


INTRODUCTION
A world free of tuberculosis (TB) has been humanityŌĆÖs long cherished desire. For decades, TB control programs have focused almost exclusively on infectious TB cases. Active case finding and proper management of active TB should be the top priority for TB control programs. However, it is evident that this strategy alone cannot achieve TB elimination. Despite great efforts, TB is still a major public health threat worldwide, with 10 million new cases and 1.2 million deaths in 2018 [1]. In South Korea, 26,433 new TB cases and 1,816 TB-related deaths were reported in 2018 [2].
Latent tuberculosis infection (LTBI) might be the most important factor for the current uncontrolled TB epidemics. One quarter of the worldŌĆÖs population, approximately 1.7 billion people, is estimated to have LTBI [3]. LTBI is a large reservoir for active TB cases because 5% to 10% of those infected will develop active TB over their lifetime [4]. How can TB elimination be achieved? Multiple modeling studies have consistently suggested the solution to this critical question. TB elimination can be achieved through comprehensive strategies directed toward integrated LTBI management with proper active TB management [5,6].
Programmatic management of LTBI is emerging as a critical component of TB control programs for TB elimination [7]. According to this paradigm shift, there have been many changes and advances in LTBI in the last decade. This paper reviews the recent progress and challenges in the conception, diagnosis, and treatment of LTBI as well as the implementation of LTBI programs in South Korea.
LTBI, AN EVOLVING CONCEPT
LTBI is defined as a state of persistent immune response to stimulation by Mycobacterium tuberculosis antigens with no evidence of clinically manifest active TB [8]. This definition is based on the traditional concept of a binary distinction between latent and active TB. Recently, LTBI has been understood as a dynamic and continuous spectrum of TB, resulting from the dynamic interaction between the host immune system and TB bacilli [9]. Recent researches suggest new insight on latency, which is dynamic spectrum of TB infection; elimination of M. tuberculosis, controlled infection with nonreplicating but viable M. tuberculosis, replicating M. tuberculosis at subclinical level, and actively replicating M. tuberculosis [9,10]. New insight on LTBI has led to renewed interest in the ŌĆśincipientŌĆÖ phase of TB [11]. Incipient TB is defined as an infection with viable M. tuberculosis bacteria that is likely to progress to active TB but has not yet induced clinical symptoms, radiographic abnormalities, or microbiologic evidence consistent with active TB disease [12]. Therefore, patients with incipient TB who are very likely to progress to active TB shortly would be an attractive target group with the greatest benefit for LTBI treatment [13]. A better understanding of incipient TB would accelerate the development of more predictive diagnostic tests and effective therapeutic interventions for LTBI.
DIAGNOSIS, NEW TESTS
The tuberculin skin test (TST) and interferon gamma release assays (IGRAs) are the main diagnostic tests for LTBI. Both are indirect tests based on immune response to TB and do not directly assess the presence or viability of TB bacilli. Both tests cannot differentiate between various stages of TB infection, and thus have a poor positive predictive value (PPV) to predict progression to active TB [14,15]. This leads to a high number of individuals who would need to be treated in order to prevent one case of active TB [16]. In a meta-analysis, the pooled PPV of the TST to predict active TB within 2 years was 1┬Ę5% and the number needed to treat (NNT) in order to prevent one TB case was 67.39; IGRAs performed slightly better, with a PPV of 2.7% and an NNT of 37.3 [17]. Due to the limitations of currently available tests, many individuals could not avoid unnecessary treatment and thus, face the potential risk of adverse events such as hepatotoxicity. New diagnostic tests with high predictive value to predict progression to active TB are urgently needed.
QuantiFERON-TB Plus
QuantiFERON-TB Plus (QFT-Plus) is the new version of the QFT-Gold In-Tube. Compared to the QFT-Gold In-Tube containing antigens optimized to stimulate CD4+ T cells, QFT-Plus contains new antigens optimized for both CD4+ and CD8+ T cell stimulation [18]. QFT-Plus has potential to indicate recent infection and disease activity. A recent meta-analysis has revealed that QFT-Plus is a more sensitive test compared to QFTGIT for detecting M. tuberculosis infection [19].
C-Tb test
The C-Tb test is a recently developed skin test utilizing early secreted antigenic target 6 (ESAT-6) and culture filtrate protein 10 (CFP-10) antigens. The C-Tb test is as simple as conducting a TST but has a higher specificity. In several phase III trials of C-Tb [20,21], C-Tb positivity using a 5-mm cutoff correlated with exposure risk, performed better than TST in Bacillus CalmetteŌĆō Gu├®rin (BCG)-vaccinated people, and had a high correlation with the results of the QFT-GIT.
Biomarkers for incipient TB
The key purpose of diagnosing LTBI is to identify who is very likely to progress to active TB [22]. Incipient TB is an attractive target for the development of new diagnostics. Host blood transcriptomic mRNA signatures have emerged as a promising platform for discovering biomarkers for incipient TB [23]. Recent studies have shown that transcriptomic signatures can predict the development of active TB [24,25]. These studies analyzed whole blood RNA sequencing data from large cohorts and revealed that some combinations of gene signatures showed a good correlation with the risk for progression to active TB in 6 to 12 months. Further research is needed for its validation and further development as a point-of-care test.
PROGRESS IN TREATMENTS
New shorter regimens
Isoniazid has been the main drug for LTBI treatment during the past decades. However, the 6 to 9 months of isoniazid regimen has shown low acceptance and completion rates due to the long treatment duration and poor tolerability [26,27]. These are the main barriers in the implementation and scale up of the programmatic LTBI treatment.
Recent studies have shown that shorter regimens using rifampicin or rifapentine are as effective as isoniazid-based regimens with higher completion rates and better safety [28-30]. A daily dose of rifampicin for 4 months [28] and 12 weeks of weekly isoniazid and rifapentine [29] were not inferior to 9 months of isoniazid for the prevention of active TB. Both regimens also showed better completion rates and fewer serious adverse events, especially hepatitis. Another much shorter regimen, one month of daily isoniazid and rifapentine [30], was not inferior to 9 months of isoniazid with a higher completion rate. Shorter rifamycin-based regimens may replace 6-9 months of isoniazid, considering better safety and adherence [31].
However, a recent Korean study of a treatment regimen using 12-week of weekly isoniazid and rifapentine showed a higher rate of flu-like symptoms and a 1.8% rate of anaphylaxis, despite a higher completion rate and lesser hepatotoxicity than 3 months of isoniazid and rifampicin [32]. These findings raise concerns that this regimen might not be appropriate for LTBI regimen for the general population in South Korea.
New vaccine
Therapeutic vaccination is a new and promising approach for LTBI treatment. In a phase IIb trial, a candidate vaccine, M72/AS01E, reduced the risk of developing active TB in human immunodeficiency virus (HIV)-negative people with LTBI by 49.7% for 3 years [33]. The overall efficacy of 49.7% is low compared with that of most established vaccines in the treatment of other diseases. However, considering the high prevalence of LTBI worldwide and the limitations of current preventive chemotherapy, a vaccine could have a great impact on TB control. In addition, the vaccine can be expected to work in patients with drug-resistant TB who show the limited effect of preventive chemotherapy.
LTBI IN SOUTH KOREA
Changes in LTBI prevalence
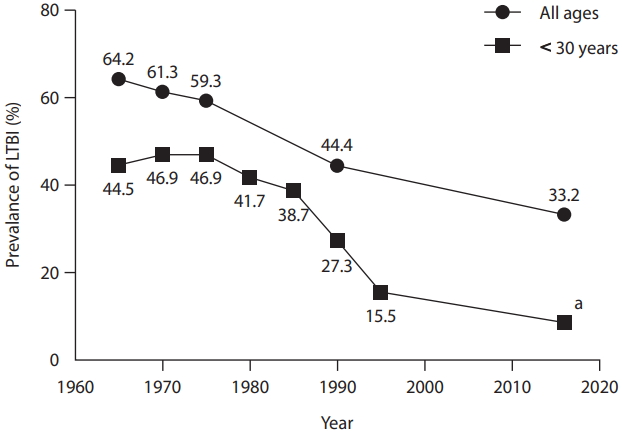
The prevalence of LTBI in Korea has gradually decreased in accordance with a decrease in the prevalence of TB. According to the National Tuberculosis Prevalence Survey, which was conducted every 5 years from 1965 to 1995, the LTBI prevalence in general population decreased from 64.2% in 1965 to 59.3% in 1975 then to 44.4% in 1990 (Fig. 1) [34]. In 2016, the Korea National Health and Nutrition Examination Survey showed an LTBI prevalence of 33.2% [35].
One of the key changes in the LTBI prevalence is its remarkable decrease in the younger population. The LTBI prevalence among those aged < 30 years was 44.5% in 1965, which was decreased to 15.5% in 1995 [36]. Recent studies showed further decrease in the rate of LTBI in the younger population (Table 1). In the 2016 surveillance using TST, the LTBI prevalence was 6.5% and 10.9% in the ages 10 to 19 and 20 to 29, respectively [35], and which was further decreased 2.0% and 3.4%, respectively, in the 2018 surveillance using IGRA [37].
In contrast, the prevalence of LTBI in the elderly population is still high. Many studies in various settings have shown that age is the most important predictor of LTBI [37-39]. To implement and scale up the programmatic management of LTBI in South Korea, the age differences of the LTBI prevalence should be considered.
Progress in the LTBI program
In South Korea, the National Tuberculosis Control policies have focused on early diagnosis and appropriate treatment of patients with active TB [34]. Recently LTBI management has been expanded and integrated into key elements of the National Tuberculosis Control program [34,40]. An LTBI program was started for HIV-infected persons and household contacts under 6 years of age in 2004 [40]. Contact investigation programs were expanded to close contacts under 18 years of age in 2008, and to all age groups in 2011. In 2013, a TB epidemiologic investigation team was established, and active contact investigation was expanded to close contact in congregate settings. In 2016, the Tuberculosis Prevention Act was amended, making TB and latent TB screening mandatory for community workers in congregate settings. By the Tuberculosis Prevention Act, systematic LTBI screening and treatment were conducted for about 1.2 million individuals in congregated settings in 2017 [38].
LTBI management has been recommended as an independent chapter in the 2011 Korean TB guidelines [41]. In the updated 2017 Korean TB guidelines, the age limit for LTBI treatment among close contacts was extended from 35 to 65 years [41]. In addition, screening for and treatment of LTBI in healthcare workers was first recommended.
Challenges
In the past decade, the LTBI program has been expanded and progressed under the vision of ŌĆśTB Free Society, Healthy Country.ŌĆÖ It is time to take a step forward to implement and scale-up programmatic LTBI management. For a programmatic approach, the following challenges need to be addressed; target group selection, treatment-related interventions, monitoring and surveillance system, and an extension plan for vulnerable and hard-to-reach groups.
Prioritization of the target population should be the first step in a national plan for programmatic management of LTBI [8,42]. The most important benefit of LTBI treatment is ŌĆśindividual-level benefit,ŌĆÖ which reduces the risk of developing TB in high-risk individuals. Another key benefit is ŌĆśpublic health-level benefitŌĆÖ which could reduce further transmission of TB in the community [43]. This is an important reason for offering LTBI screening and treatment to workers in congregated settings, including healthcare workers. To achieve TB elimination, a public health approach in LTBI management will be necessary. However, this approach has concerns about increasing the individual risk of harm from unnecessary treatment. In addition, the impact of this approach on overall TB control should be carefully assessed to optimize the allocation of available resources. In 2017, there was a debate about the plan of LTBI mass screening for adults aged 40 and first-grade high school students [44]. The Korean government conducted the proactive LTBI screening and treatment among workers in congregate settings for about 1.2 million individuals in 2017 and 0.5 million individuals in 2018 [37,38]. This project includes several groups not recommended for high-risk groups by the WHO [8]. The achievement and limitation of this project should be carefully reviewed to develop strategies that are optimized for the Korean situation.
Proper management of those identified as LTBI cases is also important. Low acceptance and poor completion rate are the major barriers to implementing programmatic LTBI management [26,27]. In order to increase adherence to LTBI treatment, treatment-related interventions should be accompanied, such as case management, education, and counselling. Appropriate recording, reporting, and monitoring systems should be established.
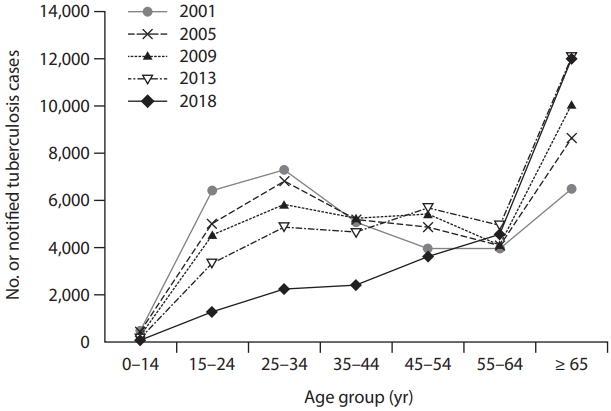
In addition, plans for vulnerable and hard-to-reach groups (i.e., elderly individuals, foreigners residing in Korea [45], North Korean defectors [46], and the homeless) should be explored [47,48]. TB among the elderly population is becoming a major problem in TB control, which accounts for approximately 40% of new TB cases and 78% of TB-related deaths in South Korea. The number of new TB cases in Ōēź 65 years of age has increased consistently with time (Fig. 2). In this group, reactivation from past infection is the major mechanism of developing active TB rather than recent transmission. Despite its theoretical benefit, providing LTBI treatment to individuals Ōēź 65 years is a clinical challenge because of the high risk of age-related adverse events such as hepatotoxicity. Therefore, a tailored approach to LTBI treatment in the elderly population is needed. Active case finding through systemic screening is another approach to managing TB in the elderly [49]. Recently, a pilot project of systematic TB screening in the elderly showed a high rate of TB detection [50].
CONCLUSIONS
LTBI treatment is a paradigm shift in TB control strategies aimed at the elimination of TB. Much progress has been made in the last decade. New insight into LTBI has led to the development of new biomarkers that have the potential to identify the target group that is very likely to progress to active TB. The shorter rifamycin-based regimens have been proven to be effective, safe, and tolerable, which could enhance adherence and completion and minimize adverse events. Along with this progress, to eliminate TB, further effort is needed to implement and expand the programmatic management of LTBI.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print





