs, including long-acting muscarinic antagonist (LAMA), long-acting β-agonist (LABA), and inhaled corticosteroid (ICS) at enrollment and medication possession ratios (MPRs) of those drugs during the follow-up period were also recorded.
The main outcome was the incidence of moderate or severe COPD exacerbations. We also assessed the decline in lung function and symptom scores, including the SGRQ-C, CAT, and mMRC Questionnaire.
Statistical analysis
Clinical characteristics were compared between women and men, using the independent samples t test for continuous variables. For categorical variables, either the chi-square test or Fisher’s exact test were used for comparison.
Propensity score matching was applied to compare women with men with similar characteristics. Multivariable logistic regression was used to compute the propensity score for women using the following baseline covariates; age, body mass index, smoking status (never-smoker vs. former smoker vs. current smoker), smoking history (pack-years), biomass fuel exposure history (< 10 years vs. ≥ 10 years vs. unknown), SGRQ-C total score (< 25 vs. ≥ 25 vs. unknown), CAT score (< 10 vs. ≥ 10 vs. unknown), mMRC dyspnea score (< 2 vs. ≥ 2 vs. unknown), exacerbation history during the previous year (yes vs. no vs. unknown), blood eosinophil (≤ 5% vs. > 5% vs. unknown), post-bronchodilator FEV1 (% predicted), post-bronchodilator FVC (% predicted), bronchodilator response of FEV1 (%), and use of LAMA, LABA, or ICS at enrollment. Following this, 1:1 matching was conducted by the nearest neighbor method within a caliper of 0.25 of the propensity score. The incidence rates of moderate or severe exacerbations were compared using the negative binomial regression model. The time to the first moderate or severe exacerbation was analyzed using the Kaplan-Meier method. Changes in post-bronchodilator FEV1 and FVC and symptom scores were analyzed with the use of random-slope and random-intercept mixed linear regression.
A p values less than 0.05 were considered significant. Statistical analyses were performed using the Stata statistical software version 14.2 (StataCorp LP, College Station, TX, USA).
RESULTS
Of the 2022 patients with COPD enrolled in the two cohorts, 618 were excluded (Fig. 1). A total of 89 women and 1,315 men with COPD were analyzed. Table 1 summarizes their clinical characteristics at baseline. Prior to matching, women were observed as more likely to be never-smokers (49.4% vs. 1.7%, p < 0.001) and have biomass fuel exposure history of greater than or equal to 10 years (69.7% vs. 41.0%, p < 0.001). Diabetes mellitus was less prevalent in women (7.0% vs. 16.0%, p = 0.025), whereas gastroesophageal reflux disease (20.0% vs. 12.6%, p = 0.074) and osteoporosis (25.0% vs. 4.9%, p < 0.001) were more prevalent. The mean SGRQ-C total scores (37.5 ± 19.8 vs. 34.7 ± 19.0, p = 0.188), mean CAT scores (16.3 ± 8.9 vs. 15.1 ± 8.0, p = 0.210), and mean mMRC dyspnea scores (1.6 ± 0.9 vs. 1.5 ± 1.0, p = 0.494) were similar in women and men. Compared with men, post-bronchodilator FEV1 was higher in women (65.8% ± 20.7% vs. 58.8% ± 17.9% predicted, p = 0.002). Less wom en than men tended to use LAMA at enrollment (39.3% vs. 53.3%, p = 0.011). After matching (Supplementary Fig. 1), 74 women and 74 men were followed up for a mean period of 2.7 and 3.1 years, respectively. Clinical characteristics of the matched pairs of women and men were comparable (Table 1). The mean MPRs of LAMA (41.7% ± 41.7% vs. 47.7% ± 41.6%, p = 0.382), LABA (55.0 ± 38.8 vs. 63.1 ± 39.4%, p = 0.209), and ICS (44.9% ± 40.0% vs. 54.7% ± 41.3%, p = 0.144) during the follow-up period were not significantly different between women and men.
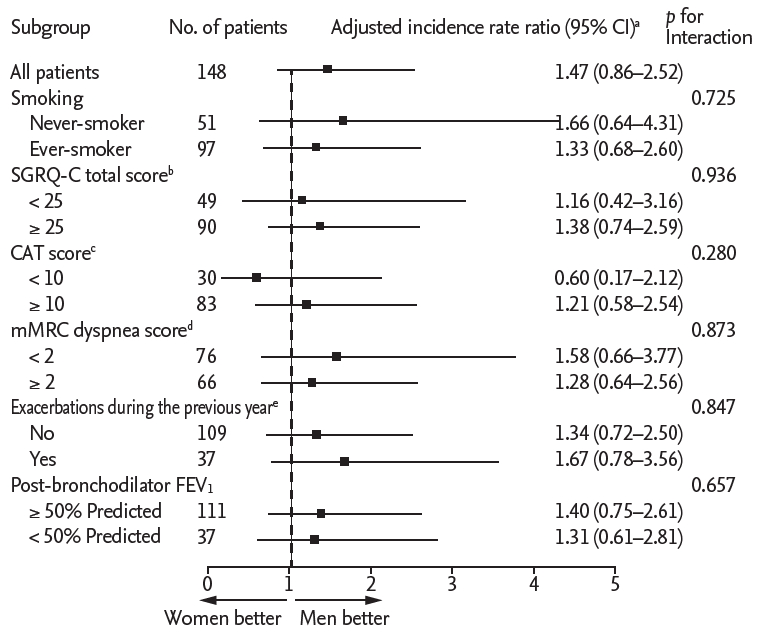
In the propensity score-matched cohort, 33 (44.6%) women experienced 184 episodes of moderate or severe exacerbation, whereas 32 (43.2%) men experienced 107 such episodes during the follow-up period. The incidence rates of exacerbations in women and men were not significantly different (incidence rate ratio, 1.49; 95% confidence interval [CI], 0.88 to 2.54) (Table 2). The difference in the incidence rates were not significant even after adjustment for MPRs of LAMA, LABA, and ICS during the follow-up period (incidence rate ratio, 1.47; 95% CI, 0.86 to 2.52). Furthermore, the time to the first moderate or severe exacerbation did not differ significantly by gender (log-rank p = 0.433) (Fig. 2). Similar results were observed in subgroup analyses of rates of moderate or severe exacerbation (Fig. 3).
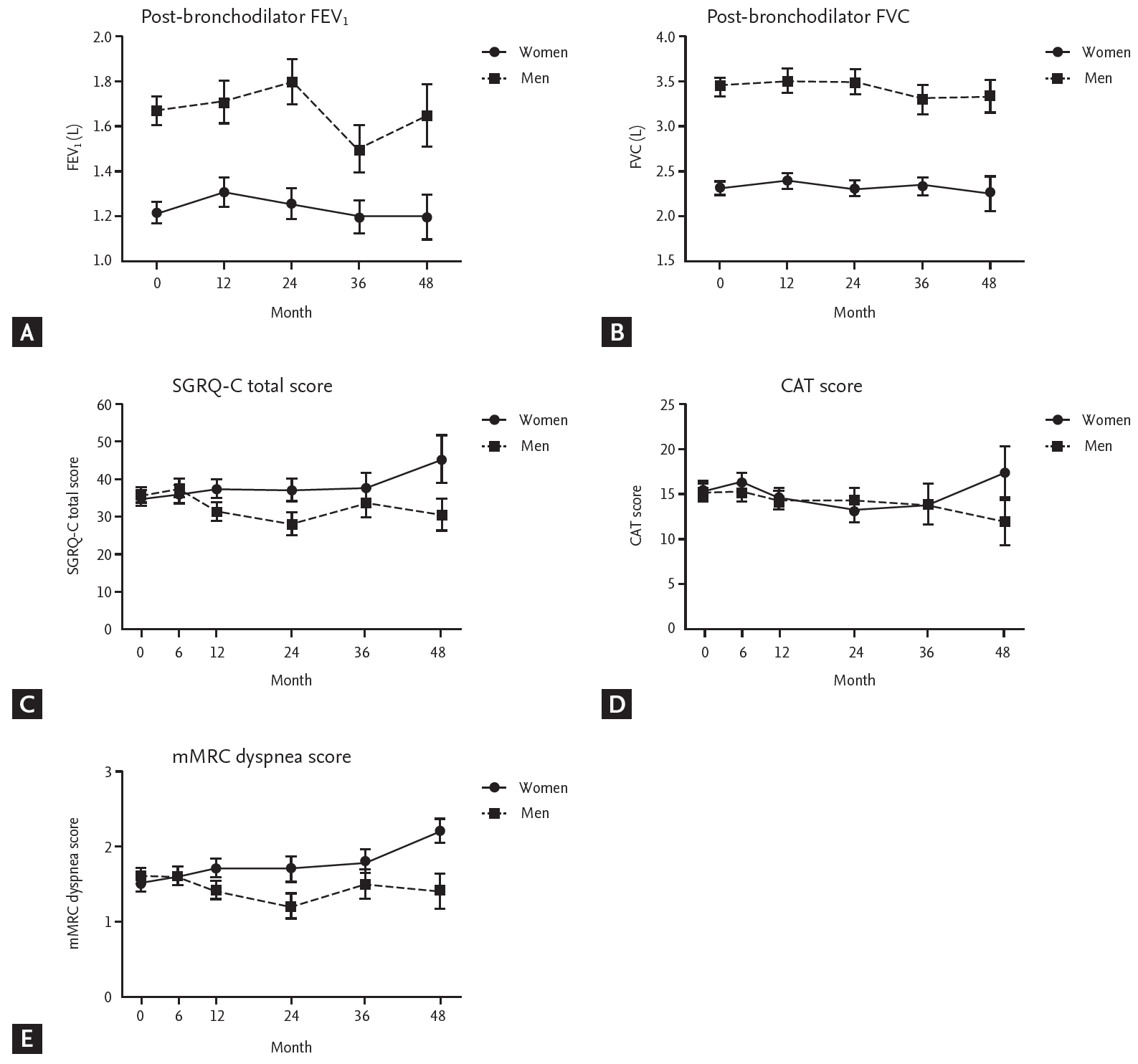
In the propensity score-matched cohort, rates of decline in post-bronchodilator FEV1 and FVC were not different in women and men during 48 months of follow-up (Fig. 4A and 4B). The changes in scores on the SGRQ-C, CAT, and mMRC Questionnaire in women were similar to those in men in the follow-up period (Fig. 4C-4E).
DISCUSSION
We conducted a propensity score-matched analysis in a prospective cohort of patients with COPD to evaluate whether gender has an impact on COPD outcomes including exacerbations, lung function, and symptoms. Our study showed that the incidence rates of exacerbations were not significantly different between women and men, nor were there any gender differences in symptoms and lung function changes during the follow-up period.
There are post hoc analyses of randomized controlled trials reporting that women with COPD experience disease exacerbations more than men with COPD. In a post hoc analysis of the Towards a Revolution in COPD Health (TORCH) trial [33], the time to the first moderate or severe exacerbation was shorter and the rate of exacerbation was reported to be 25% (95% CI, 16% to 34%) higher in women than in men although rates of exacerbations requiring hospitalization were similar in both genders [8]. Data from the Understanding Potential Long-Term Impacts on Function with Tiotropium (UPLIFT) [34] and the Prevention of Exacerbations with Tiotropium in COPD (POET-COPD) trials [35] also reported that women had higher incidence rates of exacerbation than men [15,20]. Although the results of these analyses on exacerbations in women and men were consistent, they may not represent the general COPD population. A validation study of six large pharmaceutically-sponsored COPD studies including TORCH, UPLIFT, and POET-COPD demonstrated that patients with COPD in these studies differed from patients with COPD routinely seen in primary care set-ups in Europe in terms of gender, exacerbations, lung function, and quality of life: they were predominantly male with a history of exacerbations in the preceding year and showed worse lung function and quality of life scores [25]. Patients with COPD were considered eligible for these trials if they had a history of previous exacerbation and/or moderate or severe airflow limitation [33-35]. As a result, the majority (58% to 83%) of patients with COPD in primary care would not qualify as a candidate for inclusion in these trials [25].
In addition, these trials included smokers only. Although tobacco smoking is the most well-studied risk factor for COPD, epidemiologic studies have demonstrated that biomass fuel exposure is under-recognized as a risk factor for COPD [36]. Furthermore, in the randomized controlled trials, although the factors under consideration were balanced between treatment groups by randomization, it cannot be said that they were balanced between genders. In the TORCH trial, women subjects tended to present with worse mMRC dyspnea scores at baseline (20% with 4 or 5 vs. 18%, p < 0.001) and had more exacerbations in the year before the study (59% vs. 56%, p = 0.113) than did men [8]. It is difficult to conclude, however, that these differences in COPD exacerbation are based on gender, without considering the differences in symptoms and the prior history of exacerbation.
Our prospective cohort study recruited participants from the actual clinical setting and was not restricted to including patients with COPD with exposure to tobacco smoke only; we also considered exposure to biomass fuels. Additionally, we attempted to reduce the effects of confounding by applying propensity score matching with covariates including the exposure history to tobacco smoke and biomass fuels, symptom scores, and the history of exacerbations in the preceding year. To our knowledge, our study is the first prospective, gender-specific observational study on moderate or severe COPD exacerbations. Although the Danish longitudinal population study reported gender difference and risk of hospitalization for COPD in 1997, hospitalization was not specified as exacerbations [37]. Available covariates were balanced between women and men in our study. After matching, the rate of exacerbations was slightly but not significantly higher in women than in men.
The prevalence of cigarette smoking among women in Asia is typically lower than that in Western countries. Prior to matching, approximately half of women were never-smokers and less than a quarter were current smokers in the present study (Table 1). After matching, 28.4% of women and 40.5% of men were current smokers, and the average pack-years of smoking were 18.9 and 20.7 in women and men, respectively. In the TORCH and UPLIFT trials, the proportion of current smokers in women (34% to 49%) was higher than that in men (26% to 41%), and the average pack-years of smoking were approximately 40 and 50 in women and men, respectively. Differences in exposures to tobacco smoke and biomass fuels may lead to a difference in rates of COPD exacerbations.
Our study has several limitations, including its observational design. The main limitation is the small number of women with COPD, which may have resulted in insufficient power to detect the differences between women and men. In addition, the introduction of inhaled therapy and choice of medications by physicians could have been gender-biased. Thus, we applied propensity score-matched analysis with available covariates including the use of LAMA, LABA, and ICS at enrollment, and the incidence rate ratio of exacerbations was adjusted for MPRs of drugs during the follow-up period.
In conclusion, there has been limited knowledge regarding the interplay of gender and disease outcomes in patients with COPD. We observed that gender made no difference in the rates of exacerbations in a real-world prospective observational study. It remains to be determined if this holds true in the general COPD population.


 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





