


INTRODUCTION
Hepatitis C virus (HCV) infection is a major cause of chronic liver disease worldwide. In addition, chronic hepatitis C (CHC) is associated with liver cirrhosis (LC) and hepatocellular carcinoma (HCC) [1]. Globally, HCC is the fifth most common cancer, and death from HCC ranks second among cancer-related deaths [2]. Therefore, patients with hepatitis C are recommended HCV treatment to prevent LC and further HCC progression.
In the past, the primary HCV treatment was interferon (IFN) therapy, which had poor efficacy and several limitations. In particular, this therapeutic strategy could be used to treat only a subset of patients due to IFN contraindications, such as advanced LC. As direct-acting antiviral (DAA) therapy has become more common, treatment efficacy has increased dramatically, and even patients who were difficult to treat in the past can now be successfully treated [3-5]. However, the use of DAA therapy in CHC patients with HCC is still controversial [6]. Previously, a study using data from the National Veterans Affairs health care system in the United States indicated that the treatment response rate of CHC patients with HCC was lower than that of CHC patients without HCC, but the reported response rate in that study may differ from the actual treatment response rate in Korea. In particular, the enrolled patients in that study had type 1 and type 3 genotypes, while patients in Korea predominantly have type 1 and 2 genotypes [7,8].
Another important issue related to the use of DAA therapy for hepatitis C patients with HCC is HCC occurrence and recurrence. Two previous retrospective studies have hypothesized that DAA therapy may be associated with HCC occurrence and recurrence [9,10]. Although other studies have raised objections to these studies, the benefits of using DAA as a treatment strategy for CHC patients with HCC remain unclear [11-13].
Therefore, we investigated patient responses to DAA therapy and its safety in CHC patients with or without HCC, as well as the HCC recurrence and HCC occurrence after DAA treatment.
METHODS
Study design and setting
In this single-center retrospective cohort study, data on patients who were diagnosed with CHC and started DAA therapy between January 1, 2016, and December 31, 2018, at Konkuk University Medical Center were collected. All enrolled patients were observed for at least 6 months after DAA therapy up to July 31, 2019.
To evaluate the DAA treatment response in CHC patients with or without HCC, patients were divided into two groups: those with HCV-related HCC who achieved that radiologically no viable portion of HCC before DAA therapy and those without HCC before DAA therapy. The patients with no viable portion of HCC, confirmed radiologically, were examined using computed tomography with contrast agent or magnetic resonance imaging with gadoxetic acid (Gd-EOB-DTPA) after treatment to evaluate features such as surgical resection, local ablative therapy, and transarterial chemoembolization. Sustained virologic response at 12 weeks (SVR 12) was defined as undetectable hepatitis C virus ribonucleic acid (HCV-RNA) levels after DAA therapy at 12 weeks. We compared the SVR 12 rate between these two groups.
For subgroup analysis, the HCC group was divided into the HCC recurrence group after DAA therapy and the HCC recurrence-free group. These groups were compared for the associated recurrence risk factor investigation. To analyze HCC occurrence after DAA therapy, patients without HCC before DAA therapy were divided based on HCC occurrence versus HCC-free status after DAA therapy. These groups were compared for related occurrence factor investigations.
The exclusion criteria included patients who were not followed up, those not tested for HCV-RNA at 12 weeks and those who did not complete DAA therapy. This study was approved by the Institutional Review Board of Konkuk University Medical Center (KUH 2019-07-26). Written informed consent by the patients was waived due to a retrospective nature of our study.
Data collection
We collected patient demographics and clinical variables using electronic medical records, including age, sex, body mass index (BMI), DAA regimen, IFN treatment experience, α-fetoprotein (AFP) level, Protein Induced by Vitamin K Absence or Antagonist-II (PIVKA II), serum HCV-RNA level, HCV genotype, Child-Turcotte-Pugh (CTP) score, Model for End-stage Liver Disease (MELD) score, and history of comorbidities. Alcohol drinking was judged to be more than 30 g daily for men and 20 g daily for women. The presence of LC was determined by clinical judgment and imaging studies. Additionally, the liver stiffness measurement (LSM) and fibrosis-4 index (FIB-4) were investigated to further examine the presence of LC. LSM was performed using transient elastography. The FIB-4 index was calculated as follows.
FIB-4 index: age (years) × AST (U/L) / [platelet (109/L) × alanine aminotransferase1/2 (U/L)]
Statistical analysis
We used descriptive statistics to describe the baseline demographics of the patients. To reduce the confounding variables, we used propensity score matching (PSM) in a 2:1 ratio to match patients who have HCV-related HCC and non-HCV-related HCC. The PSM was performed including age, sex, and LC. PSM variables such as LC and age were selected due to their association with HCC. The analyzed data were expressed as medians (Q1, Q3) for continuous variables and numbers with percentages for categorical variables. To compare the two groups, we analyzed using Pearson’s chi-square test or Fisher’s exact test for categorical variables and Mann-Whitney U test for continuous variables. Associated factors of HCC recurrence or occurrence were analyzed using a Firth logistic regression model. Multivariate analysis was performed with variables having a p < 0.05 in univariate analysis. All p < 0.05 were considered statistically significant. All statistical analyzes were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
RESULTS
Characteristics of patients with or without HCC before DAA therapy
Data from a total of 310 patients were collected, and the data from 192 patients were subsequently analyzed after exclusion based on the exclusion criteria (Fig. 1). A total of 54.2% of the patients were female. The HCV genotype of 55.7% of patients was type 1b, that of 42.2% of patients was type 2a, and that of 2.1% of patients was type 2 genotypes, but the subtype could not be specified. Patients who previously received IFN treatment comprised 21.9% and those with LC comprised 34.9% of the analyzed patients. The median follow-up duration of these patients was 704.0 days (IQR, 452.5 to 888.0). The baseline clinical characteristics according to the study group are summarized in Table 1.
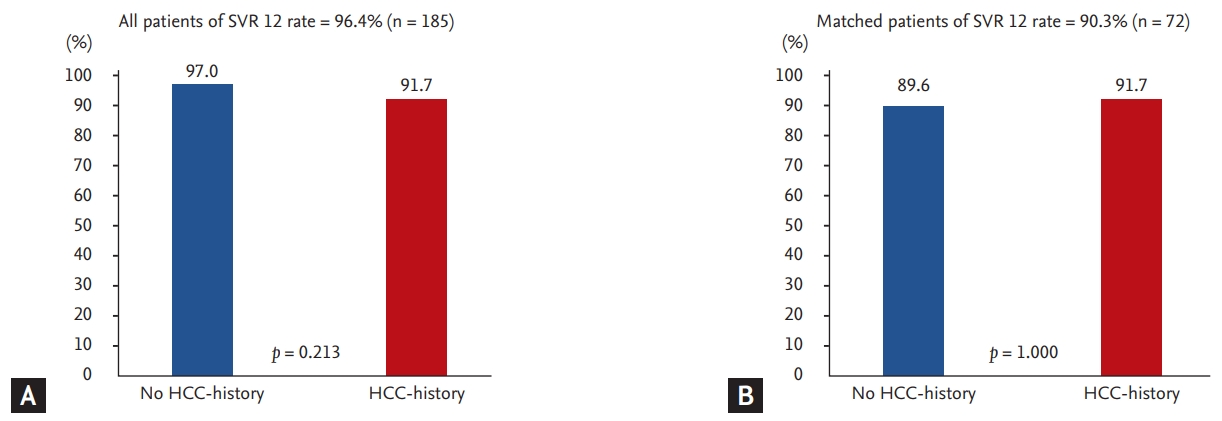
Among the 192 patients, 168 and 24 patients were divided into groups based on their HCC-history before DAA therapy. Patients with a history of HCC before DAA therapy were more likely to be older (57.0 years vs. 72.0 years, p < 0.001) and had a higher incidence of LC (26.2% vs. 95.8%, p < 0.001), higher LSM (7.0 kPa vs. 17.4 kPa, p = 0.012), higher FIB-4 (2.6 vs. 9.2, p < 0.001), and higher AFP (4.4 ng/mL vs. 8.2 ng/mL, p < 0.001). In addition, the DAA regimens used in HCV genotypes 1 and 2 were different between the two groups. In genotype 1, daclatasuvir (DCV) + asunaprevir (ASV) (31.6%) was the most common in the non-HCC group, and sofosbuvir (SOF) + ledipasvir (LDV) + ribavirin (RBV) (16.7%) and DCV + ASV (16.7%) were the most common in the HCC group (p = 0.001). In genotype 2, SOF + RBV was the most common in both groups and was more commonly used in the non-HCC group (43.5% vs. 29.2%, p = 0.018). The SVR 12 rate was 97.0% in the non-HCC-history group and 91.7% in the HCC-history group. There was no significant difference between the two groups (p = 0.213) (Fig. 2).
The PSM results for the baseline characteristics are presented in Table 2. As a result of 2:1 matching, 48 and 24 patients were divided into two groups based on their HCC-history before DAA therapy. Patients with HCC before DAA therapy had a higher incidence of LC (37.5% vs. 95.8%, p < 0.001), higher FIB-4 (3.9 vs. 9.2, p < 0.001), and higher AFP (4.6 ng/mL vs. 8.2 ng/mL, p < 0.001). DAA regimens used in HCV genotype 1 were different between the two groups. DCV + ASV (33.3%) was the most common regimen in the non-HCC group, whereas SOF + LDV + RBV (16.7%) and DCV + ASV (16.7%) were the most common in the HCC group (p = 0.025). In the HCC group, 46 patients (63.9%) were genotype 1 and had a higher incidence of LC (40.0% vs. 93.8%, p = 0.001) (Supplementary Table 1); 26 patients (36.1%) were genotype 2 and had a higher incidence of LC (33.3% vs. 100%, p = 0.002) (Supplementary Table 2) and a relatively higher model for end-stage liver disease with incorporation of serum sodium (MELD-NA) score (p = 0.026) (Supplementary Table 2). The SVR 12 rate was 89.6% in the non-HCC group and 91.7% in the HCC group, though there was no significant difference between the two groups (p = 1.000) (Fig. 2).
Adverse event of HCC-history patients after DAA therapy
Adverse events of DAA therapy are described in Table 3. Eight patients (33.3%) developed adverse events in the HCC group, of which three patients were genotype 1 and five patients were 2. The most common adverse event in the HCC group was anemia, which was defined as hemoglobin < 10 g/dL or decreased hemoglobin > 2 g/dL from baseline hemoglobin (n = 4, 16.7%). In addition, a tingling sensation (n = 2, 8.3%), insomnia (n = 1, 4.2%), and minor adverse events (n = 1, 4.2%), occurred. There were no severe adverse events in either group that would lead to discontinuation of DAA therapy. Additionally, there was no significant difference in the number of adverse events between the groups regardless of the presence of HCC (35.7% vs. 33.3%, p = 0.176). Similarly, PSM results showed no difference in adverse events between the groups (p = 0.858) (Table 2).
Comparison according to HCC recurrence in patients with a history of HCC and associated factors
Fourteen of 24 patients (58.3%) showed cumulative HCC recurrence. The median follow-up duration of the HCC group was 709.5 days (interquartile range [IQR], 539.0 to 815.5), and the total median period after DAA therapy to recurrence was 92.0 days (IQR, 31.0 to 122.0). Specifically, the median period after DAA therapy to recurrence was 92.0 days (IQR, 31.0 to 103.0) in the curative treated HCC group and 101.0 days (IQR, 88.0 to 483.0) in the palliative treated HCC group, and no significant difference was found between the two groups (p = 0.422). Patients with HCC-history before DAA therapy were divided according to the presence of HCC recurrence. A higher number of patients in the HCC recurrence group had a previous experience with IFN treatment (0% vs. 64.3%, p = 0.002) than in the non-recurrence group (Table 4). In the multivariable logistic regression analysis, a statistically significant factor was found for previous IFN treatment (odds ratio [OR], 36.26; 95% confidence interval [CI], 1.51 to 872.74; p = 0.027) (Table 5).
Comparison of HCC occurrence in patients without a history of HCC and associated factors
Five patients were found to have HCC after DAA therapy (3.0%). The time for the median follow-up duration of the non-HCC group was 699.0 days (IQR, 427.5 to 898.5), and the median period after DAA therapy to occurrence was 110.0 days (IQR, 98.0 to 217.0). The HCC occurrence group was relatively older (57.0 years vs. 64.0 years, p = 0.015) and had a higher BMI (23.3 kg/m² vs. 25.9 kg/m², p = 0.027), higher FIB-4 levels (2.5 vs. 5.9, p = 0.009), and higher AFP (4.3 ng/mL vs. 22.9 ng/mL, p = 0.002) than the non-occurrence group. Moreover, the SVR 12 rate of the HCC occurrence group was lower than that the non- HCC occurrence group (98.2% vs. 60.0%, p = 0.007), and the proportion of LC in the HCC occurrence group was relatively high (26.0% vs. 60.0%, p = 0.113) (Table 6). Of the 44 patients with LC, three had HCC, and two of 119 without LC had HCC (6.8% vs. 1.6%, p = 0.219).
PSM results regarding HCC occurrence in without HCC-history patients are presented in Table 6. The HCC occurrence group had a higher BMI (23.4 kg/m² vs. 25.9 kg/m², p = 0.009) and higher AFP (3.8 ng/mL vs. 22.9 ng/mL, p = 0.006).
Age was identified in multivariate analysis as a factor associated with HCC occurrence (OR, 1.12; 95% CI, 1.02 to 1.23; p = 0.021) (Table 5).
DISCUSSION
HCV treatment has become commonplace as DAA therapy has improved the cure rate, and it has become possible to treat patients who had difficulties with IFN treatment in the past. The treatment of HCV patients with a history of HCC is also possible because of DAA therapy. Previous studies have shown that there are several reasons why CHC patients with a history of HCC should be treated. The treatment of CHC in patients with decompensated LC can improve their LC and improve liver function, which can have positive effects [16]. In addition, referring to the literature written in the interferon era, it has been confirmed that hepatitis C treatment can ultimately reduce HCC recurrence [17-19].
Beste et al. [7] found that CHC patients with a history of HCC had lower SVR 12 rates than those without HCC-history (74.4% vs. 91.1%). However, in our study, these groups showed no significant difference in the SVR 12 rate (overall, 91.7% vs. 97.0%, p = 0.213; PSM, 89.6% vs. 91.7%, p = 1.000). There are several reasons to explain this difference. First, the enrolled patient populations have different demographic characteristics. Our study enrolled Asian patients with genotypes 1b and 2a. However, the previous study included many nonhispanic white patients with genotypes 1 and 3. Second, all patients with cirrhosis in this study showed compensated LC, but in the previous study, 31.5% of the enrolled patients showed decompensated LC.
HCC recurrence was observed in 58.3% of patients with HCC. A previous literature review reported HCC recurrence after DAA therapy for CHC with HCC patients, and the cumulative 2-year recurrence rate was 38.9% to 54.5% [20,21]. Compared with these studies, given that the median duration was 704.0 days (IQR, 452.5 to 888.0) in our study, the HCC recurrence rate of our study was similar (58.3% vs. 38.9% to 54.5%). Additionally, the time for the median period after DAA therapy to HCC recurrence was 92.0 days (IQR, 31.0 to 122.0), suggesting that patients who experienced recurrence after DAA therapy were identified in a relatively short period of time.
The HCC recurrence-related factor was previous IFN treatment, and multivariable logistic regression analysis of relevant factors showed the same results (OR, 36.26; 95%, 1.51 to 872.74; p = 0.027). A previous study on the associated factors of HCC recurrence showed that SVR 12 rate, time between the last HCC treatment and DAA therapy initiation, noncurative HCC treatment, more than one HCC treatment before DAA therapy, tumor size, LC, and AFP-L3% were relevant factors [15,20,22]. A recent study reported that patients with previous IFN experience have a high risk of de novo HCC, and the same results were found in our study [23]. As a theory supporting this result, it was estimated that this is due to the immunomodulatory and antitumor properties of IFN rather than antiviral activity alone [24]. However, this issue is controversial and should be evaluated by more studies.
In our study, the cumulative rate of HCC occurrence after DAA therapy was 3.0% in the non-HCC group during the median follow-up duration (699.0 days [IQR, 427.5 to 898.5]). Previous studies have shown that the incidence of HCC after DAA therapy was 4.9% in all patients for 3 years. In addition, patients with LC had a higher occurrence of HCC than those with non-LC (10.0% vs. 2.9%, p < 0.0001) [11]. When comparing previous studies, patients with LC did not have a statistically higher occurrence of HCC than those without LC (6.8% vs. 1.6%, p = 0.219), and the HCC occurrence rate in our study was similar (3.0% vs. 4.9%) to that in other studies.
The PSM results revealed that the HCC occurrence group had a higher BMI and higher AFP than the non-occurrence group. It is well known that the risk of HCC increases with AFP level. BMI is confirmed to be an independent factor in previous studies that have been linked to HCC [25].
The SVR 12 rate was lower in the HCC occurrence group than in the non-HCC group (98.2% vs. 60.0%, p = 0.007). Although the SVR 12 rate was found to be lower in the HCC group, more investigation is needed to determine whether SVR failure is a risk factor for HCC because a relatively small number of patients were enrolled in our study. Additionally, the proportion of cirrhosis in the HCC occurrence of this study is high, but the lack of significant differences between the two groups is probably due to a lack of sufficient numbers (p = 0.113).
The limitations of our study are its relatively small sample size and its single-center retrospective cohort study nature. As a limitation of the small sample size, there were fewer patients with HCC, and thus, the comparisons that can be made are limited. In particular, the difference among DAA regimens could not be evaluated. Moreover, the LC and FIB-4 were not corrected by PSM because the LC and above the 3.25 of FIB-4 in the HCC group was 95.8%, which is a very high rate that could not be statistically matched in the non-HCC group (LC, 37.5% vs. 95.8%, p < 0.001; FIB-4 > 3.25, 61.7% vs. 95.8%, p = 0.005). Despite these limitations, this study is the first report from Korea, and any additional information on the association of DAA therapy with HCC is clinically important and meaningful.
In conclusion, the SVR 12 rate of DAA therapy among CHC patients with or without HCC was not significantly different; the HCC recurrence rate was 58.3% during the median follow-up duration 709.5 days (IQR, 539.0 to 815.5), and the HCC occurrence rate was 3% during the follow-up of 699.0 days (IQR, 427.5 to 898.5). Although DAA therapy in patients with CHC-related HCC was found to be safe and efficacious, HCC recurrence was relatively common. Therefore, HCC in CHC patients should be considered during treatment decisions, and because of the high risk of recurrence, continuous follow-up is required after treatment.
KEY MESSAGE
1. This study evaluated the response and safety of direct-acting antiviral (DAA) therapy in chronic hepatitis C (CHC)-related hepatocellular carcinoma (HCC) patients.
2. The study demonstrated that the sustained virologic response at 12 weeks rate of DAA therapy among CHC patients with or without HCC was not significantly different; the cumulative HCC recurrence rate was 58.3%, and the HCC occurrence rate was 3%.
3. Although DAA therapy in CHC-related HCC patients was found to be safe and efficacious, HCC recurrence was common.

 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Supplement 1
Supplement 1 Print
Print





